
Abstract
Corticosteroid use as an anti-inflammatory agent in infective conjunctivitis has been met with concerns about prolonged infection. This systematic review aims to evaluate the safety and efficacy of corticosteroids as a treatment for infective conjunctivitis. A comprehensive search was conducted on PubMed, Cochrane, Scopus, ScienceDirect, Embase, and ProQuest for clinical trials of topical corticosteroids with or without combination with other medications in bacterial or viral conjunctivitis up to November 2023. The studies were screened, and data on safety and efficacy were extracted. The quality of studies was assessed using the Jadad Scale. Meta-analysis was performed using the random-effects model, with heterogeneity assessed with the I2 statistic. We found ten clinical trials that met the inclusion criteria. Overall meta-analysis revealed significant clinical resolution in dexamethasone-containing therapy compared to non-corticosteroid treatment (OR 1.51; 95% CI 1.19–1.92), with several studies reporting significantly reduced clinical symptoms severity. Two of the six studies assessing viral and bacterial eradication reported significantly improved viral clearance rates. Meta-analysis indicated no difference in ocular adverse effects compared to nonsteroid therapy (OR 1.33; 95% CI 0.82–2.16). In conclusion, corticosteroid use in infective conjunctivitis is relatively safe and may help improve clinical resolution and reduce symptom severity, especially when combined with antibiotics and antiseptics.
Introduction
Conjunctivitis is an inflammation of the conjunctiva caused by infectious or noninfectious causes. 1 Among the various etiologies of infectious conjunctivitis, viral infections are responsible for almost 80% of all cases. 2 The estimated incidence of bacterial conjunctivitis is 135 cases per 10,000 population annually. 3
Corticosteroids are one of the most prescribed medications for ophthalmological disease, not excluding conjunctivitis. Corticosteroid is especially used to treat some specific conditions of conjunctivitis, such as the occurrence of pseudo-membrane or subepithelial infiltrate.4,5
However, current clinical guidelines generally only recommend the use of corticosteroids in noninfective conjunctivitis and viral conjunctivitis. 3 Corticosteroid prescription for infectious conjunctivitis is often considered with caution due to the possibility of corticosteroids causing prolonged infection or reactivation of infection, such as in the case of herpes simplex virus (HSV). 5 The use of corticosteroids is also postulated to prolong viral shedding and increase infectivity. However, these claims were based on animal research,6,7 and recent clinical data show that corticosteroids may be effective and well tolerated, especially combined with anti-infective agents. 5
Given these controversies, this systematic review aims to elaborate on the current discussion and debate surrounding corticosteroids as a treatment option for infective conjunctivitis. To achieve this objective, we conducted a systematic review of evidence for corticosteroids’ efficacy and safety for infective conjunctivitis.
Methods
Search strategy
We searched for all articles in English assessing corticosteroid eye drops in treating conjunctivitis. The search was conducted across six major databases: PubMed, Cochrane, Scopus, ScienceDirect, Embase, and ProQuest for articles published up to November 2023; there is no limitation for older studies. Using Boolean expressions, we combined both the MeSH terms and free-word terms such as “conjunctivitis AND (viral OR bacterial) and “corticosteroid,” and their related synonyms for a comprehensive search. Details of terms being used in different search engines are elaborated in Table 1. After aggregating results from all databases, duplicates were systematically eliminated. Initial screening was based on titles and abstracts, followed by a more in-depth assessment of full-text articles to determine study eligibility. Only human clinical trials written in English were included.
Literature Searching Strategy
Study selection
For a study to be deemed suitable for our review, it had to be a clinical trial that met the following criteria: it included patients diagnosed with bacterial or viral conjunctivitis or those with a presumed diagnosis; it examined topical corticosteroid or its combination with other medications, such as antibiotics or antiseptics; and it primarily evaluated the clinical resolution or safety of the treatment. We imposed no restrictions concerning the publication year. Articles with animal models, in vitro studies, review articles, case series, case reports, and epidemiological studies were excluded.
Data processing and presentation
All articles that fulfilled the inclusion and exclusion criteria were thoroughly examined for data availability. All study selection and data extraction were conducted independently by two reviewers, and discrepancies in data extraction were resolved by discussion as needed. Data were presented in tables of study characteristics. The characteristics of the study population and treatment analyzed in this study were the infectious cause, mean age, number of subjects involved, and follow-up. The outcome variables described in this study were efficacy and safety outcomes. The quality of each study was rigorously assessed. Clinical trials were evaluated using the Jadad scale. 8
Analysis was done using Review Manager v.5.4. For the synthesis of quantitative data, we employed a random-effects model approach. The meta-analysis outcomes were visualized on a forest plot, presenting odds ratios accompanied by their 95% confidence intervals for proportional outcome data. Studies with missing data for meta-analysis were not included. Heterogeneity was assessed with the I2 statistic. Possible causes of heterogeneity among study results were explored using subgroup analysis. Whenever a comparison included a minimum of ten studies, we probed for potential publication bias using funnel plots.
Operational definition
The following are the operational definitions of the terms used in this literature review:
Viral conjunctivitis
Viral conjunctivitis is an infection of the conjunctiva confirmed by conjunctival swabs for polymerase chain reaction (PCR) detection. 9
Bacterial conjunctivitis
Bacterial conjunctivitis is conjunctival inflammation with mucopurulent discharge caused by bacteria, as confirmed by a swab sample from the inferior conjunctiva for microbiologic testing. 10
Corticosteroid
In this review, only topical corticosteroids will be considered, either used independently or in combination with other topical medications. Systemic corticosteroid was not considered to be in the scope of this review. 11
Efficacy
Efficacy assessment includes clinical resolution, duration of disease, and viral/bacterial eradication.
Clinical resolution
Clinical resolution is defined as the absence (score 0) of both bulbar conjunctival redness and conjunctival discharge. 12
Conjunctival injection
Conjunctival injection or conjunctival redness is a pathological vasodilatory response of the microvasculature in response to inflammation. 9
Conjunctival discharge
Conjunctival discharge is a common sign of acute inflammation. It can be a purulent, mucopurulent, watery discharge. 9
Duration of disease
Duration of disease is defined as the duration until signs and symptoms of conjunctivitis (conjunctival injection, discharge, scratchy sensation) are resolved. 13
Viral/bacterial eradication
Viral eradication is the reduction of viral titer confirmed by PCR or eradication of infectious virus as determined by cell culture with confirmatory immunofluorescence (CC-IFA). 14
Bacterial eradication is defined as the absence of or no detectable growth of the bacterial species confirmed by bacterial culture from a conjunctival swab sample. 13
Safety
Safety assessments include adverse events, best-corrected visual acuity (BCVA), and intraocular pressure (IOP).
Adverse event
An adverse event is defined as an ocular event that occurred or worsened after the administration of the study drug. 13
Best corrected visual acuity
BCVA is assessed using the Early Treatment Diabetic Retinopathy Study Chart logarithm of the minimum angle of resolution (logMAR) or Snellen chart. Changes in visual acuity of more than two lines are considered abnormal. 15
Intraocular pressure
IOP is measured by using tonometry. A value of >21 mmHg is considered abnormal. 16
Results
Search result
The process of conducting a literature search across six distinct search engines resulted in the identification of a total of 261 articles. Following the initial retrieval of these articles, a thorough screening process was undertaken to remove any duplicates.
During the title and abstract screening phase, as many as 147 articles were excluded for various reasons. Articles were excluded due to a lack of alignment with the clinical question or because they were not clinical trials.
A full-text search was subsequently conducted for the 13 articles that passed the title and abstract screening. One article did not have the full text, as it was a conference abstract, leaving 12 articles for the full-text assessment phase. At this stage, three articles were excluded due to misalignment of intervention characteristics with eligibility criteria. This left nine articles to be included in the systematic review. Due to an additional article found by hand searching, eventually, ten articles were considered eligible for the analysis. Seven of the included studies were included in the meta-analysis. The flow chart for study selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 17 is shown in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart for study selection.
Studies characteristic
Table 2 summarizes the characteristics of each study. The majority of the studies focused solely on subjects with viral conjunctivitis, while the study by Ta et al., 10 Hosseini et al., 13 and Rhee et al. 24 included subjects with bacterial conjunctivitis. The majority of the studies recruited adult-aged subjects, with a mean age of 30–60 years old. The follow-up duration ranged from 3 to 16 days, with most studies having a dropout rate of less than 20%. The inclusion and exclusion criteria of each included study are summarized in Table 3.
Characteristics of Included Studies
Int, Intervention; Com, Comparison; n.a, data not available.
Inclusion and Exclusion Criteria
Given that only the comparisons between dexamethasone and artificial tears and the comparison between the dexamethasone-povidone iodine combination and the vehicle were detailed in more than two studies, a more specific meta-analysis was conducted only for these two comparisons. Of three studies not included in the meta-analysis, one study is a single-arm study. 14 One study compared dexamethasone-antibiotic combination with a combination of antibiotic and loteprednol, another corticosteroid. 24 The other study, although comparing dexamethasone-povidone iodine combination with artificial tears, did not report specific outcomes on clinical remission and adverse events. 25
The quality assessment of the studies was conducted using the Jadad scale (Table 4). The study with the lowest score is Pelletier et al., 14 a single-arm study, with a score of one. The two studies that received a score of four faced challenges due to unclear descriptions regarding the randomization process. Two studies that scored three additionally did not specify how the blinding process was conducted, resulting in a suboptimal score for the double-blinding criterion.
Quality Assessment of Included Studies by Jadad Scale
Efficacy outcomes
Clinical resolution
The conceptualization of “clinical resolution” exhibits variability across different studies. The study by Ward et al. 22 lacks a precise delineation of the criteria for a subject to be classified as having achieved clinical resolution. The data on clinical resolution in the study by Wilkins et al. 21 was derived from the proportion of subjects self-reporting their discomfort level as “none (0)” during follow-up assessments. Hosseini et al. 13 characterized the clinical resolution as a score of zero on the Subject’s Global Efficacy Rating, indicating complete remission of signs or symptoms. In the research conducted by Pinto et al., 18 a clinical resolution was quantified based on the number of subjects exhibiting an absence of overall symptoms, including itching, foreign body sensation, tearing, redness, and eyelid swelling. Pepose et al., 19 in their 2018 study, defined clinical resolution through the absence of both bulbar conjunctival redness and watery conjunctival discharge, a definition which was similarly employed in the subsequent 2019 study by Pepose et al. 12 as well as by Ta et al. 10
A meta-analysis integrating data from all pertinent studies (depicted in Fig. 2a; sample size = 1398) discerned that those various topical treatments containing dexamethasone markedly increased the incidence of clinical resolutions compared to non-dexamethasone topical treatments, yielding a combined odds ratio of 1.51 (95% confidence interval [CI]: 1.19–1.92). The heterogeneity analysis showed substantial homogeneity among the included studies (I2 = 0%). Analogous trends were noted in the comparative analysis between the dexamethasone-povidone iodine combination and a placebo, with the results deemed uniformly consistent (Fig. 2b; sample size = 659; odds ratio [OR]: 1.47; 95% CI: 1.07–2.00; I2 = 0%).
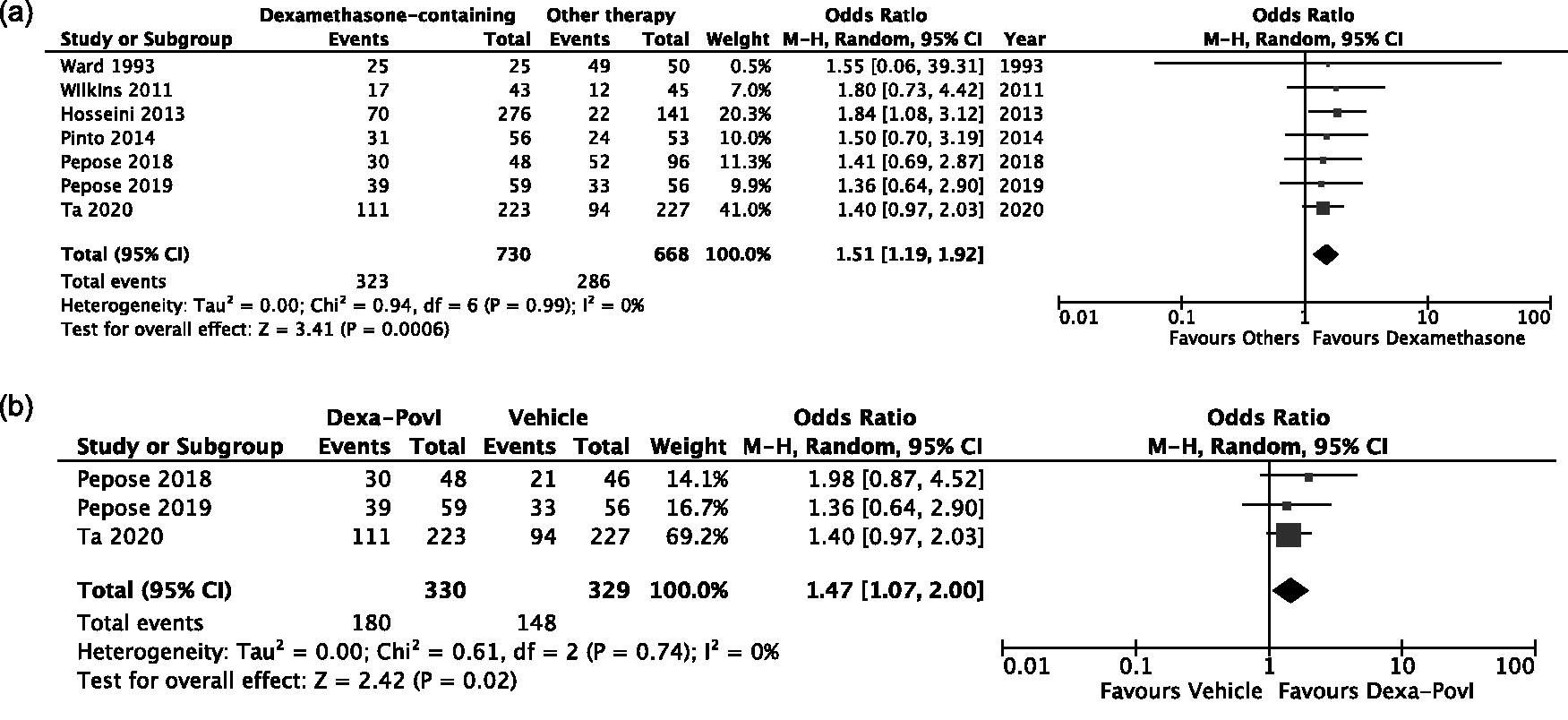
Forrest plot of meta-analysis results on clinical resolution in patients with infectious conjunctivitis on
Clinical symptom and sign grading
Several studies have utilized different approaches to report clinical symptoms and sign grading as influenced by intervention. Rhee et al. 24 developed a posttreatment symptom score encompassing blepharitis, conjunctivitis, discharge, and keratitis, with each symptom graded on a scale from 0 (absent) to 3 (severe). The mean total ocular score was calculated by summing these four symptom scores. Similarly, Pelletier et al. 14 focused on conjunctival injection and discharge, using the same grading scale and performing daily assessments until scores returned to zero. Kovalyuk et al. 25 expanded the range of evaluated symptoms and signs, including eye itching, foreign body sensation, and conjunctival injection, among others, also graded from 0 to 3, with assessments repeated over several days posttreatment. Wilkins et al. 21 reported patient discomfort and conjunctival hyperemia using a slightly varied scale, including a unique assessment method—the Efron grading scale. Lastly, studies by Pepose et al. in both 2018 23 and 2019 12 introduced a global clinical score, combining bulbar conjunctival redness and watery discharge scores, with a potential range of zero to six.
In their research, Rhee et al. 24 observed that the combination of tobramycin 0.3% with dexamethasone 0.1% demonstrated numerically superior reductions in all ocular symptom scores when compared to the combination with loteprednol 0.5%. The superiority of the tobramycin 0.3%/dexamethasone 0.1% treatment in controlling posttreatment signs of blepharitis, conjunctivitis, and ocular discharge was statistically significant, with respective p values of 0.017, 0.013, and 0.025. However, while mean keratitis scores were lower with tobramycin 0.3%/dexamethasone 0.1%, the difference was not statistically significant (P = 0.065). The treatment also resulted in significantly superior mean total ocular scores at post-visit evaluations (P < 0.05). 24
Pelletier et al. 14 reported significant decreases in symptom and sign gradings in all subjects completing follow-up, with resolution typically by day 3–5. This pattern was echoed in the Kovalyuk et al. 25 studies, where the study group showed notable reductions in symptoms, dropping from median scores of 2.0 or 3.0 at baseline to 0.0 within 5–7 days. In contrast, control groups experienced minimal reductions or no significant changes (P < 0.001). Additionally, no significant episcleral injections (SEIs) were observed in the study group during the 7-day follow-up, while their occurrence in control groups was notable, increasing significantly by day 7 (P < 0.001).
Wilkins et al. 21 reported varying levels of discomfort and hyperemia in patients using Hypromellose compared with those in the dexamethasone group. The patient-reported levels of discomfort and observer-graded conjunctival hyperemia were similar between the treatment groups, as indicated by p values of 0.204 and 0.310, respectively.
Finally, Pepose et al. (2018) 19 found the efficacy of povidone-iodine (PVP-I)/dexamethasone treatment significantly greater than the vehicle treatment at various observed time points. The PVP-I/dexamethasone group saw a more substantial reduction from the baseline in the global clinical score and a higher proportion of patients experiencing improvement from baseline at all visits. However, a subsequent study by Pepose et al. in 2019 12 did not report a similar significant difference in the reduction of the global score on day 6 in subjects receiving different interventions.
Duration of symptoms
Both studies by Ward et al. 22 and Pinto et al. 18 reported the duration of symptoms in each group of intervention. In addition, Ward et al. 22 reported the duration of isolation imposed on the subjects. In the study by Ward et al., 22 the artificial tears group, on average, experienced 11 days of symptoms or signs and 10 days of isolation in living quarters. The group treated with trifluridine had 11 days of symptoms or signs and 9 days of quarantine. Meanwhile, the steroid-treated group had an average of 10 days of symptoms or signs and 8 days of quarantine. There was no observed difference in the duration of symptoms (P = 0.56) and the isolation to quarters (P = 0.43) among all intervention groups. In contrast, Pinto et al. 18 revealed that the duration of symptoms differed significantly between groups. The intervention group had a mean of 9.4 ± 4.6 days, whereas the comparison group recorded 11.8 ± 4.9 days (P = 0.009).
Viral/bacterial eradication
In the realm of viral/bacterial eradication research, there exists a spectrum of outcomes as documented in various scholarly studies. For instance, in the context of bacterial eradication, Hosseini et al. 13 delineated this phenomenon as either the complete absence or the non-detectability of the bacterial species by the fifth patient visit, concurrently evaluating the extent of bacterial colonization reduction by the same juncture. Similarly, Ta et al. 10 characterized bacterial eradication as the non-presence of all bacterial species that were initially identified at or above pathological thresholds at baseline, specifically at the day 5 visit.
In the domain of viral eradication studies, Pelletier et al. 14 presented an analysis of daily viral titers using quantitative polymerase chain reaction (qPCR) and assessed viral infectivity through CC-IFA. Complementing this, Kovalyuk et al. 25 detailed their findings through repeated measurements of viral titers via real-time PCR. In the 2018 publication, Pepose et al. 19 defined adenoviral eradication as a negative CC-IFA result in the studied eye. A subsequent study by the same group in 2019 expanded on this by reporting viral status utilizing methods such as qPCR or CC-IFA.
Hosseini et al. 13 found that there was a significant difference in bacterial eradication when comparing the dexamethasone-azithromycin combination with sole dexamethasone (P = 0.007). They also reported that the reduction of bacterial load in relation to colonization is greater in the group receiving dexamethasone–azithromycin combination in comparison with sole dexamethasone (P = 0.024). Nevertheless, when the dexamethasone-azithromycin combination was compared with sole azithromycin only, the difference was not statistically significant (P = 0.305). 13 In contrast, Ta et al. 10 reported that there was no significant difference in bacterial eradication by day 5 when comparing the combination of dexamethasone and povidone–iodine with the vehicle. The eradication rates were 43.3% and 46.8%, respectively (P = 0.500).
Kovalyuk et al. 25 found that all patients have detectable virus reduction and reported that dexamethasone and povidone–iodine resulted in a faster reduction in adenovirus titer compared to control groups. In addition, Pelletier et al. 14 also reported that all patients except one have diminished infectivity. Pepose et al. 19 in the 2018 study also discovered that the combination of dexamethasone and povidone–iodine treatment resulted in a 79.2% eradication rate of adenoviral infections by day 6, which was notably higher than the 56.5% observed with the vehicle (P = 0.019) and 62.0% with povidone–iodine (insignificant p value). However, in the other study by Pepose et al. in 2019, 12 there is no difference in adenovirus detection between patients in the PVP-I/dexamethasone and vehicle groups.
Safety outcomes
Ocular adverse events
In this review, we are focusing on the outcome of adverse events to include only ocular adverse events. The usual adverse events usually being reported were pseudomembrane, subepithelial infiltrate, pain at the instillation site, blurry vision, and other post-treatment complaints.13,18,21 Three studies13,18,21 mentioned similar kinds of ocular adverse events, as well as other adverse events, that happened after the first installation of study medication as treatment-emergent adverse events (TEAE).
Regarding ocular adverse events as an outcome, the meta-analysis of all included studies found no difference in outcomes from various topical interventions containing dexamethasone compared to non-dexamethasone topical interventions (Fig. 3a; n = 1567; OR 1.33; 95% CI 0.82–2.16). However, heterogeneity tests showed significant heterogeneity between the studies (Tau2= 0.24; Chi2 = 16.27, df = 5 [P = 0.006]: I2= 69%). We tried to explore heterogeneity by analyzing only studies with the same intervention and control, in this case, studies comparing dexamethasone 0.1% + povidone iIodine 0.6% q.i.d. and control vehicle. However, similar findings were observed (Fig. 3b; n = 892; OR 1.26; 95% CI 0.57–2.77) and heterogeneity persists (Tau2 = 0.38; Chi2= 10.11, df = 2 [P = 0.006]; I2= 80%).

Forrest plot of meta-analysis results on ocular side effects in patients with infectious conjunctivitis on
A comparison of dexamethasone with artificial tears was not feasible, as the study by Ward et al. 22 did not report the number of patients with ocular side effects. However, Ward et al. 22 did not report any side effects that led to the discontinuation of participation. Similarly, Wilkins et al., 21 Rhee et al., 24 and Pelletier et al. 14 did not identify any serious complications. However, Wilkins et al. 21 did report ocular adverse events, including conjunctival pseudomembrane and subepithelial corneal infiltrates. Hosseini et al. 13 reported that 25% of patients experienced AEs, but these were evenly distributed across the intervention groups. Pinto et al. 18 reported no significant difference in the frequency of subepithelial corneal infiltrate during follow-up. However, there was a significant difference in terms of stinging as an adverse event (P < 0.05).
Pepose et al. 19 in the 2018 study highlighted that the vehicle group experienced the highest TEAEs, followed by the povidone–iodine and the combination of dexamethasone and povidone–iodine groups. Most of these TEAEs were mild and ocular. Notably, none were suspected to be directly related to the treatment. The 2019 study by Pepose et al. 12 found no serious AEs or deaths, with the most frequently reported TEAEs being mild instillation site pain and corneal infiltrates.
Ta et al. 10 presented results consistent with Pepose et al., where no serious AEs or deaths were reported. The most common ocular TEAE was instillation site pain, which was primarily mild to moderate in severity. Additionally, low incidences of punctate keratitis and corneal infiltrates were noted. A unique non-ocular TEAE related to the combination of dexamethasone and povidone–iodine reported in this study was dysgeusia, affecting 1.5% of the subjects.
Visual acuity
In their study, Wilkins et al. 21 assessed unaided visual acuity utilizing the Snellen chart. They observed that the median posttreatment unaided visual acuity in both experimental groups was equivalent, specifically at 6/6. Hosseini et al. 13 examined visual acuity as a component of safety outcomes, defining no change in visual acuity as a deterioration of fewer than three lines during the fifth visit compared to baseline measurements. Their findings indicated that visual acuity remained predominantly stable in the majority of participants across different intervention groups, with stability rates of 91.4% in the dexamethasone-azithromycin group, 87.9% in the azithromycin-only group, and 89.0% in the dexamethasone-only group. Similarly, Rhee et al. 24 reported no significant clinical changes in visual acuity, as measured by the Snellen chart, in either treatment group throughout their study.
Pepose et al., 19 in a 2018 publication, did not specifically address visual acuity in the context of safety outcomes. However, their subsequent 2019 study 12 employed best spectacle-corrected visual acuity (BSCVA), assessed using the Early Treatment Diabetic Retinopathy Study (ETDRS) chart, as a measure of visual acuity changes. This study reported that the mean changes in BSCVA during the study period did not reveal significant improvements in any treatment group. Nevertheless, some participants did experience changes in BSCVA of 0.22 logMAR or greater (3.6% [2/55] in the PVP-I/dexamethasone group and 3.7% [2/54] in the vehicle group on Day 6; 5.0% [1/20] in the PVP-I/dexamethasone group and 10.0% [2/20] in the vehicle group at Day 11–14). Overall, the collective findings from these studies suggest that the treatments did not result in notable changes in visual acuity.
Intraocular pressure
Across various studies, the change in IOP among subjects undergoing corticosteroid-containing therapies was consistently reported as insignificant. Ward et al. 22 noted that none of the subjects exhibited a posttreatment IOP exceeding 22 mmHg or an increase in IOP of 6 mmHg or more. Wilkins et al. 21 observed that the mean post-treatment IOP in the right eye was 14.05 mmHg (SD 3.70) in the Hypromellose group and 13.5 mmHg (SD 3.07) in the dexamethasone group, with similar values for the left eye.
Hosseini et al. 13 found that, across all follow-up visits, the mean IOP change was marginally higher in the dexamethasone-azithromycin and dexamethasone-only groups compared to the azithromycin-only group. The median IOP change was zero in the azithromycin-only group and 1.0 mmHg in the other two groups. However, these differences were not statistically significant. Similarly, Pinto et al. 18 reported no significant differences in IOP across various visits and interventions in the dexamethasone 0.1%/povidone–iodine 0.4% group compared to the artificial tear group. Rhee et al. 24 also reported consistent mean IOP values pre- and posttreatment in both study groups.
Discussion
Pathophysiology of infective conjunctivitis
Conjunctival infection by pathogenic microorganisms can happen mostly by exogenous inoculation. These pathogens usually have properties that enable them to adhere to, invade, or break the ocular epithelium barrier. In addition, they also have properties to protect themselves from immune response. 9
Penetration of pathogens through conjunctival epithelium will immediately trigger the dilation of conjunctival vasculature and induce the increase of vascular permeability. It will manifest into chemosis, swelling, and hyperemia of the conjunctiva. 20 In some cases of infection or conjunctival foreign bodies, the aforementioned process can also cause inflammatory exudate that is composed mostly of fibrin and slowly develops into a yellow–white thin pseudomembrane. 23
Neutrophil and Th1 cells will be the main contributors to the immune response toward the pathogen, releasing interleukin-1 (IL-1) and interferon-γ, while the epithelial cells of conjunctiva support the inflammatory response against infection by releasing IL-6, IL-8, and tumor necrosis factor-α. These cytokines can also enter the tear fluid and corneal stroma in the event of corneal epithelium damage, activating corneal fibroblasts. 20 This kind of inflammatory action in the cornea in response to infection in conjunctiva can manifest into subepithelial infiltrate, which is transformed keratocytes and Langerhans cells of the cornea responding to the inflammatory signaling and action from conjunctiva. 26
Corticosteroids: Mechanism of action
Corticosteroids are synthetic analogs of steroid hormones produced by the adrenal cortex, primarily glucocorticoids, which play a significant role in metabolism as well as in the regulation of the immune system and inflammatory responses. 11 Recognized for their therapeutic efficacy in ocular inflammation, corticosteroids have played a pivotal role in clinical practice for over half a century. The anti-inflammatory action of corticosteroids is multifaceted, encompassing the interruption of the inflammatory cascade at several junctures. This includes the inhibition of eicosanoid biosynthesis, the modulation of cytokine, chemokine, and matrix metalloproteinase activity, as well as reducing the stability of mRNA of various inflammatory mediators like vascular endothelial growth factor and cyclooxygenase 2.27,28 The therapeutic actions of corticosteroids are mediated through both genomic and non-genomic pathways.29,30
Corticosteroid and conjunctivitis
Some published clinical guidelines include corticosteroids as one of the treatment options for infective conjunctivitis, especially viral conjunctivitis with pseudomembrane formation. 3 However, some guidelines and literature on conjunctivitis specifically cautioned about the potential prolonged adenoviral infection or worsening HSV infection caused by corticosteroid administration.3,6,31
AAO guidelines suggest that topical corticosteroids can alleviate symptoms and potentially mitigate scarring in severe manifestations of adenoviral keratoconjunctivitis, characterized by pronounced chemosis, eyelid edema, epithelial loss, or membranous formations. However, stringent monitoring is essential for those receiving corticosteroids for adenoviral conjunctivitis, given that animal studies indicate an extension in viral shedding posttreatment, although the relevance to human cases remains unclear. Additionally, therapeutic use of povidone–iodine at 0.4%, alone or augmented with dexamethasone at 0.1%, has been associated with decreased viral loads, limited viral propagation, a shortened duration of clinical symptoms, and the conservation of visual acuity. Meanwhile, AAO does not include corticosteroids as therapeutic options for bacterial conjunctivitis. 31
All included clinical trials provided evidence of the efficacy and safety of corticosteroids for conjunctivitis. It helps reduce the duration and the severity of signs and symptoms to the point of resolution. This kind of effect can be based on the immunomodulatory role of steroids as provided in multiple preclinical studies. Notably, research by Shoji et al. 32 elucidated that dexamethasone administration in rat models led to a diminished density of immune system cells in subconjunctival tissues. Their work also unveiled corticosteroids’ genomic control over inflammation, spotlighting dexamethasone’s inhibition of the C ε gene expression. Complementary findings from studies on bacterial conjunctivitis animal models indicate that a dexamethasone-antibiotic combination curtails infection rates and reduces cytokines, including IL-6 and transforming growth factor beta (TGF-ß). 33 This immunomodulatory role reduces the inflammatory process that happens in conjunctivitis, resulting in the resolution of signs and symptoms.
Regarding the efficacy of corticosteroids in pathogen eradication, current evidence presents a contentious landscape. A comprehensive analysis of pertinent studies indicates that the optimal eradication efficacy of corticosteroid-containing therapy is predominantly evident in combination regimens, such as those pairing corticosteroids with antibiotics or povidone–iodine. However, as highlighted in research by Hosseini et al. 13 and Pepose et al., 12 the efficacy of topical antibiotics or povidone–iodine alone in pathogen eradication should not be underestimated. This observation necessitates a cautious approach toward prescribing corticosteroids for infective conjunctivitis, particularly in light of preclinical evidence suggesting that corticosteroids may prolong viral shedding in animal models of conjunctivitis, as noted by Romanowski et al. 6
In this systematic review, half of the ten included studies, including three within the meta-analysis, investigated the efficacy of a corticosteroid and povidone–iodine combination in treating bacterial or viral conjunctivitis. This therapeutic approach has been deemed at least as effective, if not superior, to other treatment modalities. While corticosteroids address the inflammatory symptoms of conjunctivitis, povidone–iodine exhibits pathogen-killing properties against both bacteria and viruses. The mechanism involves the release of free iodine from the aqueous solution of povidone–iodine, which penetrates bacteria and interacts with proteins, nucleotides, and fatty acids, thereby exerting a bactericidal effect. Additionally, iodine impedes essential viral enzymes, obstructing viral attachment to host cell receptors and hindering viral replication, as described by Dang et al. 34 Notably, a preclinical study on adenoviral conjunctivitis by Clement et al. 35 demonstrated that a combination of dexamethasone with povidone–iodine resulted in lower viral titers, comparable to those achieved with antiviral agents alone. Consequently, if corticosteroids are to be utilized for infective conjunctivitis, a combination regimen with an antibiotic such as azithromycin, or with povidone–iodine in cases of viral conjunctivitis, is preferable.
The review also assessed the adverse events associated with corticosteroid-containing therapy for conjunctivitis, finding them to be infrequent and non-severe. Pain at the instillation site was among the most commonly reported adverse events, particularly prevalent in combination regimens involving corticosteroids with antibiotics or povidone–iodine, as noted in studies by Hosseini et al., 13 Pinto et al., 18 and Pepose et al.12,19 This increased incidence of instillation pain might be attributed to the antibiotic or povidone–iodine components, given the known cytotoxic effects of povidone–iodine on corneal cells as documented by Chou et al. 36
Limitations
Despite efforts to conduct a comprehensive search, resource and language constraints may have limited the inclusivity of the search, potentially biasing the findings toward studies published in English and indexed databases. Ambiguities in the methodological design of some studies, especially regarding randomization, and differences in therapeutic combinations and follow-up durations, may have introduced elements of variability and heterogeneity. he variability is notably evident with regard to viral/bacterial eradication. There are different operational definitions being used in several studies, hindering the ability to statistically synthesize the effect size for this outcome. Moreover, no study reported time to viral/bacterial clearance, highlighting a research gap that should be filled by future studies.
Implications for practice and future research
Future research is needed on the role of corticosteroids in infective conjunctivitis, especially bacterial conjunctivitis, and determining the most effective pharmacologic combinations. These studies will be pivotal in refining an evidence-based approach to treating infectious conjunctivitis.
Conclusion
This systematic review and meta-analysis highlight the efficacy of corticosteroids, specifically topical dexamethasone in combination with antibiotics or antiseptics, for the treatment of infective conjunctivitis. Corticosteroid therapy results in a significantly higher rate of clinical resolution and reduces the duration and severity of symptoms and signs of conjunctivitis. Corticosteroid therapy is also relatively safe with few potential adverse events. More research on corticosteroid use in infective conjunctivitis is needed, especially on bacterial conjunctivitis and on identifying the effective pharmacological combinations.
Footnotes
Authors’ Contributions
L.R.P.: Data curation; formal analysis; methodology; visualization; writing—original draft. L.E.: Supervision; validation; writing—review and editing.
Author Disclosure Statement
The authors of this systematic review article report no conflict of interest.
Funding Information
This systematic review article received no government or nongovernment funding/support.