
Abstract
Background/Aims:
To investigate the effectiveness of re-esterified triglyceride form of omega 3 (rTG-omega 3) on patients with meibomian gland dysfunction (MGD) after cataract surgery.
Methods:
This multicenter, randomized, investigator-blinded, clinical study was conducted between June 2021 and March 2023 and enrolled 107 patients with MGD who had undergone cataract surgery within 3 months at seven sites across South Korea. Patients were randomly assigned to rTG-omega 3 group or a control group. We compared (1) tear film break-up time (TBUT) (s), (2) corneal fluorescein staining score [National Eye Institute/Industry (NEI) scale], (3) conjunctival fluorescein staining score (NEI scale), (4) strip meniscometry (SM) tube score (mm), (5) MGD stage, (6) MG quality, (7) MG expressibility, (8) Standard Patient Evaluation of Eye Dryness (SPEED) score, and (9) Ocular Surface Disease Index (OSDI) scores at baseline and 6 and 12 weeks.
Results:
TBUT, corneal fluorescein staining score, and SM tube score were significantly improved in the rTG-omega 3 group compared with control group (P = 0.005, P = 0.003, and P = 0.0049, respectively). Subjective questionnaire responses were also improved significantly (SPEED score, P = 0.022; OSDI score, P = 0.0011). MGD parameters were not significantly different. However, during subanalysis, significant improvements in MG quality and expressibility were observed in the MGD stage 4 group with rTG-omega 3 supplementation (P = 0.0177 and P = 0.0205, respectively).
Discussion:
rTG-omega 3 supplementation facilitated improvements in both objective and subjective parameters. In particular, MG quality and expressibility were significantly improved in the severe MGD group.
Introduction
Dry eye disease (DED) is very common worldwide, affecting about 5%–30% of individuals ≥50 years of age. 1 Multiple factors can cause DED, but one of the most frequent causes is meibomian gland (MG) dysfunction (MGD),1–3 which causes tear film lipid layer instability. 3
Previous studies have reported that cataract surgery can aggravate MGD. Qiu et al. found that lid margin morphology and meibum expression significantly worsened after cataract surgery. 4 It results in reduced visual acuity or continuous discomfort of the ocular surface, adversely affecting patient satisfaction and quality of life.5,6 Therefore, controlling MGD after cataract surgery is important for good surgical outcomes. Many treatments, including artificial lubricants, eye ointments, anti-inflammatory agents, warm compression, and antibiotics, are used to improve MG lipid flow and tear film stability. 7 However, the treatment outcome is often inadequate, suggesting the necessity of other treatments that can target the fundamental mechanism. 8
Recently, some investigators suggested omega 3 oral supplementation for MGD treatment.9–11 The Tear Film and Ocular Surface Society Dry Eye Workshop proposed omega 3 oral supplementation for DED modification.3,12 A cohort study reported that supplementation with a re-esterified triglyceride (TG) form of omega 3 (rTG-omega 3) improved subjective questionnaire responses. 13 These studies explained that omega 3 supplementation exerts its function through the following mechanisms. Inflammation plays a significant role in chronic MGD. 14 Metabolizing omega 3 produces anti-inflammatory molecules that inhibit arachidonic acid (AA) pathways competitively. 15 Eicosapentaenoic acid (EPA) and alpha-linolenic acid adjust the prostaglandin pathway toward anti-inflammatory eicosanoid synthesis, which suppresses inflammation.15,16 Oral omega 3 intake may also affect the lipid composition of meibum, leading to tear film stability.13,17
On the other hand, other studies argue that omega 3 does not play a critical role in reducing MGD symptoms. Asbell et al. reported that dietary intake of oral omega 3 over 12 months did not improve DED compared with placebo. 18 Likewise, another randomized clinical trial found that omega 3 fatty acids had no significant effect on meibum lipid composition or tear film evaporation rate. 19
Considering these conflicting arguments, Park et al. suggested that the type of omega 3 be considered. 13 The previous studies were all performed with the ethyl ester (EE) form of omega 3, which might influence the outcome. Omega 3 can exist in various forms, including a TG form, EE form, phospholipid form, and free fatty acid form. 15 Among the forms, variations in bioavailability exist within the body. 20 By re-esterification, the chemically adjusted EE form of omega 3 can be changed to the TG form, which exhibits the greatest bioavailability and has fewer digestive side effects. 21
Therefore, in this study, we aimed to investigate the effectiveness of rTG-omega 3 oral supplementation. As far as we know, only a pair of studies to date has demonstrated the effectiveness of omega 3 supplementation in DED aggravated by cataract surgery.13,22 Both studies reported improvements in subjective symptoms, but they yielded contrasting results concerning effects on objective signs like the tear film break-up time (TBUT) and Schirmer test results. We believe that these results are due to the previous studies being conducted on a variety of patients with DED without delineation by type. Improving MG quality might play a more critical role in MGD-type DED than in the aqueous-deficient type DED. Accordingly, the present study analyzed the effectiveness of rTG-omega 3 oral supplementation in DED associated with MGD, which has not been investigated before. Additionally, we divided patients according to MGD stage and compared improvements in MGD parameters between these groups. As far as we know, no prior study has divided patients based on MGD severity. We believe this analysis will help with establishing criteria for oral supplementation of rTG-omega 3.
Materials and Methods
This was a multicenter, prospective, randomized investigator-blinded study conducted between June 2021 and March 2023. We enrolled 140 patients across seven sites in South Korea. This study was conducted after obtaining approval from the institutional review boards of these seven sites and adhered to the Declaration of Helsinki. Prior to study enrollment, all candidates signed an informed consent form.
The trial is registered at the Ministry of Food and Drug Safety of South Korea, number of TJO-2101-501. We used CONSORT 2010 guidelines when writing this study. 23
Patient selection
Patients with DED with MGD who had undergone cataract surgery within 3 months in one of seven centers in South Korea were invited to participate. Consistent with previous studies,24–26 we diagnosed patients with MGD if they satisfied one or more of the following criteria. (1) waxy white or viscous secretion upon digital expression, 27 (2) the presence of margin telangiectasias at more than two sites, and (3) plugging of more than two gland orifices.24–26 We also measured the fluorescein TBUT of participants and only included those whose TBUT was <10 s. 28
Patients were excluded from the current study if they had any preexisting ocular or eyelid disease. Also, those who had undergone ocular surgery other than cataract surgery were not included. Patients with systemic diseases like Sjögren’s syndrome, those with malignant tumors, or individuals taking systemic medications that might affect the ocular surface were not eligible to participate. Contact lens wearers, pregnant women, and patients with allergic disorders were also excluded. 11 The details of the exclusion criteria are described in Table 1.
Exclusion Criteria
Eye disorder [abnormal eyelid function (when all meibomian gland outlets are blocked or when there is something wrong with the eyelashes, etc.), herpetic keratopathy, conjunctival scarring due to cicatricial keratoconjunctivitis (alkaline damage, Steven-Johnson syndrome, ocular scarring, bullous pemphigoid), pterygium, congenital lacrimal gland deficiency, neurotrophic keratopathy, keratoconus, corneal transplantation, etc.)].
Patients were asked to restrict the use of ocular lubricants other than artificial tears (New Hyaluni ophthalmical solution 0.15%; Taejoon, Seoul, South Korea) and to avoid performing warm eyelid compression, which can improve DED syndrome.
The patients with MGD who underwent cataract surgery within 3 months were randomly assigned using a computer-generated random number table into two groups. Group 1 (the rTG-omega 3 group) received dietary omega 3 supplementation [Ocuaredstwo; Taejoon for a total of 1,000 mg of EPA + DHA (EPA:DHA = 571.4:428.6)], 2 tablets twice daily for 12 weeks with artificial tear eyedrops (New Hyaluni 0.15%; Taejoon).Group 2 (control group) was only allowed to use artificial tear eyedrops to control DED without rTG-omega 3 supplementation. Eyedrop instillation was allowed up to six times a day in both groups.
Participants were instructed not to use artificial tears on the day when evaluation visits to the clinic were scheduled.
In this study, patients documented their medication adherence daily. Additionally, patients were instructed to bring any remaining doses of omega 3 supplements during both at the 6-week visit and at the 12-week visit. A comparison was made between the patient records and the remaining quantity of omega 3 supplements. In instances where the two values differed, adherence was determined based on the quantity of remained medication. Then, the compliance rate is calculated as follows: (number of consumed capsules/total number of capsules to be taken per day) × 100.
Sample size calculation
The primary endpoint of this study is to prove that the improvement in TBUT of the rTG-omega 3group after 12 weeks is superior to that of the control group. α was 0.05 and β was 0.2 which means confidence interval was 95% and power was 80%.
The ratio of the number of subjects in the test group and control group is 1. We used the results of an article by Epitropoulos et al., a clinical trial using the improvement in TBUT, which is the same evaluation variable as this study. Therefore, the resulting pooled standard deviation was 3.62, and mean change difference between the two groups was applied as 2.00.
Zα/2 was the critical value or quantile at which the right tail area becomes α/2, and Zβ was the critical value or quantile at which the right tail area becomes β in a standard normal distribution.
Using the above formula, the minimum number of subjects is 52.
Appropriate efficacy assessment requires approximately 70 subjects to be registered per group, considering a dropout rate of approximately 25%, resulting in a total of 140 subjects across both groups.
Masking
To maintain blinding of the investigators, the allocation information regarding blinding for each group was managed in a sealed state (SNOSE) by the principal investigator. It was not disclosed until the end of the study, except in cases where it was necessary to check the assigned group due to serious adverse events or other significant clinical situations. No instances occurred where the investigator’s blinding was compromised in this study. The pharmacist, delegated by the principal investigator, provided the corresponding supplementation to the study subjects according to their assigned groups.
Measurements
Both groups visited the centers a total of three times for this study. During the first visit, which was scheduled within 3 months of cataract surgery, baseline ocular parameters were measured in patients. Subsequent follow-up measurements were conducted at 6 and 12 weeks. At each visit, ophthalmological examinations and questionnaire surveys were performed. Ocular parameters including (1) TBUT (s), (2) the corneal fluorescein staining score according to the National Eye Institute/Industry (NEI) scale, (3) the conjunctival fluorescein staining score according to the NEI scale, (4) the strip meniscometry (SM) tube score (mm), (5) MGD stage, (6) MG quality, (7) MG expressibility, (8) the Standard Patient Evaluation of Eye Dryness (SPEED) score, and (9) Ocular Surface Disease Index (OSDI) scores were measured.
We measured ocular parameters in the following sequence: The measurements of the SM tube, TBUT, cornea staining score, and conjunctiva staining score were performed. After that, MG parameters, Meibum quality, and expressibility were investigated.
At each center, an ophthalmologist was designated to conduct three ocular measurements. Patients were instructed to visit the clinic at the same time each day. The room conditions were kept consistent, with temperatures maintained between 20°C and 25°C and humidity ranging from 60% to 80% as closely as possible. The TBUT was evaluated with a stopwatch for accuracy; after fluorescein installation, the subjects were asked to blink several times. Investigators measured the time between the last complete blink and the appearance of the first corneal black spot, and the average of three trials was calculated. The corneal fluorescein staining and conjunctival fluorescein staining scores were evaluated using the NEI scale, with scores ranging from 0 to 15 and 0 to 18 points, respectively. To calculate the SM tube score (Echo Electricity Co., Ltd., Fukushima, Japan), the tip was immersed into the lower tear meniscus on the lateral side of the eyelid for 5 s. According to the criteria suggested in the International Workshop on Meibomian Gland Dysfunction, MGD was divided into five stages (1–4 and plus) based on severity. The “plus” stage was defined by comorbid conditions occurring at any stage and requiring treatment, 3 and all MGD eyes with mucosal keratinization, phlyctenular keratitis, trichiasis, chalazion, anterior blepharitis, or demodex-related anterior blepharitis were categorized into the plus stage. 3 We excluded patients who presented in the plus stage. Also, if a subject was newly categorized into the plus stage at the 6- or 12-week visit, we excluded them from the study considering the possibility of an allergic reaction to the rTG-omega 3 supplement or tear eyedrops. Assessment of meibum quality was performed at each of the eight glands in the central third of the lower lid, applying a scale ranging from 0 to 3 points for each gland [0, clear; 1, cloudy; 2, cloudy with debris (granular); and 3, thick, like toothpaste (total score range, 0–24 points)]. 3 Expressibility was the number of expressible MGs among the eight in the central third of the lower lid (total score range, 0–8 points). 3 After detailed ocular examination, subjects were asked to complete the SPEED questionnaire (total score range, 0–28 points) and OSDI questionnaire (total score range, 0–100 points).
The primary outcome was the change in TBUT from baseline to 12 weeks within the two groups. Secondary outcomes include changes at 6 weeks and 12 weeks in other ocular parameters, such as corneal fluorescein staining score, conjunctival fluorescein staining score, SM tube score (mm), MGD stage, MG quality, MG expressibility, SPEED score, and OSDI scores in both groups. Additionally, the TBUT change from baseline to 6 weeks was considered a secondary outcome. Changes in MGD parameters within each MGD stage group were also addressed as secondary outcomes.
Statistical analysis
All categorical variables were summarized by treatment group with the percentage of subjects in each category. Continuous variables are summarized descriptively with mean and standard deviation values. Sex distribution was compared with the chi-square test. In comparing between groups, normality was assessed using the Shapiro–Wilk test. When both the rTG-omega 3 group and the control group met the normality assumption, a two-sample t-test was used for comparative analysis. In cases where normality was not met in at least one group, the Wilcoxon rank-sum test was used for comparative analysis.
In baseline characteristics, both patient’s age and all ocular parameters demonstrated significance in the Shapiro–Wilk test (Table 1). Furthermore, at 6 and 12 weeks, all ocular parameters also exhibited significance in the Shapiro–Wilk test, leading to the subsequent utilization of the Wilcoxon rank-sum test (Table 2). In the analysis of MG parameters, only MG quality and MG expressibility in the MGD stage 4 group met normality, as evidenced by nonsignificance in the Shapiro–Wilk test. Consequently, a two-sample t-test was employed (Table 4).
Baseline Patient Characteristics
Chi-square test.
Wilcoxon rank-sum test.
MG, meibomian gland; MGD, meibomian gland disease; NEI, National Eye Institute/Industry; OSDI, Ocular Surface Disease Index; rTG-omega 3, re-esterified triglyceride form of omega 3; SM, strip meniscometry; SPEED, Standard Patient Evaluation of Eye Dryness; TBUT, tear film break-up time.
For within-group comparisons, a paired t-test was used. Generalized linear modeling with adjusted baseline values was used to compare changes between groups. Two-sided P values of <0.05 were considered statistically significant. Meanwhile, when the P value fell between 0.05–0.1, it was described as borderline significant. All statistical analyses were conducted using SAS® (version 9.4; SAS Institute, Cary, NC, USA).
Results
Among 140 patients found to be eligible for the study, 107 completed the study.
Fifty-six patients were included in the rTG-omega 3 supplement group, while 51 patients who only used artificial tear eyedrops without taking rTG-omega 3 supplements were included in the control group. Thirty-three participants who withdrew their consent for participation or took unapproved drugs, such as oral nonsteroidal anti-inflammatory medications, or who missed the test visits at 6 or 12 weeks, were excluded. No patient was excluded due to being newly diagnosed with the plus stage of MGD at 6 or 12 weeks (Fig. 1). The oral supplementation medication adherence of the r-TG omega 3 patients’ group was found to be 97.7% in the study.
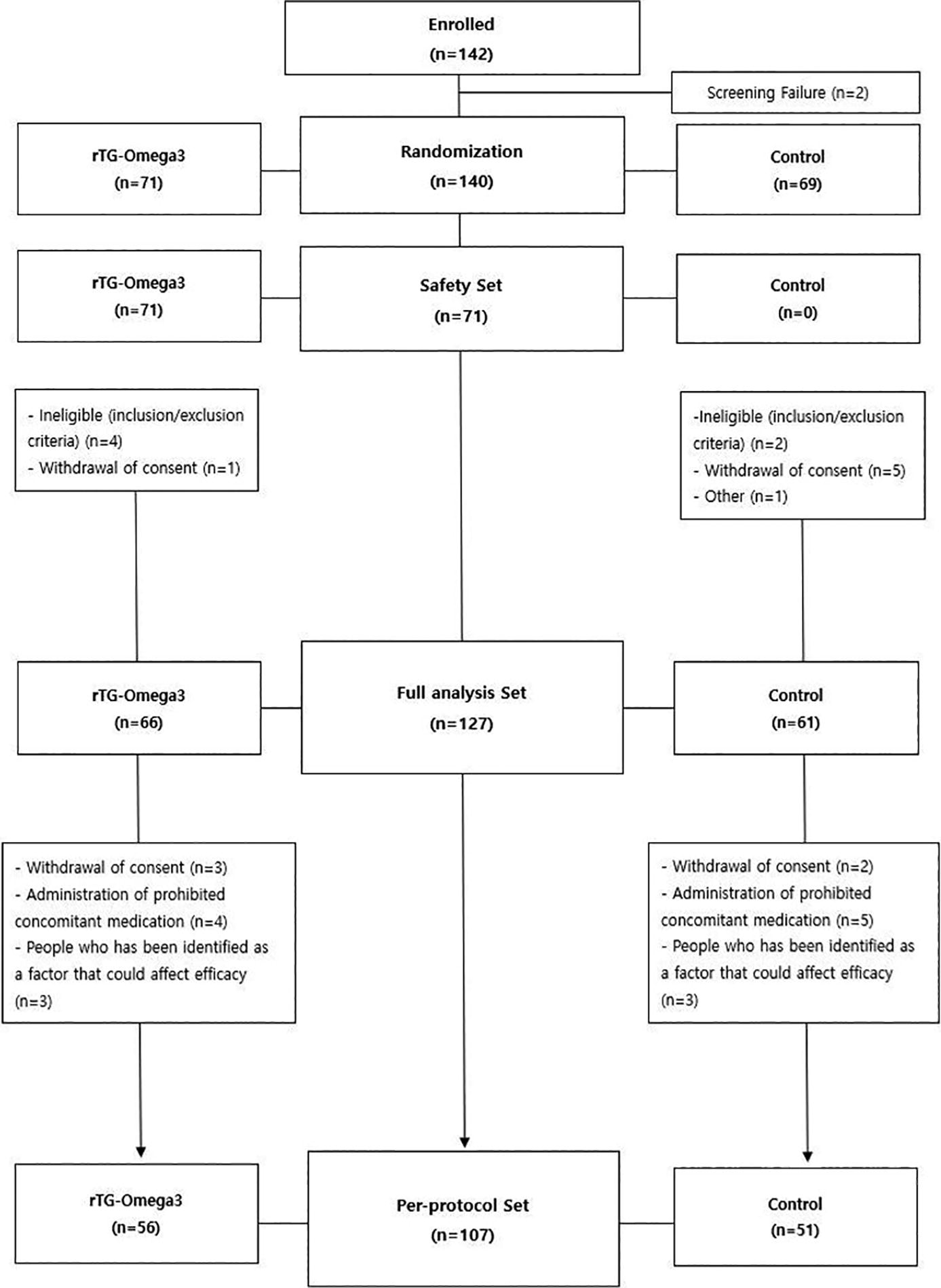
Total 142 patients participated for study screening and 140 patients found to be eligible for the study. Among them, 33 patients were excluded. Finally, 56 patients were included in the rTG-omega 3 supplement group, while 51 patients who only used artificial tear eyedrops without taking rTG-omega 3 supplements were included in the control group. rTG-omega 3, re-esterified triglyceride form of omega 3.
There was no difference in baseline demography and ocular parameters, including TBUT, corneal fluorescein staining score, conjunctival fluorescein staining score, and MGD stage (P = 0.711, P = 0.524, P = 0.477, and P = 0.288) (Table 2).
After 12 weeks, the TBUT of the rTG-omega 3 group tended to be higher, and the difference showed a statistically borderline significant difference (4.99 ± 1.64 s vs. 4.27 ± 1.79 s, P = 0.056) (Table 3; Fig. 2A). The TBUT changes from baseline were significantly different between the two groups (1.98 ± 1.69 s vs. 1.25 ± 1.52 s, P = 0.0158) (Table 4).
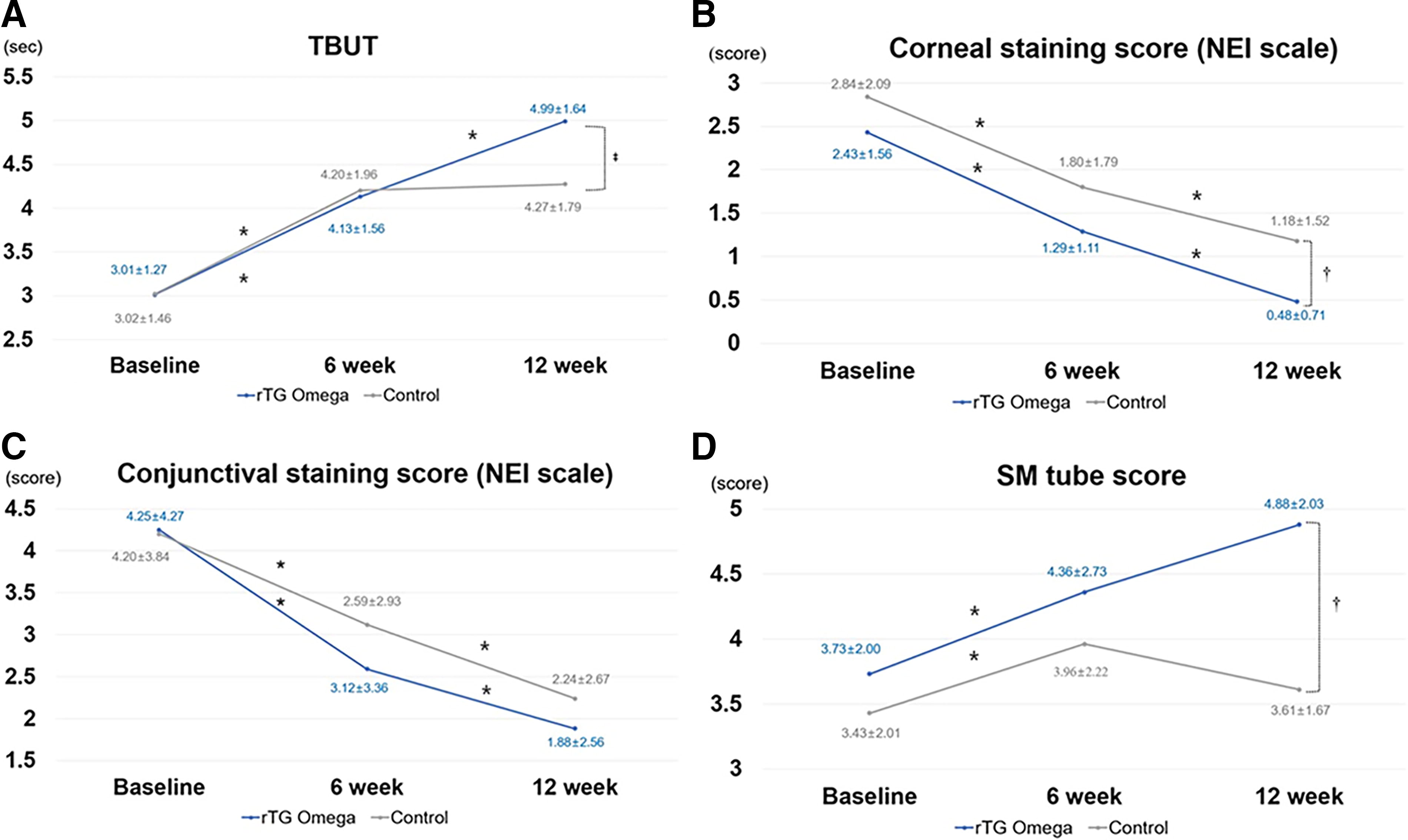
Changes in objective DED parameters over 12 weeks are described in the above graphs. The TBUT was higher in the rTG-omega 3 group, with borderline statistical significance
Comparison of Parameters Used to Evaluate MGD in the rTG-Omega 3 and Control Groups
Wilcoxon rank-sum test.
wks, weeks.
Changes in Parameters from Baseline in rTG-Omega 3 Group and Control Groups
Generalized linear model, which adjusted baseline value.
The corneal fluorescein staining score (NEI scale) at 12 weeks was 0.48 ± 0.71 points in the rTG-omega 3 group and 1.18 ± 1.52 points in the control group, respectively, showing a statistically significant difference (P = 0.006) (Table 3; Fig. 2B). Likewise, the changes from baseline were different between two groups (P = 0.0049) (Table 4).
The conjunctival fluorescein staining score (NEI scale) at 12 weeks was 1.88 ± 2.56 points in the rTG-omega 3 group and 2.24 ± 2.67 points in the control group. The difference was not statistically significant (P = 0.305) (Table 3; Fig. 2C).
The SM tube scores in the rTG-omega 3 and control groups, respectively, were 4.88 ± 2.03 mm and 3.61 ± 1.67 mm at 12 weeks. As such, the score was significantly higher in the rTG-omega 3 group (P < 0.001) (Table 3; Fig. 2C). The change from baseline was also greater in the rTG-omega 3 group (1.14 ± 1.49 mm vs. 0.18 ± 1.80 mm) (P = 0.002) (Table 4; Fig. 2D).
The SPEED score (4.68 ± 3.67 vs. 6.22 ± 4.21) and OSDI score (11.58 ± 10.76 vs. 19.80 ± 16.33) were significantly lower in the rTG-omega 3 group at 12 weeks (P = 0.048, P = 0.003) (Table 3; Fig. 3A and B). Likewise, the change of SPEED score (−3.80 ± 4.20 vs. −2.33 ± 4.71) (P = 0.029) and the change of OSDI score (−11.25 ± 14.66 vs. −7.18 ± 14.78) (P = 0.004) (Table 4) were also significantly greater in the rTG-omega 3 group (Table 4).
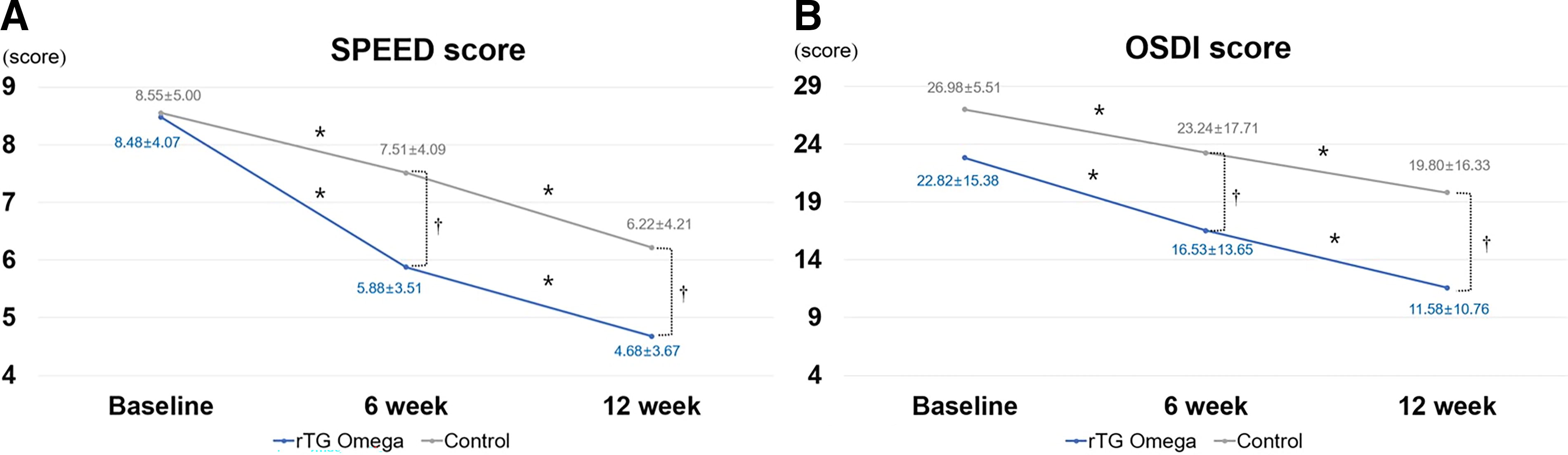
Changes in subjective DED parameters during 12 weeks are presented in the above graphs. Both SPEED and OSDI scores were significantly lower in the rTG-omega 3 group
There was no difference in MGD stage between the two groups at 12 weeks (1.86 ± 0.88 vs. 2.12 ± 0.95, P = 0.146) (Table 3). Also, changes in MGD stage from baseline were not significantly different between the two groups (−0.77 ± 0.76 vs. −0.63 ± 0.72, P = 0.328) (Table 4).
Meibum quality and MG expressibility were also not different between the two groups at 12 weeks (10.91 ± 7.03 vs. 12.69 ± 7.40, P = 0.200) (5.57 ± 2.52 vs. 4.92 ± 2.22, P = 0.111) (Table 3).
In additional subanalysis, we divided the patients according to MGD stage and compared MGD parameters within each group. The MGD parameter values measured at baseline, 6 weeks, and 12 weeks are presented in Table 4. In MGD stage 3 group, rTG-omega 3 patients showed a statistically significant difference in meibomian gland quality compared with control group at 12 weeks, though there was no difference at basement measurement. (P = 0.0348) (Table 5). In this subgroup, the change from baseline was also different between the two groups (rTG-omega 3 vs. control), showing borderline significance (−6.64 ± 5.84 vs. −4.04 ± 5.36) (P = 0.0597) (Table 6). MGD stage 4 patients also showed significantly improved MG quality and expressibility with rTG-omega 3 oral supplementation (P = 0.0226 and P = 0.0143) (Table 5; Fig. 4A and B) Likewise, the changes from baseline in MG quality and expressibility were significantly different between the two groups (−4.36 ± 2.87 vs. −0.57 ± 2.57, P = 0.0177) (2.55 ± 3.08 vs. 0.57 ± 2.44, P = 0.0205) (Table 6).
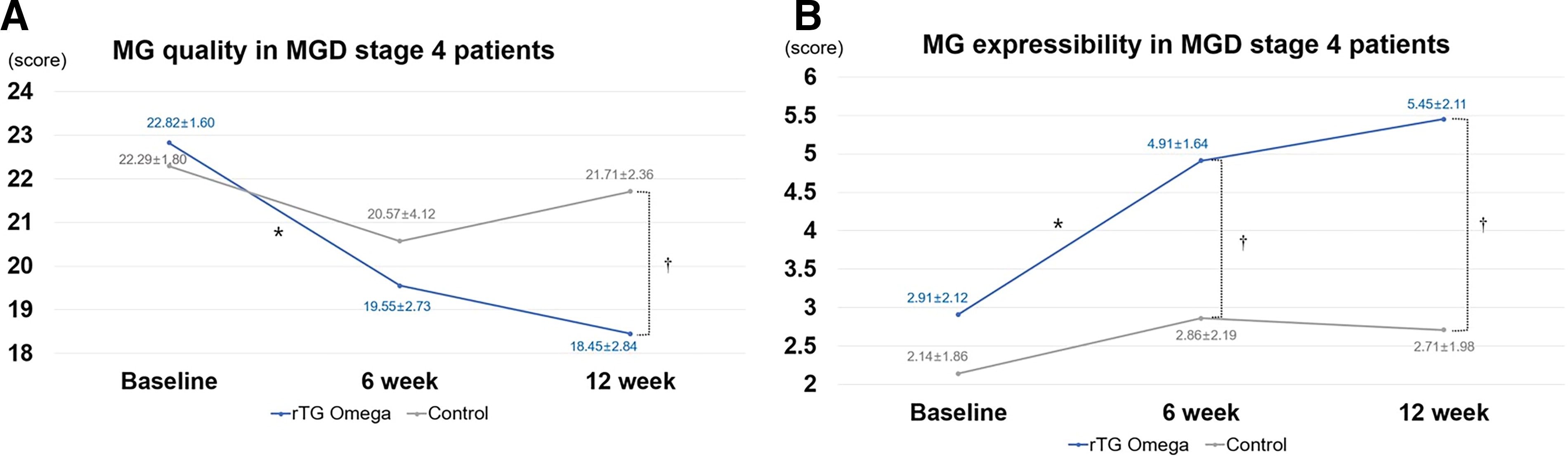
Changes in MG parameters in MGD stage 4 patients during 12 weeks are demonstrated in the above graphs. MG quality was significantly improved in the rTG-omega 3 group after 12 weeks of supplementation
Comparison of MGD Parameters according to MGD Stage between Omega 3 and Control Groups
Wilcoxon rank-sum test.
Two-sample t-test.
Changes in MGD Parameters according to MGD Stage after 12 Weeks
Generalized linear model (GLM), which adjusted baseline value.
Discussion
Cataract surgery is one of the most commonly performed surgeries worldwide. However, during and after surgery, many risk factors for DED aggravation present, including the corneal incision performed during cataract surgery, postoperative nonsteroidal anti-inflammatory use, and exposure to the laser light during the procedure.29–31 A previous study demonstrated that meibum quality in particular was significantly decreased after cataract surgery. 32 A reduced quality of meibum increases tear instability and leads to evaporative DED. It can also cause tear hyperosmolarity, which can facilitate inflammation of the ocular surface. 3
This study demonstrated that rTG-omega 3 supplementation can improve objective DED parameters, including TBUT and SM tube score. We believe that changes in the fatty acid composition of meibum affect the result. Previous studies have suggested that omega 3 intake increases the proportion of unsaturated fatty acids in meibum.11,33 Due to its property of maintaining a liquid state at body temperature, meibum tends to be easily secreted from the glands. 11 It prevents evaporation, leading to increased tear volume. A study by Park et al. reported no significant improvement in TBUT in patients with DED supplementing with rTG-omega 3, 13 even though subjective symptoms were decreased. In the current study, both aspects were improved, demonstrating that rTG-omega 3 supplementation is effective for addressing both objective and subjective parameters in DED associated with MGD after cataract surgery. We suggest that the difference in our results from those of the previous study may be attributed to the type of patients with DED we enrolled. The previous study investigated different patients with DED, including those with aqueous-deficiency DED, which is relatively less influenced by improvements in MG function. Therefore, the results of this study suggest that rTG-omega 3 supplementation may be more beneficial for DED associated with MGD.
There was no significant difference in MGD stage quality or expressibility between the rTG-omega 3 group and the control group. However, in the additional analysis, significant differences in MG quality and expressibility were observed in the MGD stage 4 group. This suggests that, in cases of mild MGD, improving tear stability by hyaluronic acid (HA) alone can lead to significant therapeutic effects. However, in severe cases, HA alone is not sufficient, and there may be a necessity for another mechanism to block the vicious cycle in DED.11,13,33 We also believe the anti-inflammatory nature of omega 3 played a critical role. In DED, tear instability leads to hyperosmolarity, which triggers inflammatory responses on the ocular surface. This inflammation stimulates epithelial cells to produce inflammatory cytokines like MMP-9, IL-1a, and IL-1b, 34 which promote epithelial proliferation and keratinization of MGs, leading to tear instability again. 3 Previous studies have recorded decreased MMP-9 concentrations in omega 3 supplementation groups. The omega 3 fatty acid EPA and the omega 6 fatty acid AA competitively participate as substrates for the enzymatic activities of cyclooxygenase and 5-lipoxygenase. 35 The mechanism underlying the anti-inflammatory effect is hypothesized to arise from the of prostaglandin E3 and leukotriene B5 originating from EPA, thereby inhibiting the conversion of AA into potentially harmful inflammatory mediators, such as prostaglandin E2 and leukotriene B4.16,17 Likewise, MGD society guidelines have recommended different treatment approaches for individual MGD stages and highlight the importance of anti-inflammatory therapy in stage 4 cases. 3
The subjective questionnaire responses and objective parameters in this study revealed significant improvement differences after 12 weeks of supplementation compared with 6 weeks of supplementation. Several previous studies also reported that omega 3 supplementation demonstrated effectiveness in longer periods, and the results of this study support the need for longer supplementation periods >12 weeks.10,11,13
A strength of this study is that it was a randomized, multicenter, investigator-blind study. Furthermore, we analyzed the effectiveness of rTG-omega 3 supplementation after cataract surgery and included only one specific type of DED. We also divided patients with MGD according to severity and compared treatment effectiveness between these groups, which has never been done before.
A limitation of this study is that we did not administer a placebo to the control group, which could have affected the results, including subjective questionnaires.
Several parameters, including the primary outcome, exhibited borderline significance ranging from 0.05 to 0.10. While we considered that these statistics might hold clinical significance, their interpretation could introduce subjectivity.
Additionally, in this study, we solely examined the adherence to r-TG omega 3 among patients and did not perform the analysis of omega 3 index, which measures intra-body omega 3 levels, or meibum contents. Therefore, we suggest that future studies include more objective indicators to demonstrate the correlation between the omega 3 index and improvements in ocular parameters.
In conclusion, in this study, rTG-omega 3 oral supplementation led to improvements in both objective signs and subjective symptoms, with no significant difference in MGD parameters between the two groups. However, when we divided patients according to MGD stage, the group with the most severe MGD stage showed improvements in MG quality and expressibility. Therefore, we suggest that rTG-omega 3 supplementation may benefit patients with DED with MGD, especially those with more severe MGD.
Footnotes
Authors’ Contributions
J.S.S. was involved in the conception and design of the study. M.W., Y.E., H.K.K., K.C.Y., K.S.N., K.J.C., H.K.L., and J.S.S. were involved in data collection and literature research. S.H. was involved in the interpretation and critical revision of the article. J.S.S. was involved in the data analysis and drafting of the article. M.W., Y.E., H.K.K., K.C.Y., K.S.N., K.J.C., H.K.L., and J.S.S. were involved in the final approval of the article.
Author Disclosure Statement
All authors certify that they have no financial disclosures.
Funding Information
This study was funded by Taejoon Pharm (Seoul, Republic of Korea).