
Abstract
Purpose:
Topical tacrolimus is currently used in ocular surface pathologies as a corticosteroid-sparing immunosuppressive agent. It could also help prevent endothelial corneal graft rejection and inflammatory diseases; however, its hydrophobic nature and high molecular weight theoretically limit its intraocular penetration. The aim of this study is to investigate the corneal and intraocular penetration of a 0.1% tacrolimus ophthalmic suspension.
Methods:
Sixteen rabbits were randomly spread into four groups defined by the delay between the last tacrolimus instillation and corneal sampling (2, 6, 11, and 24 h). Three rabbits per group received bilateral instillations of tacrolimus twice daily for 5 days, the 4th subject in each group serving as negative controls. The 5th day, conjunctiva, corneal epithelium, anterior stroma, posterior stroma, corneal endothelium, iris, choroid/retina, aqueous humor, and plasma samples were collected. Tacrolimus concentrations were determined using high-performance liquid chromatography coupled with tandem mass spectrometry.
Results:
Maximum mean concentration was reached after 2 h in the epithelium, anterior and posterior stroma, and endothelium: 12794 (±2656), 436 (±178), 341 (±179), and 4125 (±1673) ng/g, respectively. The descending rank order of exposure over 24 h was: corneal epithelium; corneal endothelium; conjunctiva; anterior stroma; posterior stroma; iris; and chorioretina with 158.0; 39.99; 4.620; 4.134; 3.350; 0.384; 0.270 ng.h/mg, respectively.
Conclusions:
Tacrolimus concentrations measured in the corneal tissues are significantly higher than that described as lower limit of efficacy in solid organ transplantation. Topical 0.1% tacrolimus could therefore become an alternative to corticosteroids for endothelial graft rejection prevention and endothelial inflammatory pathologies management.
Introduction
Tacrolimus was first isolated in 1987 from strains of Streptomyces tsukubaensis, a bacterium found in soil, by Kino et al. 1 This discovery led to the development of the immunosuppressive agent FK506, used in organ transplantation to prevent graft rejection. 2 Tacrolimus is a macrolide immunosuppressant of the calcineurin inhibitor class. Its mechanism of action is based on its ability to bind to an intracellular protein called FKBP (FK506-binding protein), forming a tacrolimus-FKBP complex. This complex specifically inhibits the activity of calcineurin, a crucial calcium phosphatase for T-cell activation. By blocking this signaling pathway, tacrolimus reduces the production of pro-inflammatory cytokines such as interleukin-2 (IL-2), thereby suppressing the adaptive immune response.3,4 Its efficacy in solid organ graft rejection prevention has been shown for tissular concentrations above the threshold concentration (Cthreshold) of 100 ng/g. 5
Animal studies have shown a benefit of topical tacrolimus compared to a placebo in penetrating keratoplasty graft failure prevention.6–8 This would also help reduce the risk of known ocular side effects associated with steroid use, such as an increase in intraocular pressure and cataract development, which are major concerns in the long-term management of patients undergoing treatment with topical corticosteroids.
Systemic tacrolimus has demonstrated efficacy in reducing graft rejection in high-risk corneal transplants in studies involving humans, and topical tacrolimus is already successfully used for its immunosuppressive properties in various inflammatory dermatological and ocular conditions as a corticosteroid-sparing agent.9–14 While current data supports topical tacrolimus use for superficial diseases, its effectiveness on deeper stromal and endothelial pathologies remains debated. In corneal transplantation, typically managed with topical corticosteroids, tacrolimus suspension offers a promising alternative.15–17 A pilot study comparing topical FK506 to local steroids after normal-risk penetrating keratoplasty yielded encouraging results, though with limited patient numbers and concurrent steroid use. 18
Due to its highly hydrophobic nature and its molecular weight of 822 Da, deep corneal penetration of tacrolimus is uncertain. This study aimed to measure the intraocular and intracorneal penetration, layer by layer, of a 0.1% tacrolimus suspension in an animal model.
Methods
Animals
New Zealand white female rabbits, aged 77 days, weighing between 2.0 and 2.5 kg were purchased from the C.E.G., A.V farm, Approval No. B-28–010-01, Argenvilliers (France). Rabbits were kept at a room temperature of 18°C–21°C and humidity of 40%–60%, with a 12 h/12 h dark/light cycle, 14 days before the experiment. Food and water were supplied ad libitum. A comprehensive health assessment, including an eye examination, was performed on all rabbits, and only those confirmed to be in good physical condition and free from any overt ocular defects were used in the study. All animal experiments were approved by the French Authorities, Approval No. DAP#34274.
All experiments were conducted in adherence to the statement of the Association for Research in Vision and Ophthalmology (ARVO) for the Use of Animals in Ophthalmic and Vision Research and the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines.
Study drug
Tacrolimus 0.1% ophthalmic suspension (Talymus®, Senju Pharmaceuticals Co Ltd, Japan). It is a sterile, tacrolimus hydrate aqueous suspension for topical ophthalmic use, also containing partially hydrolyzed polyvinyl alcohol, benzalkonium chloride, sodium chloride, dibasic sodium phosphate hydrate, sodium dihydrogen phosphate dihydrate, phosphoric acid, and sodium hydroxide as inactive ingredients.
Drug administration and sample collection
This study was carried out on a total of 16 rabbits, divided into groups of 4 according to the delay between the last tacrolimus instillation and the corneal sampling (2, 6, 11, or 24 h, n = 4). One drop of the tacrolimus 0.1% suspension was administered into both eyes of 3 subjects per group. Both eyes of the 4th subject of each group were kept as a negative control. The eye drops were instilled twice a day, i.e., 8:00 AM and 6:00 PM, during 5 days.
Briefly, the lower eyelid was gently pulled away from the eye globe, and ∼ 50 μL of the formulation was applied in the lower conjunctival cul-de-sac. After instillation, the upper and lower eyelids were hand-held together for ∼ 5 s to permit the formulation to come into contact with the cornea.
On the 5th day, at the predetermined time points, the blood sample was drawn (1 mL) through the marginal ear vein using a 24-gauge catheter left in place. After blood collection, the rabbit was pre- anesthetized with isoflurane 5%/oxygen 100%, then sacrificed with an intravenous injection (5 mL) of 1% propofol followed by thiopental (0.5g). Conjunctival tissue was sampled using a Troutman forceps and Vannas scissors. Aqueous humor samples were drawn using a 30-gauge needle. Corneal samples were retrieved by making a 360° transfixing scleral incision 3 mm from the limbus with a 15° blade, followed by circular cutting with Vannas scissors. This allowed for the removal of the cornea along with the scleral ring, without any manipulation of the corneal tissue. The iris and lens were then excluded. This sampling method, identical to that used in corneal graft procurement, ensured the preservation of the tissue’s structural integrity. Corneal sampling was carried out by dissecting the epithelium, anterior stroma, posterior stroma, and endothelium. First, the corneal epithelium was removed with a Desmarres knife. The corneal endothelium was then carefully removed using another Desmarres knife. After placing the residual corneal sample on an artificial anterior chamber, an intrastromal pocket was then performed at mid-stromal thickness by an experienced corneal surgeon using dissecting knives, and the anterior stroma was progressively separated from the posterior stroma. Finally, iris and chorioretinal samples were individualized using a Troutman forceps, generating a total of 204 samples. All obtained samples were then stored in methanol at −80°C until analysis.
Clinical examination
Clinical evaluation included ocular inspection of the eyelids, conjunctiva, and cornea before and after each instillation and before dissection.
Sample preparation and analysis procedure for tacrolimus quantification
Cornea samples were collected using weighted tubes, each containing two hundred microliters of methanol. Tubes were weighted before and after sampling. Tacrolimus extraction was performed by vortexing the mixtures for 10 s, followed by sonication for 15 min and centrifugation.
Tacrolimus concentration in each sample was quantified using a fully validated method dedicated to the determination of blood immunosuppressants in clinical practice by high-performance liquid chromatography coupled with tandem mass spectrometry (HPLC-MS/MS). The chromatographic system consisted of a Prominence Shimadzu UFLC system (Shimadzu®, Prominence, Kyoto, Japan) in combination with a 3200QTRAP equipped with an electrospray ionization source operating in positive ion mode (Sciex®, Toronto, Canada). Briefly, 100 µL of each supernatant was mixed with 200 µL of a solution containing methanol/ZnSO4 5% (m/m) spiked with the internal standard tacrolimus-13CD2 (tacrolimus-d3, 40 ng/mL) in order to address potential matrix effects, as is typically performed for this type of analysis.19,20 After centrifugation at 3000 rpm for 5 min, 200 µL of the supernatants were collected and directly injected in the LC-MS/MS system. Quantitation was performed using the following precursor-ion to product-ion transitions (quantitation/qualification): tacrolimus m/z 821.5 → 768.5/821.5 → 786.5, and 824.5 → 771.5 for the deuterated tacrolimus-d3. Chromatographic separation was achieved on an Alltima HP C18HL analytical column (2.1 μm particle size, 50 mm length × 3 mm inner diameter; VWR International®, France) after online extraction using a Poros R2/20 (20 μm particle size, 30 mm length × 2.1 mm inner diameter; Applied Biosystems®, France). The auto-sampler temperature was set at 8°C, the column oven at 60°C, the injected volume was 40 μL, and the isocratic flow rate was 200 μL/min. The mobile phase consisted of aqueous 15 mM ammonium acetate buffer (solvent A) and 10 mM ammonium acetate buffer/0.1% acetic acid in methanol (solvent B). Chromatographic data acquisition and processing were performed using the Analyst v1.6.32.7 software (AB Sciex®).
The analytical procedure used in this study met international analytical requirements according to ISO 15189, EMA, and FDA guidelines on bioanalytical method validation. The limits of quantification and detection of the method were 1.4 ng/mL and 0.4 ng/mL, respectively. Calibration curves ranged from 1.4 to 40.0 ng/mL for tacrolimus quantification. The accuracy ranged from 85% to 115%, and the intraday and interday precision were lower than 15%.
Pharmacokinetic parameters
Measured pharmacokinetic parameters in this study included maximum tacrolimus concentration (Cmax), time to reach Cmax (Tmax), area under the concentration–time curve (AUC2-24h) from first to last measurable concentrations (2–24 h). Cmax and Tmax were obtained directly from the observed data. Pharmacokinetic parameters were analyzed using Microsoft Excel (Version 16.90).
Results
The mean (±standard deviation) concentration values for each studied ocular tissue are given in Table 1. Significant levels of tacrolimus are found in all four studied corneal layers throughout the 24-h study period. The proportion of samples with a tacrolimus concentration above Cthreshold (100 ng/g) is presented in Figure 1.
Mean (±Standard Deviation) Tissular Concentrations (ng/g) of Tacrolimus Over Time
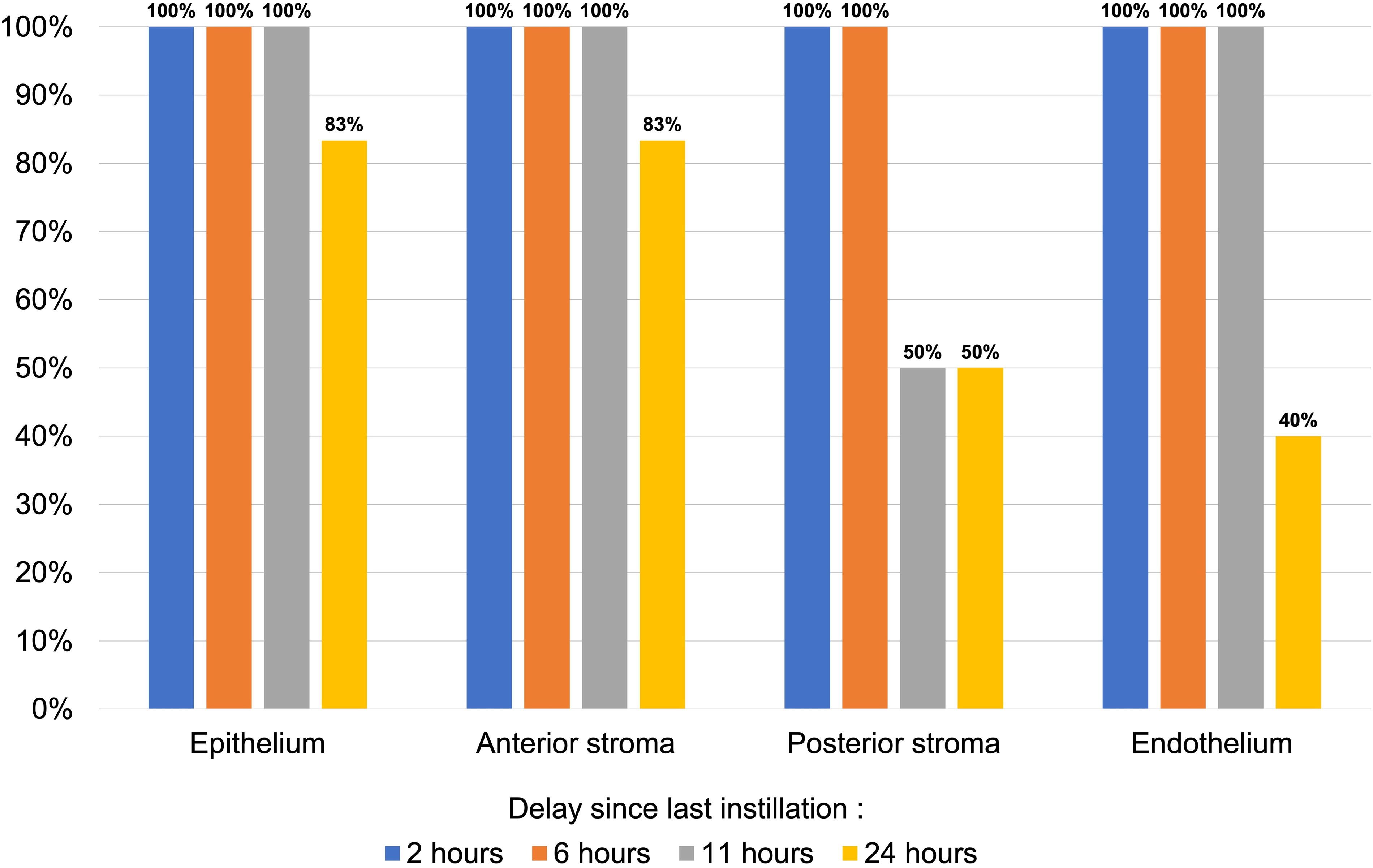
Proportion of samples with concentration above Cthreshold (100 ng/g). Cthreshold, threshold concentration.
The PK parameters for the distribution of tacrolimus in corneal tissues after repeated instillations are presented in Table 2. The results showed that the maximum concentration (Cmax) of tacrolimus in the different ocular tissues was achieved within 2 h after last instillation, except for the corneal endothelium in which the Cmax was obtained 6 h after instillation. The ocular tissue exposure was characterized by the area under the concentration curve (AUC2-24h) Highest values were measured in the corneal epithelium and endothelium. The rank order of exposure as measured by AUC2-24h in ocular tissues after repeated instillations of tacrolimus 0.1% suspension was, in descending order, as follows: corneal epithelium, corneal endothelium, conjunctiva, anterior stroma, posterior stroma, iris, and chorioretina.
Ocular Pharmacokinetic Parameters of Tacrolimus
AUC2-24h, area under the concentration-time curve from 2 to 24 h after last instillation; Cmax, maximum tacrolimus concentration; Tmax, time to the maximum tacrolimus concentration.
Tacrolimus was also found in the aqueous humor and plasma at the 2-h timepoint in three samples, with a mean (±standard deviation) concentration of 1.313 (±0.895) ng/mL and 0.673 (±0.162) ng/mL, respectively, and at the 6-h timepoint in one sample with a measured concentration of 1.680 ng/mL and 0.510 ng/mL, respectively. All other aqueous humor and plasma samples had a null or below quantification level tacrolimus concentration.
Safety assessment
The treated rabbits exhibited health outcomes comparable to those of the control group throughout the study. Both groups maintained stable body weights and displayed no signs of discomfort or adverse reactions. Ocular health was assessed using the McDonald-Shadduck scoring system. 21 Specifically, there were no corneal opacity, ulceration, redness of the nictitating membrane, discharge, hypopyon, chemosis, conjunctival inflammation, or any other ocular abnormality. Upon examination on dissection day, the eyes of the treated rabbits were in a comparable condition to those of the control group, with no observable differences between the two groups.
Discussion
Our study results confirm that tacrolimus penetrates the full thickness of the cornea, from epithelium to endothelium, after twice-daily topical instillation of a tacrolimus 0.1% ophthalmic suspension during 5 days. To our knowledge, this measurement of tacrolimus concentration has not been conducted before. However, determining the concentrations in each corneal layer is fundamental due to the cornea’s structure, which can restrict the penetration of many molecules. We also found discrete, yet non-null, concentrations of the study drug in the aqueous humor during the first 6 h after instillation, suggesting that the cornea acts as a retaining tissue for tacrolimus while gradually clearing it via aqueous humor drainage. This clearing process most likely continues beyond the first 6 h; however, we did not manage to demonstrate this, possibly because our quantification threshold was above the actual concentrations. These results are consistent with those obtained by Fujita et al. who observed the penetration of a 14C-tacrolimus 0.3% suspension, without measurement in each individual corneal layer. 22
While using eye drops directly from the vial of a commercially available formulation may result in less precise volume calibration, this approach closely mirrors real-world clinical conditions. Additionally, our pharmacokinetic investigation in rabbit ocular tissues showed that this formulation could maintain adequate tacrolimus concentrations in all corneal layers for up to 24 h after instillation. Tacrolimus concentrations remain high over the 24-h study period, regardless of the corneal layer, and maintain above the efficacy threshold in solid organ graft rejection prevention (Cthreshold = 100 ng/g) during the first 6 h in all studied corneal samples and during the first 11 h in all corneal endothelium samples. The peak concentration is attained 2 h after instillation in every studied tissue except for the corneal endothelium (6 h) and then decreases over the 24-h study period, similarly to the findings of Pleyer et al. in their whole cornea analysis. 23
In high-risk settings, the prevention and management of corneal graft rejection involve the use of topical corticosteroids combined with topical cyclosporin A in 48% to 77% of cases, though Javadi et al. reported no significant benefit from adding 2% ciclosporin A.16,24 Given tacrolimus’s 50 to 100 times higher immunosuppressive potency compared to ciclosporin A, exploring its intracorneal penetration is a crucial step towards safer ocular immunosuppression.25–31 We found the epithelial and endothelial layers of the cornea to have an exposure to tacrolimus over 10-fold superior to that of the stromal layers. This can be explained by the hydrophobic nature of the study drug, both limiting its affinity with the electronegative and hydrophilic stromal compartment and enhancing its intracellular penetration into these two highly cell-populated layers of the cornea through their high density of lipidic cell membranes. This elevated concentration in the endothelial layer combined with its higher potency than that of ciclosporin could provide a clear benefit in preventing and managing endothelial graft rejections that ciclosporin struggles to counter according to Price et al. and Javadi et al.24,32
Moreover, it is important to note that ciclosporin exists in various formulations, each with distinct pharmacokinetic profiles. 33 This variability challenges the assessment of ciclosporin’s efficacy, particularly in terms of its penetration and activity in the deeper corneal layers, and raises questions about the conclusions drawn regarding good ciclosporin penetration in similar studies.
Plasmatic tacrolimus concentration, although non-null during the first 6 h after instillation, is well under the toxicity threshold (15.0 ng/mL) and the target residual concentration in solid organ transplantation (7.0 ng/mL) throughout the 24-h study period.34,35 These results are similar to those of other studies but in opposition with the findings of Yuan et al. who did not find any systemic absorption.22,36,37 Also, this is aligned with the results of Daeschler et al. who did not find any tacrolimus in the vital organs of rats after 4 weeks of topical ocular tacrolimus treatment. 38
Rabbits stand as the most convenient and frequently employed animal model for assessing the pharmacokinetic profile of eye drop formulations. 39 Nonetheless, its predictive ability regarding tissue penetration in clinical scenarios is not always reliable. Given that endothelial keratoplasties (EK) are now the most common corneal grafts in many countries and involve only endothelial rejections, we chose to study tacrolimus penetration in healthy eyes to better simulate the target model and therefore best align with the clinical setting in which this treatment could be prescribed.40,41 Indeed, in many cases, EK is replacing penetrating keratoplasties due to its lesser impact on the corneal stromal structure, which could potentially limit topical drug penetration postoperatively. The recipient cornea in EK more closely resembles a healthy cornea than a trephined one, making this approach more accurate.
The current data provide insights into the local distribution of tacrolimus through the cornea, revealing effective tacrolimus concentrations throughout the 24-h study period. Our results demonstrate that the studied suspension is effective in delivering tacrolimus to the deep corneal layers. From this, it can be inferred that a topical tacrolimus 0.1% suspension might serve as a viable option for preventing endothelial graft rejection and treating stromal and endothelial inflammatory diseases by a sustained modulation of local immune activity.
Footnotes
Acknowledgments
The authors wish to thank David Toubeau, head of Tissue Preparation at the Rouen University Hospital, and his team for their help in preparing the tissue sampling. The authors also thank the Pharmacology department technicians of the Rouen University Hospital for their precious help in sorting and analyzing each of our numerous samples.
Authors’ Contributions
M.Q.: Conceptualization of study; data collection; data interpretation; original draft writing, revisions, and approval of the article. F.L.: Data collection; data interpretation; critical review, revisions, and approval of the article. C.A.: Data collection; critical review, revisions, and approval of the article. G.G.: Conceptualization of study; critical review, revisions, and approval of the article. A.G.: Data collection; data interpretation; critical review, revisions, and approval of the article. T.C.: Data collection; data interpretation; critical review, revisions, and approval of the article. M.M.: Conceptualization of study; data collection; data interpretation; critical review, revisions, and approval of the article. J.G.: Conceptualization of study; data collection; data interpretation; critical review, revisions, and approval of the article. All authors had full control of the content and made the final decision on all aspects of this publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was partly funded by Théa laboratories. The funder had no role in the design, analysis, or the interpretation of results.