
Abstract
Purpose:
The aim of this study was to identify and quantify the occurrence of corneal deposits caused by medications, utilizing data from the Food and Drug Administration Adverse Event Reporting System (FAERS).
Methods:
We conducted a retrospective analysis of the national FAERS database, focusing on instances of drug-induced corneal deposits reported between 2004 and the third quarter of 2023. Our methodology included applying the proportional reporting ratio, reporting odds ratio, empirical Bayes geometric mean, and information component in our disproportionality analysis. A signal was considered present if all four of these disproportionality metrics showed positive results.
Results:
Over the span of 20 years, our research identified 383 adverse event reports linked to corneal deposits associated with 349 different medications. The most common age-group of these reports involved patients over 65 years of age (32.4%), with equal distribution between male (40.0%) and female (42.8%) patients. Thirty-one medications showed a positive signal. Notably, drugs such as amiodarone (68 reports), prednisolone (60 reports), and timolol (54 reports) were most frequently mentioned. Cyclopentolate and chloramphenicol demonstrated robust statistical relevance in association with corneal deposits.
Conclusions:
Positive signals for drug-induced corneal deposits included both well-known medications such as amiodarone and lesser-studied medications such as prednisolone and timolol. Clinician awareness of these findings alongside further investigation is needed.
Introduction
The cornea safeguards the eye from harmful ultraviolet radiation, prevents the entry of foreign objects or substances, and facilitates the precise refraction of incoming light. 1 Pathologies that impact the cornea can be complex and systemic in nature. One particularly relevant pathology includes corneal deposits.2,3 Corneal deposits entail the accumulation of abnormal material within the layers of the cornea. 4 Individuals affected by corneal deposits may manifest either asymptomatic presentations or exhibit symptoms such as diminished visual acuity and ocular discomfort. While corneal deposits may arise due to inherent anomalies, such as Fabry disease or multiple myeloma, 4 an important, alternative consideration is that of drug administration. 5 Understanding iatrogenic corneal deposits is particularly important because while discontinuation can result in resolution in the majority of cases, cessation must be weighed against the risks of underlying disease. 6
An array of medications has been demonstrated to be linked with corneal opacities, including agents such as amiodarone, tamoxifen, atovaquone, and fluoroquinolones. 7 Drugs from many pharmacologic classes are associated with various patterns of corneal depositions. 6 For example, medications with cationic amphiphilic structures can effect intracellular phospholipid accumulation/vortex keratopathy, whereas antineoplastic agents can produce a diffuse corneal haze, while others are associated with crystalline precipitations.
Although there are systematic reviews and other small-scale studies evaluating corneal deposits, their pathophysiology, and their treatment options, there is a general lack of analyses evaluating drug-induced corneal deposits at a national scale. 6 In this article, we seek to evaluate real-world data from the Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) database to both derive novel insights on the effects of current pharmacotherapies and highlight potential avenues for future research and investigations.
Methods
Data source
In this retrospective study, we utilized data from the FAERS, a national database maintained by the U.S. FDA. FAERS contains comprehensive information on adverse events and medication errors associated with FDA-regulated drugs and therapeutic biological products. The database includes details such as the type and severity of adverse events, patient demographics, drug information (name, dosage, and administration route), and outcomes of reported events.
FAERS is a publicly available resource accessible through quarterly data files or public dashboards provided by the FDA. Its purpose is to monitor and evaluate potential safety concerns related to approved medications on the market. The data in FAERS come from voluntary reports submitted by health-care professionals, patients, and drug manufacturers. It serves as a valuable tool for monitoring drug safety and adverse event surveillance, especially for capturing rare or long-term adverse events that may not initially be evident in clinical trials.
Data collection
In this study, FAERS case reports from 2004 to the conclusion of the third quarter of 2023 were selected. We identified 383 corneal deposit adverse event reports associated with approximately 349 drugs. OpenVigil—a validated data extraction, cleaning, and mining tool—was utilized in accordance with FDA recommendations to eliminate duplicate entries based on case numbers. 8 To identify corneal deposit adverse events, we used the preferred term (PT) “corneal deposits” (PT: 10010999) from the Medical Dictionary for Regulatory Activities.
Statistical analysis and signal detection
First, a descriptive analysis was conducted to summarize the clinical features of corneal deposit cases, encompassing patients’ age, gender, and reporting country (Table 1). Based on the aggregate report counts for each specific drug, all drugs with five or more reports associated with corneal deposits were identified (Fig. 1). As such, 55 drugs were included from a total of 349 drugs. These 55 medications were grouped for ease of interpretation by antiarrhythmic status, immunosuppressant status, ocular medications, antibiotics/antivirals, and others (Supplementary Table S1, Supplementary Fig. S1).
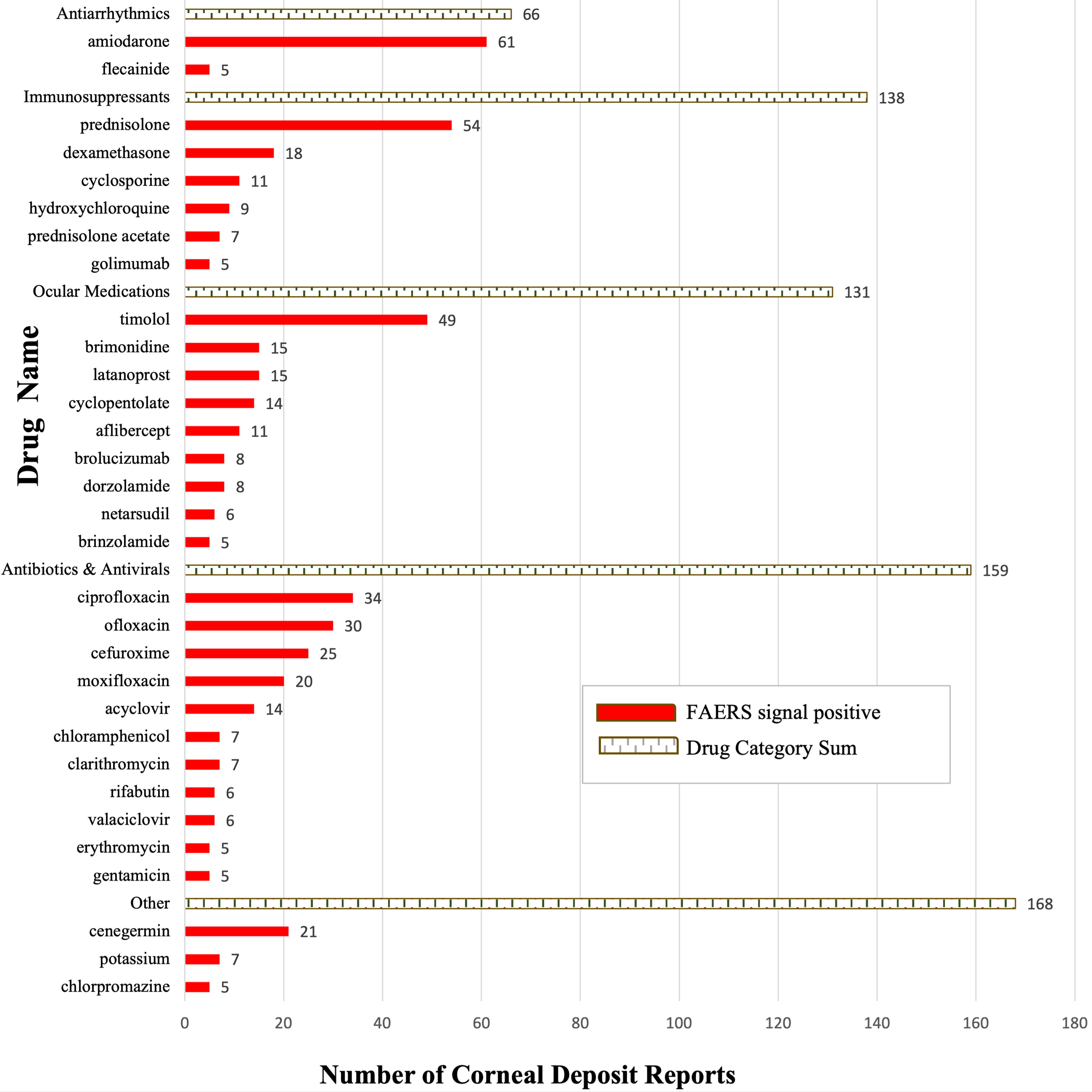
Listing of positive signals from the 55 most common drugs for drug-induced corneal deposits on FAERS. FAERS, Food and Drug Administration Adverse Event Reporting System.
Characteristics of Cases with Corneal Deposits
Disproportionality analysis was then conducted to investigate the association between corneal deposit adverse effects and all drugs in the FAERS database (Table 2). The aim of this analysis was to identify adverse drug signals from FAERS, enabling the differentiation between authentic drug–adverse event associations and coincidental co-occurrences. To identify such signals, we utilized four data mining algorithms: reporting odds ratio (ROR), proportional reporting ratio (PRR), empirical Bayes geometric mean (EBGM), and information component (IC). The stringent criteria for identifying a positive drug signal were that all algorithms produce significant values (PRR ≥2.0 with χ2 ≥ 4, ROR 95% confidence interval [CI] >1.00, EBGM05 > 2.0, IC025 > 0 with n ≥ 3). The statistical techniques and criteria employed in these methods have been extensively described and studied in prior literature.9–12 Notably, four algorithms were utilized. The PRR and ROR are two frequentist algorithms based on the assumption that probabilities are fixed and objective; most notably, the PRR is similar to the old proportional mortality ratio, whereas the ROR is a slightly newer metric allowing for estimations of relative risk when the outcome in choice is rare. 13 In contrast, the EBGM and IC are Bayesian techniques, which assume that probabilities change based on new information. The IC was originally derived using a Bayesian confidence propagation neural network, with the express intent of designing a tool to find drug–adverse drug reaction combinations in the midst of many other variables. 11 The derivation behind the EBGM and its algorithmic calculation has been detailed in past papers; of note, the EBGM has been demonstrated as the most conservative algorithm. 12 All statistical analyses were conducted using SPSS Statistics Version 25.0 (IBM Corporation, Armonk, NY) and Microsoft Excel (Microsoft Corporation, Redmond, WA).
PRR (χ2), ROR (95% CI), EBGM (EBGM05), and IC (IC025) for All Positive Signals
CI, confidence interval; EBGM, empirical Bayes geometric mean; FAERS, Food and Drug Administration Adverse Event Reporting System; IC, information component; PRR, proportional reporting ratio; ROR, reporting odds ratio.
Results
During our study period, a total of 383 reports of corneal deposits adverse effects were identified. While 37.4% of reports did not include an age, reports that did include age most commonly involved patients aged 65 or older, who accounted for 32.4% of the cases. Furthermore, a similar proportion of females (42.8%) exhibited corneal deposits compared with males (40.0%), and the most common country of reported cases was the United States (33.9%). Additional findings are available in Table 1.
Of the most common drugs associated with corneal deposits, 31 drugs yielded positive signals, as depicted based on the total counts of adverse event reports in Figure 1. Amiodarone (61 reports), prednisolone (54 reports), timolol (49 reports), ciprofloxacin (34 reports), ofloxacin (30 reports), and cenegermin (21 cases) were among the most frequently reported drugs in association with corneal deposits and accounted for over half of all analyzed reported cases.
Notably, both antiarrhythmics (amiodarone and flecainide) evaluated in this analysis yielded positive signals (Table 2). From immunosuppressive medications, prednisolone, dexamethasone, cyclosporine, hydroxychloroquine, prednisolone acetate, and golimumab yielded positive signals. Notably, all evaluated ocular medications (inclusive of timolol, brimonidine, and latanoprost, among others), all antibiotics (inclusive of ciprofloxacin, ofloxacin, cefuroxime, and chloramphenicol), and both antivirals (acyclovir and valacyclovir) yielded positive signals. Finally, cenegermin, potassium, and chlorpromazine yielded a positive signal.
Utilizing four previously described data-mining algorithms (Table 2), disproportionality analysis enabled the identification of statistically positive signals. Cyclopentolate had a notable statistical positive with corneal deposits (n = 14; PRR: 612.5; ROR: 624.5; EBGM: 590.1; IC: 9.2), as did chloramphenicol (n = 7; PRR: 267.1; ROR: 269.4; EBGM: 262.2; IC: 8.3).
Discussion
In this study, a comprehensive investigation was carried out on all drugs associated with corneal deposits utilizing a pharmacovigilance database. Although not all corneal deposits present a substantial threat to vision, certain instances may lead to vision loss or give rise to complications such as painful corneal erosions. 14
A range of case reports and previous prospective studies have been documented concerning drugs such as netarsudil, 15 antimalarial drugs, 16 tamoxifen, 17 and chlorpromazine. 18 While a comprehensive interpretation of these associations remains challenging primarily due to the constraints posed by limited sample sizes or dated studies, the mechanisms behind various drug-induced corneal epithelial changes and recommendations for treatment have been evaluated in recent systematic reviews.6,7
Corneal deposits are a well-described side effect of amiodarone, which is theorized to be due to secretion of the drug in the lacrimal gland with uptake by the cornea. 19 Past literature has observed bilateral vortex keratopathy with brown to golden deposits.6,7 Notably, Mäntyjärvi et al. reported that these deposits do not significantly impair visual acuity, suggesting that treatment discontinuation may not be warranted based on this factor. 20 In fact, corneal deposits have been described as the most common and well-known ocular adverse effect of amiodarone, although other effects include lens opacities and optic neuropathy. 20
While prednisolone, among other immunosuppressive medications, exhibits anti-inflammatory and other systemic effects, prednisolone is known to induce apoptosis in the corneal epithelium. 21 Furthermore, in a study utilizing albino rabbits, Phillips et al. observed a significant suppression of stromal neovascularization by prednisolone, accompanied by reduced wound tensile strength and decreased collagen formation. 22 The precise mechanism linking these observations to corneal opacities remains unclear, necessitating further studies to unravel the underlying processes involved. However, there have been reports of steroid phosphates such as prednisolone being associated with stromal corneal calcifications; other researchers have posited that this corneal change may be secondary to an alteration of glycosaminoglycan metabolism of stromal keratocytes in the calcification process induced by topical steroid-phosphate medication. 23 Notably, our study did not yield a positive signal for prednisone or nonphosphate steroids, which aligns with prior literature.
Several glaucoma medications were also found to have positive signals for deposits, with the most common in this study being timolol, brimonidine, and latanoprost. Timolol has not been as commonly recognized for a potential association with corneal deposits in clinical practice, although there have been several plausible mechanisms reported. For instance, Nork et al. reported decreased corneal wound healing in both rabbits and monkeys following the administration of timolol. 24 Furthermore, in a randomized controlled trial, Grüb et al. reported an increased corneal thickness of 20 mm (P = 0.0659) following the application of timolol. 25 Another randomized controlled trial in 2013 by Grüb observed reversible increases in central corneal thickness. 26 Timolol appears to have an influence on the cornea as seen through these studies, although ascertaining a plausible mechanism for the development of corneal deposits necessitates further investigation. Furthermore, while changes have been observed in animal models, and while our finding of timolol-associated corneal deposits is new, timolol has been demonstrated to effect an anesthetic-like effect associated with superficial punctate keratitis. 27 Brimonidine, an effective glaucoma medication, also showed a positive signal for corneal deposits. In a prospective, randomized study of 20 patients, brimonidine induced a reversible increase in corneal thickness, but this finding’s clinical significance is yet to be determined. 28
Case reports of latanoprost-associated corneal toxicity 29 and netarsudil-induced corneal toxicity 15 also exist. Interestingly, this study identified a positive signal for cyclopentolate, although literature on cyclopentolate-associated corneal toxicity is scarce, and further investigation is needed to ascertain if this is a real signal. Anti-vascular endothelial growth factor agents such as aflibercept and brolucizumab have been found to influence the morphology of the cornea, although reports of deposits remain rare. 30 It is salient to note that ocular medications are used in aged patients who typically have ocular pathology. For example, in the case of cyclopentolate, which can be used to treat uveitis, it may be possible that the deposits observed in these reports are secondary to underlying disease such as uveitis rather than directly from medication.
Our study also found a significant signal for netarsudil. Netarsudil, recently approved in the United States in December 2017, has also been associated with vortex keratopathy/cornea verticillata and corneal epithelial edema due to its pharmacological effects on the trabecular meshwork and corneal endothelium.7,31–33 Corneal verticillata is a benign and reversible deposition of lipids or metabolic by-products within the corneal epithelium, leading to a vortex-like pattern visible under slit-lamp examination. These changes do not typically affect visual acuity and often resolve upon discontinuation of netarsudil. 7 Additionally, netarsudil may induce mild corneal edema in some cases, likely related to its influence on endothelial pump function and production of guttata-like abnormalities of the corneal endothelium. 15 Netarsudil only generated six reports on our analysis for corneal deposits, although for more specific terms such as “corneal edema,” it yielded 84 reports and statistical significance. While generally well-tolerated, these corneal changes underscore the need for regular monitoring in patients using netarsudil, especially those with preexisting corneal conditions.
Fluoroquinolones have been extensively documented to exhibit an association with corneal deposits. 6 Fluoroquinolones are known to be involved in the formation of white crystalline deposits, seen most often in ciprofloxacin. 18 The low solubility of ciprofloxacin at the physiological pH of the tear film enables corneal deposits to form. 34 In contrast to ciprofloxacin, ofloxacin exhibits the ability to penetrate the corneal barrier more effectively due to its higher solubility at the pH of the tear film. McDermott et al. found that ofloxacin at a dose of 30 µg/mL for 3 h did not induce adverse structural changes in the cornea. 35
Otherwise, clinical trials have documented that cenegermin is safe and effective in restoring corneal integrity, showing higher rates of healing when compared with treatment using the vehicle. 36 As early as 2022, a case report documented the first association between precipitate deposition on the ocular surface and cenegermin intake, and while this somewhat aligns with FAERS, further clinical investigations are warranted. 37
In our study, we expectedly found that the age-group with the most reports of corneal deposits was the elderly (65 years or older), although more than a third of reports had a missing age. Many of the patients who take the medications that yielded positive signals are elderly. However, Hashemi et al. substantiate the concept that advancing age is linked to a higher incidence of corneal pathology, emphasizing that the age-group of 80 years or older exhibits a greater prevalence compared with the 60–64 years age-group. 38 The role of sex in contributing to corneal deposits is less obvious: past studies have reported divergent findings, with some indicating a higher prevalence of corneal opacity in men, 38 whereas others have observed a higher prevalence in women. 39 Our findings were fairly unremarkable with approximately 40% of reports each from men and women, although 17% of reports were of an unknown gender.
In this study, FAERS offers strengths with its vast database of spontaneous reports from real-world clinical settings spanning 18 years. This retrospective approach provides a unique advantage by yielding findings over an extended duration, which can help identify rare or long-term adverse events not apparent in clinical trials. FAERS enables monitoring and detection of safety concerns related to medications and medical products, making it a valuable tool for generating hypotheses for subsequent clinical investigations.
However, there are limitations to consider. FAERS primarily collects spontaneous reports, which may result in gaps in coverage for all adverse events. This reliance on voluntary submissions could lead to underreporting, particularly among marginalized populations or those with limited understanding of the adverse event reporting process. FAERS also does not contain detailed, codified data on visual outcomes, and it may be possible that while some medications with positive signals in this report may cause corneal deposits, these deposits may not be clinically or visually significant. Additionally, the presence of comorbidities and concurrent use of multiple drugs among patients with corneal deposits may confound and weaken the associations observed in FAERS analysis. Genetic and environmental factors should also be considered in understanding this association. Clinical trials are essential to identify specific patient profiles susceptible to experiencing corneal deposits, but the follow-up period may not be adequate if the corneal deposit takes many years or decades to manifest. Another limitation common to adverse event analyses is that while we have data on event reports, we do not have data in terms of how many patients are taking these medications on a daily basis. Regardless, disproportionality analysis attempts to correct for these confounding factors. The quality of FAERS analysis relies on the quality of reported data, emphasizing the need for a more systematic approach to reporting adverse events associated with medications to draw stronger and more reliable conclusions, thereby enhancing pharmacovigilance and patient safety. Despite these limitations, FAERS can serve as a valuable tool for hypothesis generation and to identify potentially fruitful avenues of future study.
Conclusion
In conclusion, we identified positive safety signals for several medications linked to corneal deposits, inclusive of both well-known medications such as amiodarone and chloramphenicol and lesser-studied medications such as prednisolone and timolol. It is important to raise clinician awareness of these medications while pursuing future studies to further assess these corneal deposits.
IRB Approval
Ethical review and approval were waived for this study due to deidentified data. This study is exempted by the Rutgers New Jersey Medical School Institutional Review Board.
Footnotes
Authors’ Contributions
O.A.: Conceptualization, data curation, visualization, writing—original draft preparation, and writing—review and editing. H.K.: Methodology, investigation, software, and writing—review and editing. B.A.: Formal analysis and writing—review and editing. W.H.: Writing—review and editing, supervision, and validation. Y.D.: Supervision and validation.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
The authors did not receive any funding or support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.