
Abstract
Purpose:
To evaluate and compare the effects of subconjunctival injection of coenzyme Q10 (CoQ10) and vitamin E (Vit E) ophthalmic solution (Coqun®) with subconjunctival bevacizumab in a suture-induced corneal neovascularization (CoNV) rabbit model.
Materials and Methods:
CoNV was induced in the right eyes of 24 New Zealand rabbits using a 7.0 silk suture. One week after suturing, the rabbits were randomly divided into four groups and treated with a subconjunctival injection of either 0.1 mL balanced salt solution (control), bevacizumab (2.5 mg/0.1 mL), or two different doses of Coqun [(2 mg CoQ10 + 10 mg Vit E/0.2 mL) and (4 mg CoQ10 + 20 mg Vit E/0.4 mL)]. Photographs were taken on day 7 (pre-injection) and day 14 (7 days post-injection). On day 14, the regression area of CoNV was measured for analysis, and enucleation was performed for histopathological evaluation.
Results:
The CoNV areas after treatment were smaller in all three treatment groups compared with the control group (p < 0.01). The mean percentage of CoNV regression was highest in the bevacizumab group (87.8% ± 3.2%), followed by the Coqun groups (69.5% ± 5.9% in the 0.2 mL dose, and 67.1% ± 9.3% in the 0.4 mL dose) No significant difference was observed between the two different doses of Coqun (p = 0.99).
Conclusions:
Subconjunctival administration of Coqun ophthalmic solution may offer a beneficial adjunct for the treatment of CoNV. Although it is not less effective than bevacizumab, its neuroprotective properties suggest potential value in cases where CoNV and glaucoma coexist. Further clinical studies are warranted to confirm these findings and to better define its therapeutic role.
Introduction
A healthy cornea is avascular and transparent, ensuring proper vision. 1 Corneal neovascularization (CoNV), a major public health concern, affects approximately 1.4 million people annually, often resulting from infections, injuries, inflammatory diseases, prolonged contact lens use, or corneal transplantation. 2
Different surgical and medical strategies have been used for the treatment of CoNV. Some of the applied treatment methods are amniotic membrane transplantation, topical steroids, nonsteroidal anti-inflammatory drugs, laser photocoagulation of feeding vessels, photodynamic therapy, fine-needle diathermy, and antivascular endothelial growth factor (VEGF) antibodies (bevacizumab, ranibizumab, aflibercept). 3 The beneficial effect of these therapies was shown in numerous studies.4,5
Coqun® (Visufarma SpA, Roma) is a sterile, preservative-free solution containing 100 mg coenzyme Q10 (CoQ10) and 500 mg vitamin E (a tocopheryl polyethylene glycol 1000 succinate) (Vit E). Coqun shows antioxidant effects by increasing energy production and protecting retinal ganglion cells, whereby they are used as an add-on treatment with antihypertensive glaucoma medications. 6 CoQ10 found in tissues with high energy requirements is a key factor for energy production in the mitochondria.7,8 It has antiapoptotic, anti-inflammatory, and antioxidant effects, which include inhibition of lipid peroxidation and free radical damage. 9 In the literature, CoQ10 has shown substantial benefits on rapid nerve regeneration and ocular surface stability. 10 Vit E provides antioxidant effects via stabilization of cell membranes, regulation of signaling factors, and inhibition of protein kinase C activation.11,12 It can also inhibit nuclear factor (NF-κB) activation, which is a eukaryotic transcription factor activated by oxidative stress. 13
There is no data in the literature whether Coqun is pro-angiogenic (regarding its antiapoptotic properties) or antiangiogenic (regarding its anti-inflammatory properties) on the cornea. The object of the study to determine the effect of subconjunctival injection of Coqun on the suture-induced CoNV in the rabbit eyes.
Materials and Methods
This experimental animal study, approved by the Gazi University Ethics Committee (Project number G.Ü.ET-18.058), enrolled 24 healthy male New Zealand rabbits. We adhered to the Animal Research: Reporting of In Vivo Experiments and the Association for Research in Vision and Ophthalmology guidelines throughout our research process. All rabbits were individually housed in cages at controlled humidity and room temperature.
CoNV was induced using a modified suture model described by Williams in 1985.
14
Under general (intramuscular 50 mg/kg ketamine and 5 mg/kg xylazine) and topical anesthesia (proparacaine HCl 0.5%; Alcaine, Alcon Pharmaceuticals Ltd., Fort Worth, Texas), a 7.0 silk suture (3 mm width) was placed in the corneal stroma, 1–1.5 mm away from the superior limbus, using an operating microscope. To prevent infection, moxifloxacin eye drops (Vigamox; Alcon, Texas) were administered twice daily for 1 week. All sutures were placed by the same surgeon (M.C.O.). After 7 days, under general anesthesia, all sutures were removed. The rabbits were then randomly assigned to one of four treatment groups:
Group 1 (Control): Received a subconjunctival injection of 0.1 mL balanced salt solution (n = 6). Group 2 (Bevacizumab): Received a subconjunctival injection of 0.1 mL bevacizumab (Avastin®, Roche Pharmaceuticals, Switzerland) (2.5 mg) (n = 6). Group 3 (0.2 mL-dose Coqun) Received a subconjunctival injection of 0.2 mL Coqun (2 mg CoQ10 + 10 mg Vit E, Coqun®, Visufarma SpA, Roma) (n = 6). Group 4 (0.4 mL-dose Coqun) Received a subconjunctival injection of 0.4 mL Coqun (4 mg CoQ10 + 20 mg Vit E) (n = 6).
Photographs of the CoNV area were taken using an operating microscope with 16× magnification (Möller-Wedel FS 3000, Haag Streit) on day 7 (before injections) and day 14 (7 days after injections). The area of CoNV was measured in square millimeters using ImageJ software (Version 1.52i, USA). Calibration was performed by taking a photograph of a ruler under the same magnification and setting a 1-mm reference line within the software to ensure standardized measurements. The neovascular region, extending from the limbus to the suture line, was manually outlined on the screen by two examiners (A.O. and M.C.O.) (Fig. 1). The initial CoNV area (on day 7) was set as 100%, and the percentage regression after treatment was calculated using the formula: CoNV area 7th day-CoNV area 14th day)/CoNV area 7. Day ×100. The Intraclass Correlation Coefficient between the two examiners was 0.98 (95% confidence interval: 0.957–0.993, p < 0.05), indicating excellent interobserver reliability. After euthanasia and enucleation, corneal samples from the neovascularized areas, including the limbus, were excised and fixed in 10% formalin for 24 h. The samples were then embedded in paraffin, sectioned at 4 μm thickness, and stained with hematoxylin and eosin for histopathological analysis.
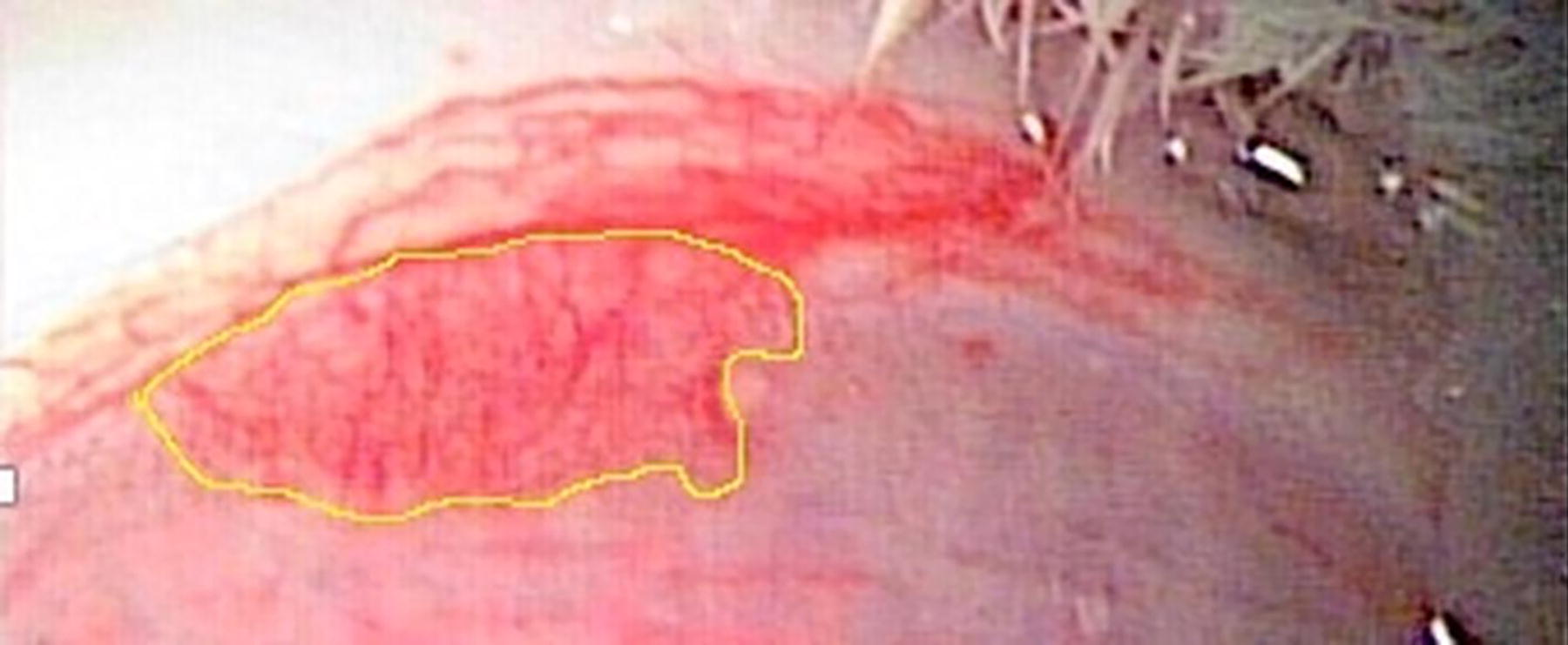
Surrounded neovascular region from limbus to suture line with mouse.
The data were presented as means ± standard deviation for symmetrically distributed variables. Group comparisons were performed using the Kruskal–Wallis one-way analysis of variance test. Post hoc analysis was conducted to determine significant differences between groups. A p value of <0.05 was considered statistically significant. SPSS software (Version 20.0.0, IBM Corp.) was used for statistical analysis.
Results
Following suture removal, the mean CoNV areas were measured as follows: Group 1 (Control): 2.62 ± 0.39 mm2, Group 2 (Bevacizumab): 2.59 ± 0.33 mm2, Group 3 (Low-dose Coqun): 2.82 ± 0.41 mm2, and Group 4 (High-dose Coqun): 2.61 ± 0.27 mm2. There was no significant difference in baseline CoNV areas among the four groups (p = 0.7) (Table 1). After 1 week of treatment (day 14), the mean CoNV areas were: Group 1: 1.86 ± 0.19 mm2, Group 2: 0.31 ± 0.04 mm2, Group 3: 0.86 ± 0.19 mm2, and Group 4: 0.85 ± 0.20 mm2. The mean percentage regression of CoNV areas was:
The Mean Corneal Neovascularization Areas at the Seventh (Pre-Injections) and Fourteenth (7 Days After Injections) and the Mean Percentages of Regression Areas of CoNV
Post hoc analysis showed that coenzyme Q10/Vitamin E and bevacizumab treatments were significantly associated with regression areas than those with control group (P < 0.001 for all). Also, significant regression of treatment areas was observed in the bevacizumab group when compared with coenzyme Q10/Vitamin E groups.
CoNV, Corneal neovascularization; Group 1: control; Group 2: 0.1 mL Bevacizumab; Group 3: 0.2 mL coenzyme Q10/vitamin E; Group 4: 0.4 mL coenzyme Q10/Vitamin E.
Group 1: 28.7% ± 3.8 (p < 0.01) (Fig. 2A, B)
Group 2: 87.8% ± 3.2 (p < 0.01) (Fig. 2C, D)
Group 3: 69.5% ± 5.9 (p < 0.01) (Fig. 2E, F)
Group 4: 67.1% ± 9.3 (p < 0.01) (Fig. 2G, H)
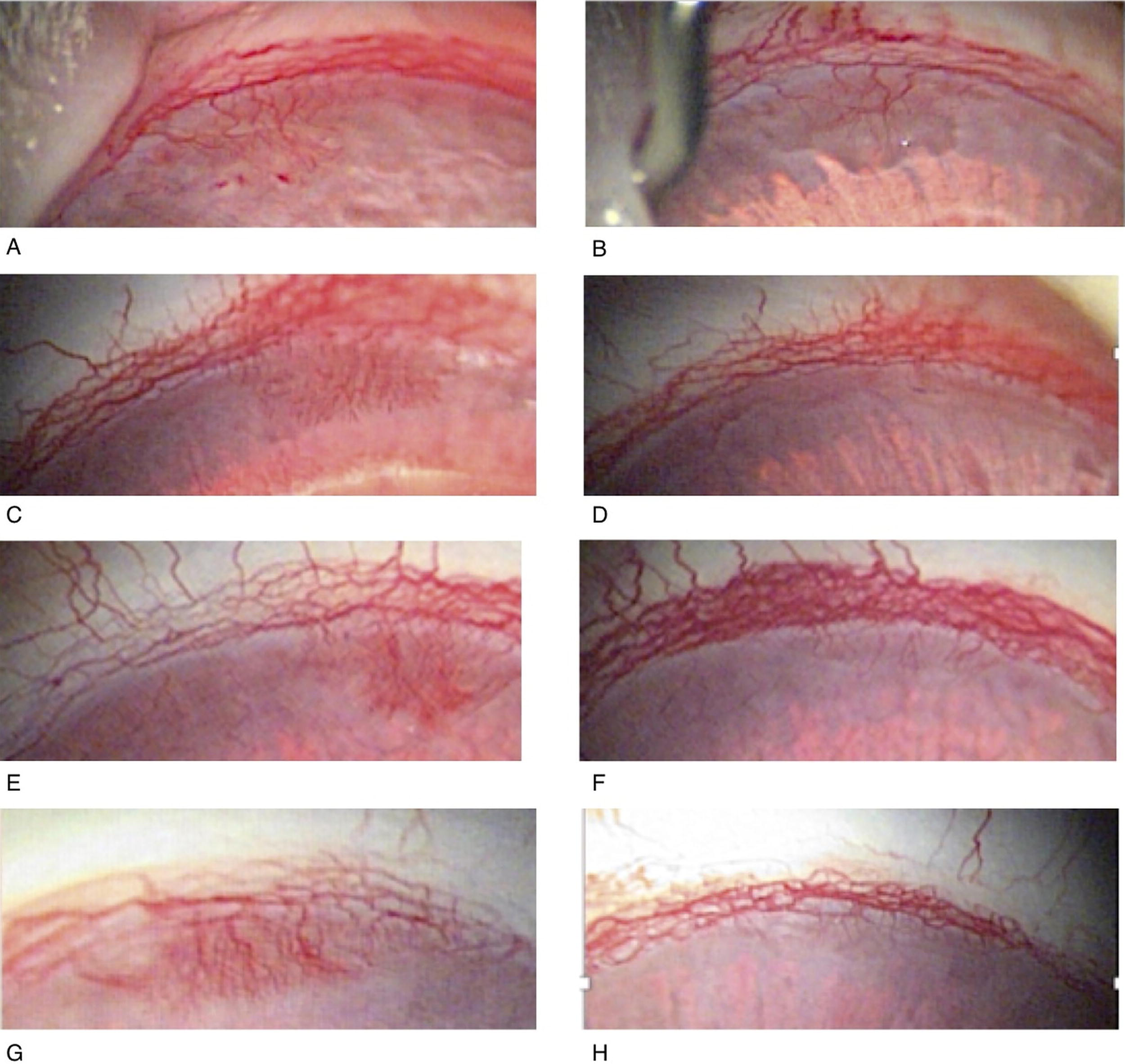
Photographs of corneal neovascularization regions on the 7th day (pre-injections) [control
The CoNV regression was significantly greater in all three treatment groups (Groups 2–4) compared with the control group (p < 0.01). There was no statistically significant difference between low-dose (Group 3) and high-dose (Group 4) Coqun (p = 0.99) (Fig. 3). However, regression in the bevacizumab group (Group 2) was significantly higher than in the Coqun groups (Groups 3 and 4) (p < 0.05). Histopathological analysis with hematoxylin-eosin staining revealed numerous neovascular vessels in the control group (Fig. 4A). In contrast, no detectable vessels were observed in the bevacizumab group (Group 2) (Fig. 4B), while fewer vessels were seen in the Coqun groups (Groups 3 and 4) (Fig. 4C, D).
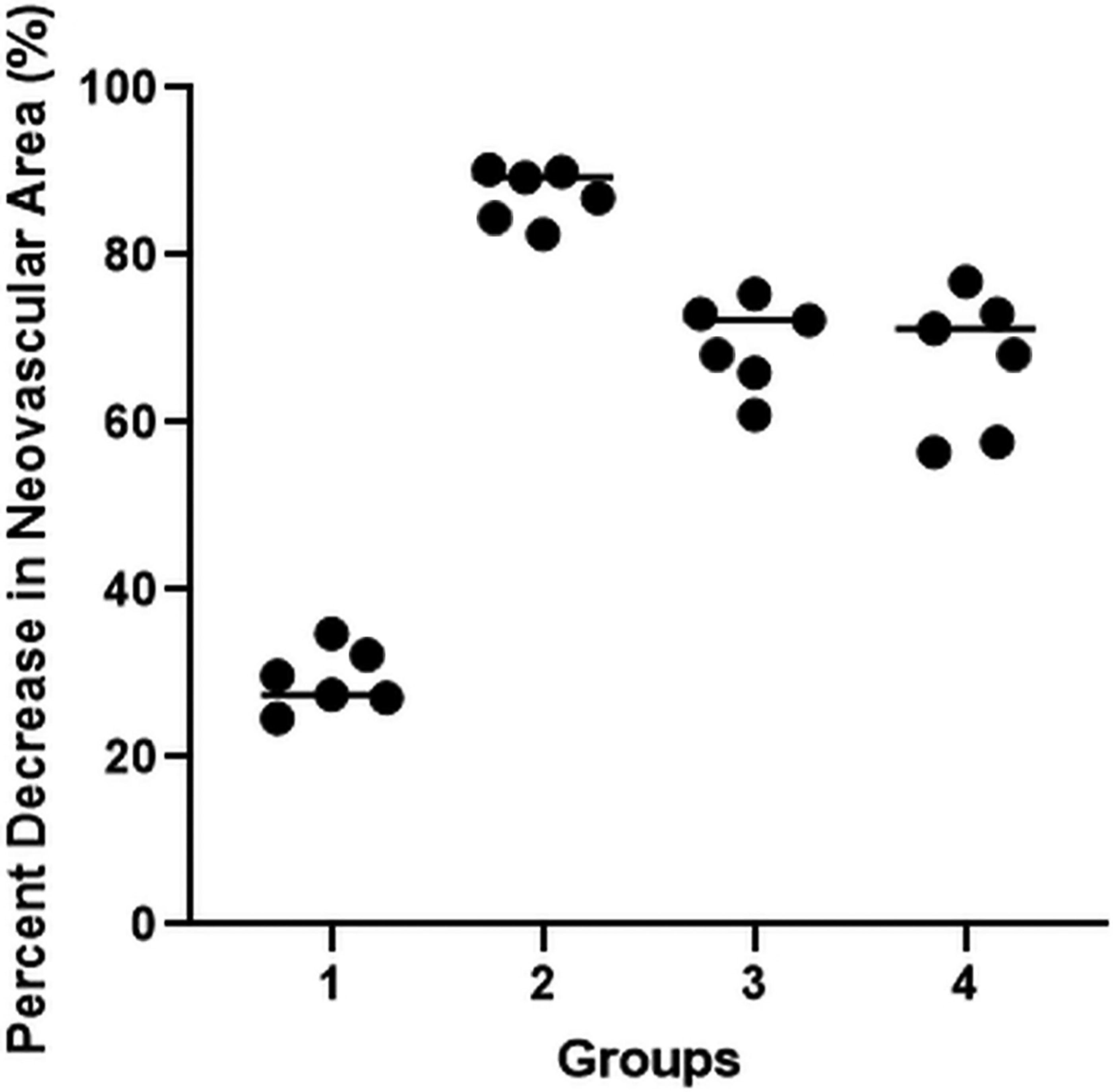
Percent decrease in neovascular area (%) in group 1, group 2, group 3, and group 4.

Hematoxylin and eosin staining of the corneal regions: control,
Discussion
Various treatment strategies have been explored for CoNV, but an optimal regimen remains controversial. The goal is to prevent new vessel formation and promote regression of existing vessels. 15 Although many experimental and clinical studies have shown the effectiveness of bevacizumab in treating CoNV, bevacizumab alone may not be sufficient for complete regression. 16 Incomplete regression of CoNV with bevacizumab may be due to the involvement of multiple pro-angiogenic and/or pro-inflammatory factors beyond VEGF, including tumor necrosis factor-alpha, fibroblast growth factors (FGF-1 and FGF-2), angiostatin, endostatin, thrombospondin, matrix metalloproteinases, insulin-like growth factor, and platelet-derived growth factor.17,18 Corticosteroids and NSAIDs are commonly used due to their anti-inflammatory and antiangiogenic effects; however, long-term use carries the risk of corneal complications and glaucoma.19–22 For these reasons, research has focused on new treatment strategies with fewer side effects.23–26
CoQ10, known for its neuroprotective effects in glaucoma, is commercially available for ophthalmic use only in combination with Vit E. 27 Studies by Behndig et al. demonstrated that CoQ10 protects the cornea from oxidative damage following refractive surgery.28,29 Brancato et al. further reported that CoQ10 reduces corneal keratocyte apoptosis more effectively than other antioxidants after excimer laser surgery.30,31 Additional studies have shown that CoQ10 mitigates corneal damage from UVB exposure and protects against keratocyte apoptosis induced by ethanol.9,32 The combined effects of CoQ10 and Vit E enhance mitochondrial bioenergetic function, inhibit glutamate excitotoxicity, and reduce oxidative stress.33,34 However, their role in ocular angiogenesis has not been widely studied. Research in oncology models suggests that CoQ10 inhibits angiogenesis by suppressing MMP-9/ICAM-1/NF-κB activation and upregulating antioxidant gene expression.35–37 Given that ERK pathway activation is a key driver of angiogenesis, CoQ10’s modulation of this pathway may explain its antiangiogenic effect.38–40 On the other hand, A study on an experimental retina model has shown that CoQ10 supplementation reduces VEGF expression and neovascularization. 41
Vit E, a lipid-soluble antioxidant, protects cell membranes from lipid peroxidation and exerts have additional nonantioxidant effects, including inhibition of protein kinase C and activation of phosphoprotein phosphatase 2A. 42 It may also inhibit NF-κB, a transcription factor critical for inflammation, cell proliferation, and angiogenesis. 43 Although the exact mechanisms remain unclear, Vit E appears to reduce angiogenesis through both antioxidant and nonantioxidant pathways. 12
Coqun, has shown potential for ocular protection with no corneal side effects, making it a promising candidate for CoNV treatment. 27 The Coqun likely exerts its antiangiogenic effect through the indirect modulation of oxidative stress and inflammatory pathways. Both bevacizumab and Coqun (available in 2 mg/10 mg and 4 mg/20 mg doses) significantly diminished CoNV in comparison to the control group, yet bevacizumab revealed a regression that was approximately 20% greater than that of Coqun. This suggests that bevacizumab targets angiogenesis more effectively than Coqun, likely due to its direct VEGF inhibition. The association of glaucoma and CoNV after penetrating keratoplasty is not uncommon. Although not as potent as direct VEGF inhibition, the Coqun combination may be useful in the treatment of CoNV with concurrent seconder glaucoma thereby offering a dual therapeutic value: downregulating angiogenesis and supporting neuroprotection. 44
A key limitation of this study is that the individual effects of CoQ10 and Vit E were not assessed independently, as only the combined ophthalmic formulation was available for ocular use. This limits our ability to distinguish the specific contribution of each component to the observed antiangiogenic effects. CoQ10 and Vit E are lipid-soluble antioxidants that work synergistically to protect cells from oxidative damage. When Vit E neutralizes free radicals, it becomes oxidized. CoQ10 can regenerate oxidized Vit E, restoring its antioxidant function. This redox cycling enhances the overall antioxidant capacity of the cell.35–37 Other limitation is that no statistically significant difference was observed between the two dosing levels of the Coqun, possibly due to a plateau effect where tissue response no longer increases with higher doses. Moreover, as the study was conducted in a rabbit model, differences in pharmacokinetics and pharmacodynamics compared to humans may limit direct translation.45,46 Further clinical research is needed to determine optimal dosing and assess dose-response relationships in human subjects.
Histopathological analysis supported our findings, showing a high density of neovascular vessels in the control group, no vessels in the bevacizumab group, and fewer vessels in the Coqun groups. However, statistical analysis of histological results was not feasible due to variability in vessel counts across sections. No ocular complications, such as corneal edema or epithelial defects, were observed.
Conclusions
Our study is the first to demonstrate that subconjunctival injection of Coqun reduces CoNV in an experimental model. This combination may provide clinical benefit in cases where CoNV and glaucoma occur together. Further long-term, prospective, and comparative clinical studies are necessary to determine the optimal dosage, treatment duration, and potential combination.
Footnotes
Authors’ Contributions
A.Ö.: Conceptualization, methodology, investigation, writing—original draft, data curation, and formal analysis. M.C.Ö.: Supervision, conceptualization, methodology, validation, review, and editing. D.Y.Y.: Writing—review and editing. M.A.İ.: Histopathological analysis and data curation. All authors have made substantial contributions to the conception, design, execution, analysis, and interpretation of this study. Each author has approved the final article and agrees to be accountable for all aspects of the work, ensuring its integrity and accuracy. The authors confirm that the article is original, has not been published before, and is not currently under consideration for publication elsewhere.
Author Disclosure Statement
None of the authors of this article has a financial or personal relationship with other people or organizations that could inappropriately influence or bias the content of the article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.