
Abstract
Abstract
Objective:
The primary goal of the study was to assess the efficacy of mindfulness-based meditation therapy on anxiety, depression, and spiritual well-being of Japanese patients undergoing anticancer treatment. A secondary goal was to assess the relationships among anxiety, depression, spiritual well-being, growth, appreciation, pain, and symptoms.
Methods:
The subjects were 28 patients who were receiving anticancer treatment. The subjects participated in two sessions of mindfulness-based meditation therapy, including breathing, yoga movement and meditation. Each patient was taught the program in the first session, then exercised at home with a CD, and subsequently met the interviewer in a second session after 2 weeks. Primary physicians recruited the patients and interviews were conducted individually by nurses or psychologists with training in the program. Patients completed preintervention and postintervention questionnaires on anxiety and depression (Hospital Anxiety and Depression Scale [HADS]), spiritual well-being (Functional Assessment of Chronic Illness Therapy-Spiritual [FACIT-Sp]), and appreciation, growth, pain, and symptoms.
Results:
HADS scores significantly decreased from 12 ± 5.3 to 8.6 ± 6.3 (p = 0.004) after the intervention, and FACIT-Sp increased from 32 ± 6.5 to 33 ± 6.9 (p = 0.69), but the change was not significant. There were significant associations between FACIT-Sp and HADS (r = −0.78, p = 000), FACIT-Sp and growth (r = −0.35, p = 0.04), FACIT-Sp and pain (r = −0.41, p = 0.02), and growth and appreciation (r = 0.45, p = 0.009).
Conclusions:
Mindfulness-based meditation therapy may be effective for anxiety and depression in Japanese cancer patients, and spiritual well-being is related to anxiety and depression, growth, and pain. The negative correlation of spirituality with growth differs from the results of previous studies and the mechanism of this effect needs to be investigated further.
Introduction
A mindfulness approach is an effective intervention from a psychological perspective. The Mindfulness-Based Stress Reduction (MBSR) program was modeled on the work of Kabat-Zinn and colleagues 6 at the Center for Mindfulness-Massachusetts Medical Center. The program is based on the principal of mindfulness, defined as moment-to-moment, present-centered, purposive nonjudgmental awareness. The goal of the MBSR program is to guide participants to achieve greater awareness of themselves, their thoughts, and their bodies through class discussion, meditation, and yoga exercises. For patients with cancer, Speca et al. 7 showed effects of the MBSR on mood disturbance using the Profile of Mood Scale (POMS) and stress symptoms using the Symptoms of Stress Intervention (SOSI), and Carson et al. 8 showed an effect on quality of life based on the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) and the immune profile. Monti et al. 9 showed that Mindfulness-Based Art-Therapy (MBAT), which includes mindfulness and art therapy, also produces a significant decrease in symptoms of distress and improvements in key aspects of health-related quality of life using the Short-Form Health Survey (SF-36). Garland et al. 10 examined the effects on spirituality, stress symptoms, and mood of a Healing Art (HA) program compared with MBSR PTG. Improved growth, a relationship of PTG in MBSR with spirituality, and increases in spirituality with related decreases in stress and mood disturbance were found in participants in both groups.
Many studies from Western countries have shown the efficacy of MBSR on mood or symptoms, but few have been performed for Japanese patients. Therefore, it is unclear if MBSR is effective for moods such as anxiety or depression in Japanese cancer patients. Moreover, very few studies have investigated the effects of a mindfulness program on growth or spirituality. Thus, we investigated the efficacy of mindfulness on anxiety, depression, and spirituality in Japanese patients with cancer, and determined the associations among anxiety, depression, spiritual well-being, growth, and appreciation, in addition to physical symptoms.
Patients and Methods
Participants
The participants were outpatients who were receiving anticancer chemotherapy, radiation, or medication at a general hospital in Western Japan. The additional inclusion criteria were no cognitive impairment and age greater than 20 years old. Patients were excluded if they were experiencing severe pain or physical symptoms. These were rated using a numeric rating scale (0–10 points), and those with a score of above 8 were excluded from the study. A total of 28 patients (4 males, 24 females) with a mean age of 60.0 ± 9.2 years old participated in the study. The primary tumor sites were the breast (n = 21), colon (n = 2), stomach (n = 2), and bladder (n = 2). The performance status ranged from 0 to 2 and all patients were able to visit the hospital.
Outcome measures
The Japanese version of the Hospital Anxiety and Depression Scale (HADS)11,12 was used to measure levels of anxiety and depression. The HADS score ranges from 0 to 42. Following the model of our group, we chose the sense of meaning measured by the FACIT-Sp scale 13 as the primary end point. The validity and reliability of the Japanese version of the FACIT-Sp is well established. 14 The FACIT-Sp consists of two domains, meaning of life and religious issues, but we only used the meaning of life domain, which includes 8 items and is scored on a 4-point scale (range, 0–4). The total range of the FACIT-Sp is 0 to 32 and high scores indicate an elevated sense of meaning of life or a peaceful state of mind.
To measure psychological appreciation, we used several items from the Caregiving Consequence Inventory. 15 This is a 12-item questionnaire with 4 core domains, of which we used “appreciation” only. Appreciation is determined from 2 items: “Having this disease made me more grateful for my family” and “Having this disease made me more grateful for other people.” To measure psychological growth, we used 3 items from the Benefit Finding Scale 16 : “Having had cancer has made me more sensitive to family issues,” “Having had cancer made me a more responsible person,” and “Having had cancer has helped me to budget my time better,” using a 7-point numeric rating scale. The α reliability coefficient of the 3 items was 0.71 in this sample. A high score indicates an elevated sense of life completion (range, 1–7). We also monitored the intensity of pain and physical symptoms such as constipation, nausea, fatigue, and sleep disturbance on a 10-point numeric rating scale (0–11).
Interventions and procedure
We used a modified version of the MBSR program,6,17 in which we refer to cyclic meditation as that including both breathing and meditation. During meditation, patients move their hands or legs to focus their attention (Fig. 1). The cyclic meditation program takes about 30 to 60 minutes per session and is conducted by nurses or a clinical psychologist who received training for at least 3 hours. The training included basic communication skills and yoga skills learned directly from a yoga specialist or using a CD or DVD. A primary physician recruited the patients and a clerk obtained informed consent and asked the patients to complete questionnaires preintervention and postintervention. In the pretherapy session, the patient learned the cyclic meditation program and it was recommended that they perform the therapy at home once per day. After 2 weeks, the patients met the interviewers in a second session to talk about their impressions.
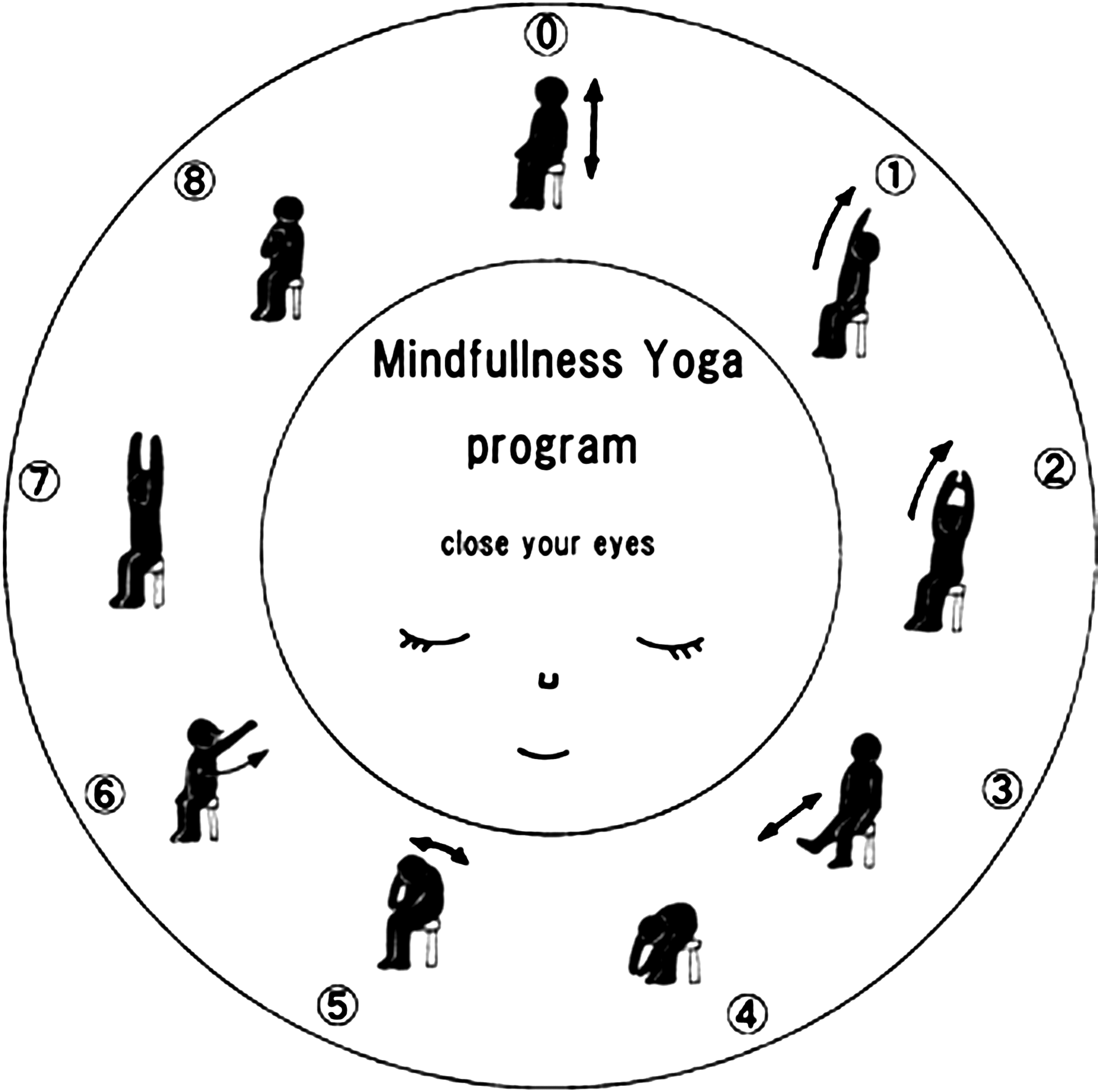
The cyclic meditation program.
Statistical analysis
A p value less than 0.05 was taken to indicate a significant level in all statistical analyses. All reported p values are two-tailed. The statistical procedures were conducted with SPSS 15.0 (Japanese version) for Windows (SPSS Inc., Chicago, IL, 2006). To evaluate the efficacy of mindfulness therapy on anxiety, depression and spirituality, a Wilcoxon sign rank test was conducted on the HADS and FACIT-Sp scores.
Results
Table 1 shows the scores for questionnaires pre- and post-intervention. Anxiety score of the HADS significantly decreased from 6.9 ± 3.6 to 5.1 ± 3.9 (p = 0.01) and Depression score of the HADS also significantly decreased from 5.1 ± 2.9 to 3.5 ± 3.1 (p = 0.009). Total HADS scores significantly decreased from 12 ± 5.3 to 8.6 ± 6.3 (p = 0.004) after the intervention, and FACIT-Sp scores increased from 32 ± 6.5 to 33 ± 6.9 (p = 0.69, not significant). Table 2 shows the results of correlation analyses. There were significant relationships between FACIT-Sp and HADS (r = −0.78, p = 000), FACIT-Sp and growth (r = −0.35, p = 0.04), FACIT-Sp and pain (r =−0.41, p = 0.02), and growth and appreciation (r = 0.45, p = 0.009).
FACIT = SP, Functional Assessment of Chronic Illness Therapy-Spiritual; HADS, Hospital Anxiety and Depression Scale.
p < 0.00.
p < 0.05.
p < 0.01.
HADS, Hospital Anxiety and Depression Scale; FACIT = Sp, Functional Assessment of Chronic Illness Therapy = Spiritual.
Discussion
The decrease in the HADS scores after the intervention shows that mindfulness-based cyclic meditation affects anxiety and depression for Japanese cancer patients. This result is consistent with those of Tacon et al.18,19 using the State-Trait Anxiety inventory and Garland et al. 10 using the Profile of Mood of States. Therefore, MBSR may be effective for anxiety or depression in Japanese patients as an individual and short-term therapy. Matchim and Armer 20 suggested that more research is needed to test the instruments in MBSR and establish their validity and reliability in oncology patients. Thus, the present study provides a new finding that MBSR may affect anxiety and depression in Japanese patients based on the HADS score. The increase in FACIT-Sp scores after MBSR was not significant, with a change from 32.1 to 33.0 compared to the increase in FACIT-Sp score in Garland et al. 10 from 28.43 to 32.1. These results suggest that ceiling effects may prevent a significant change in spiritual well-being.
Regarding the association among variables, the relationship of FACIT-Sp with HADS (r = −0.78) shows that spirituality is correlated with anxiety and depression. This result is also in accord with Garland et al., 10 in which increased spirituality was related to decreased stress and reduced mood disturbance after MBSR. FACIT-Sp and growth showed a significant negative association, which is opposite to the results of Garland et al., 10 in which a benefit finding was elicited or posttrauma growth was related to spirituality. Our results suggest that patients with high spirituality such as meaning or moderate feelings do not always experience growth. This negative association may have been influenced by other variables such as pain, 5 and self-reporting or a daily diary may be useful to examine the process of psychological change.21,22
Last, we note several limitations of the study, including that a control group was not established and the number of participants was small. However, the results provide a useful indication that MBSR may be effective for anxiety and depression in Japanese cancer patients, and that spiritual well-being is related to anxiety, depression, and growth. A further study including a control group may help to establish these findings more clearly.
Footnotes
Acknowledgments
This research was supported by a Grant-in-Aid for Scientific Research (C).
Author Disclosure Statement
No competing financial interests exist.