
Abstract
Abstract
Purpose:
Florida was the first state to develop and implement a publicly funded pediatric palliative care program, which provides supportive care services to children and families from the point of diagnosis onward. Nurses employed by the Florida Department of Health, Children's Medical Services Network (CMSN) play an important role in this program as they are charged with identifying children with life-limiting illnesses in their caseloads for referral to the program. This study aims to estimate the differtences in referral preferences of nurses who work in Partners in Care: Together for Kids (PIC:TFK) program areas versus nurses who work in non-PIC:TFK areas.
Methods:
Mail and Web-based surveys were conducted with 279 nurses, 141 of whom work in a PIC:TFK site and 138 did not.
Results:
Results of the multivariate analyses suggest that few significant differences exist in the nurse's preferences to refer children to pediatric palliative care; however, there were significant differences in the preferred timing of referral. Nurses who work in an PIC:TFK area were 3.7 to 10.4 times as likely as nurses who do not work in a PIC:TFK area to refer children prior to the end of life.
Conclusion:
Our study provides evidence that nurses who have experience with a pediatric palliative care program are more likely to refer children to programs before the end of life. While our study results are encouraging, they also suggest that as the PIC:TFK program expands nurse training will be essential for equitable and appropriate referrals across a diverse set of illnesses.
Introduction
Traditionally, reimbursement policies for private and public health care organizations in the U.S. require a physician's authorization to refer a child to pediatric palliative care. Oftentimes however, nurses are the first to identify and suggest names of children to the physician for referral.13,14 Outside of the United States, nurses often have as much referral authority as physicians in pediatric palliative care programs. 15 Regardless of who is authorized to make referrals, nurses play a key role in the process. Therefore, it is important to understand nurses' perceptions on which children should be referred to pediatric palliative care.
Although there are a number of studies on nurses attitudes and knowledge of palliative care, as well as nurses' perceived barriers toward palliative care, there is little evidence on nursing referral preferences, and these studies are focused on adults.14,16,17 A 1998 study, which included but was not limited to nurses, retrospectively analyzed data from 108 referrals to a palliative consulting team. 18 Results showed that referred patients represented a variety of diseases including cancer, acquired immune deficiency syndrome (AIDS), as well as cardiac, renal, pulmonary, and neurologic diseases, and the majority (52%) had cancer. Another study surveyed 160 registered nurses and asked about their attitudes toward hospice referral. 19 Findings suggest that nurses resist referring patients to hospice care as long as they thought that home health care could provide adequate services. A more recent study investigated the role of nursing home staff members in referral and timing of referral to hospice care. 20
Qualitative findings show that staff looked for familiar signs of decline in the patient's health status when deciding to refer patients and some staff members felt that hospice did not add value to nursing home care or was only for patients in crisis. To our knowledge there have been no studies on nurses' perceptions of referral to pediatric palliative care for a variety of diseases.
Identifying children for referral is the first step to enrolling children in Florida's integrated pediatric palliative care program called Partners in Care: Together for Kids (PIC:TFK). Nurse care coordinators employed by the State's Title V program identify children for potential enrollment from their caseloads of children with special health care needs. These children are enrolled in Medicaid or the State Children's Health Insurance Program (SCHIP), which serves children up to age 21. A referral must then be granted from the children's primary care physicians. Because the state-employed nurses initiate the enrollment process, it is imperative that these nurses understand the basic tenets of pediatric palliative care and the PIC:TFK program. All nurse care coordinators who are employed in a PIC:TFK site are required to attend an on-site training session which is conducted by the PIC:TFK program director. The training describes the program's services and provides guidance on identifying and enrolling children. Once the primary care physician authorizes the referral, families are approached to voluntarily enroll in PIC:TFK and ultimately, hospices provide palliative care services including support counseling, expressive therapies, specialized nursing care, respite, and pain and symptom management. Although the state-employed nurse care coordinators do not provide the palliative care, they work with hospice staff to ensure that the children's needs are met.
A paucity of evidence exists on nurse referral preferences, yet nurses play an important role in the referral process. To address this gap in knowledge, this study has three aims. First, the study describes whether or not nurses believe children with 11 life-limiting diseases should be referred to pediatric palliative care. Second, for those nurses who indicate that they would refer a child with that disease, the study describes the factors that affect nurses' preferred timing of referral. Finally, the results are compared and contrasted for those state-employed nurses in Florida who did and did not work in an area in which the PIC:TFK program operates.
Methods
To estimate the factors that affect nurses' referral preferences, we used a cross sectional study design. In the fall of 2008, surveys were administered to all state-employed nurse care coordinators in Florida. The University of Florida's Institutional Review Board approved this study.
Study participants
There are 21 Children's Medical Services Network (CMSN) area offices located in Florida, where nurses are responsible for coordinating the care of children with special health care needs who are enrolled in Medicaid or the SCHIP. Regional nursing directors were asked to provide the number of nurses in their area office. There are 454 nurses across the state; 206 nurses employed at PIC:TFK sites and 248 nurses employed at non-PIC:TFK sites.
Surveys were mailed to each office, and nurses had the option of completing the survey online if preferred. A tracking code linked respondents to their respective area office; however, surveys were completely anonymous. Reminders were sent 2, 4, and 6 weeks after the first mailing. The overall survey response rate was 61%; the response rate for PIC:TFK sites was 68% and the response rate for non-PIC:TFK sites was 56%.
Measures
We utilized an 88-item survey that was developed by researchers at the University of Florida to capture referral preferences of primary care practitioners to pediatric palliative care. 21 Survey questions assessed whether or not nurses would refer children with specific diagnoses to palliative care services, and if so, when. Diagnoses included cancer, cystic fibrosis, human immunodeficiency virus (HIV), extreme prematurity, genetic diseases, metabolic diseases, sickle cell disease, cerebral palsy, brain injury, muscular dystrophies, and diabetes. For each of the diagnoses, the responses were: “does not need referral,” “needs referral at diagnosis,” “needs referral once the child and family have been living with the disease for a while, but the condition is stable,” “needs referral once the child's condition becomes unstable,” and “needs referral at the end of life, once curative treatment is no longer an option.” Respondents' age, gender, race/ethnicity, highest degree held, years in practice, past participation in a formal palliative care training course, and numbers of children on the nurse's current caseload were also recorded. Race/ethnicity categories were white non-Hispanic; black non-Hispanic; Hispanic; and other race, which may have been chosen by nurses of more than one racial category.
Two binary dependent variables were created to reflect the two primary outcomes of interests. First, respondents were assigned a value of one if they indicated the child should be referred to palliative care and a value of zero otherwise. If respondents indicated that referral was necessary, a second binary variable was created. Nurses who indicated that the child should be referred at diagnosis or mid stage of illness were assigned a value of one, and a value of zero was assigned to responses that palliative care was appropriate at the end of life. Predictor variables were included to control for demographics, highest degree earned, years in practice, current caseload, and completion of a formal palliative care training course in the past. Formal palliative care training courses could have included End-of-Life Nursing Education Consortium, Initiative for Pediatric Palliative Care, or a National Hospice and Palliative Care Organization course. A binary variable was included and equal to one if a nurse was employed in a PIC:TFK site, and zero otherwise. All analyses were conducted using SPSS version 16.0 (SPSS Inc., Chicago, IL).
Results
Sample characteristics
As shown in Table 1, the overwhelming majority of survey respondents are female (99.3%) and registered nurses (93.7%). Respondents are primarily white, non-Hispanic (81.0%), older than 50 (59.4%), and had more than 20 years' experience as a practicing nurse (64.1%). Demographic profiles of respondents at PIC:TFK sites versus non-PIC:TFK sites were similar, with the exception of caseload and highest degree earned. The mean number of children in a nurse's current caseload was significantly lower for PIC:TFK sites (166) than for non-PIC:TFK sites (196; p < 0.02).
PIC:TFK, Partners in Care: Together for Kids; SD, standard deviation.
Referral to palliative care
Figures 1 and 2 show that across all but one of the diseases, approximately 88% of nurses would refer a child to palliative care. Fewer nurses would refer children with diabetes in both the PIC:TFK (81.2%) and non-PIC:TFK (71.3%) sites. Cancer was the only disease for which 100% of nurses reported they would refer to palliative care. Results from paired t tests show that a significant difference in referral preferences existed between the PIC:TFK and non-PIC:TFK sites for sickle cell disease, whereas more nurses in the PIC:TFK sites would refer a child compared to nurses in the non-PIC:TFK sites (p < 0.01).
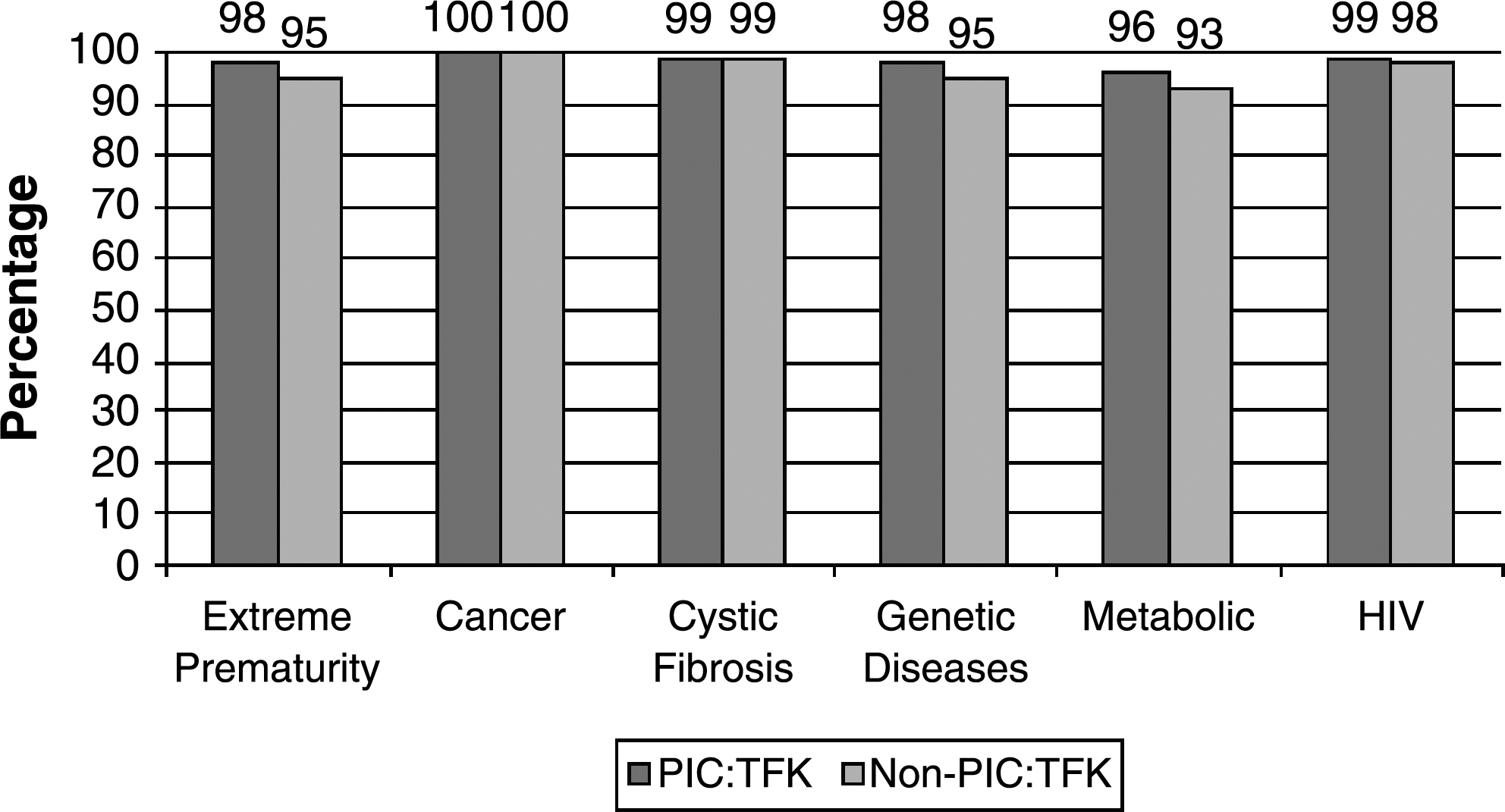
Percentage of nurses who would refer by disease.

Percentage of nurses who would refer by disease.
Timing of referral to palliative care
Figures 3 and 4show the preferred timing results. Overall, the percentage of nurses who would refer a child to palliative care at diagnosis or mid stage as versus end of life ranged from 57% to 88%. Comparing the results by PIC:TFK versus non-PIC:TFK site shows that more nurses in the PIC:TFK sites would refer prior to the end of life across all 11 diseases. Paired t tests revealed significant differences in referral preferences based on employment at a PIC:TFK site versus employment in a non-PIC:TFK site for all 11 diseases.
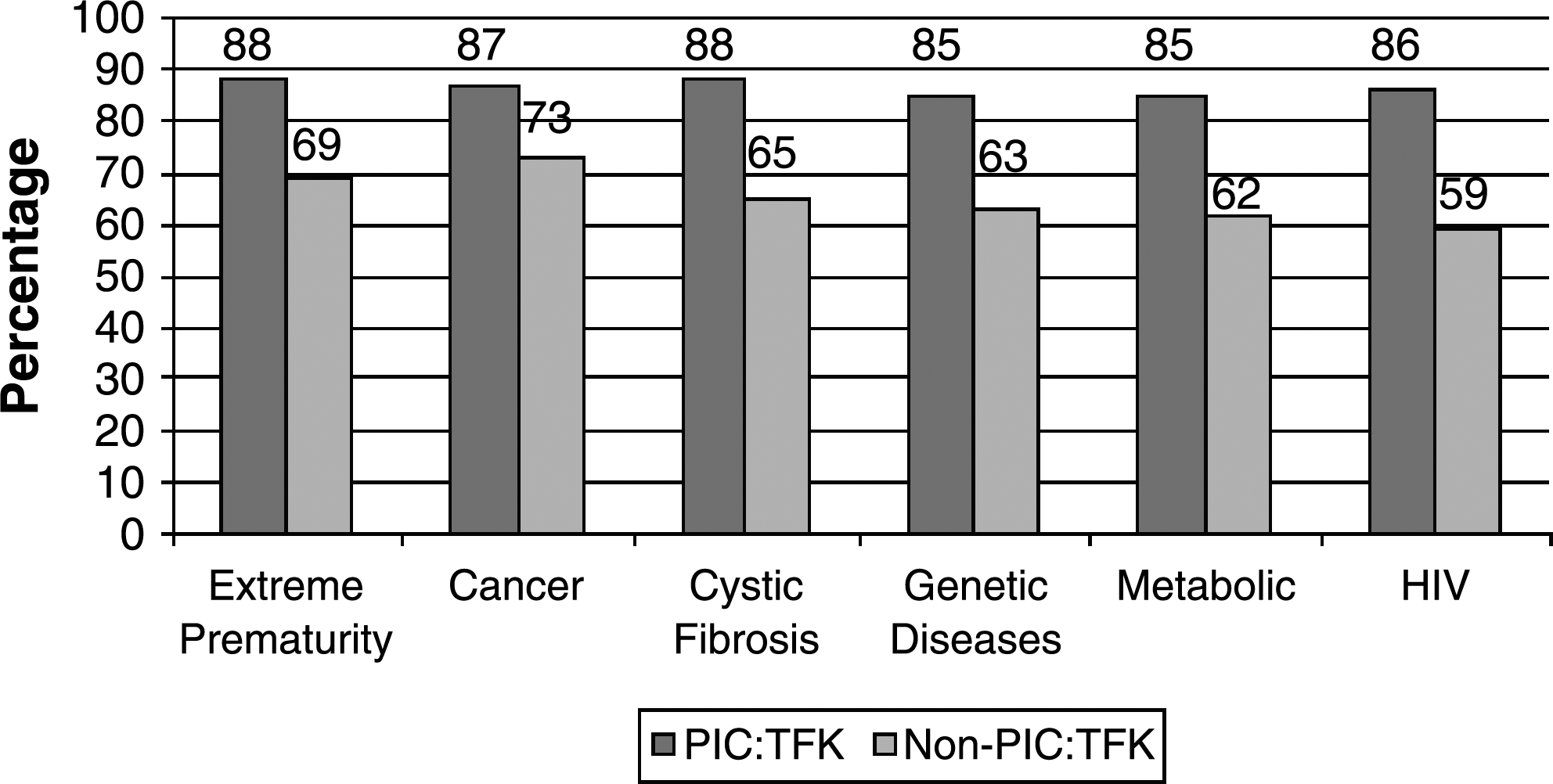
Percentage of nurses who would refer prior to end of life by disease.
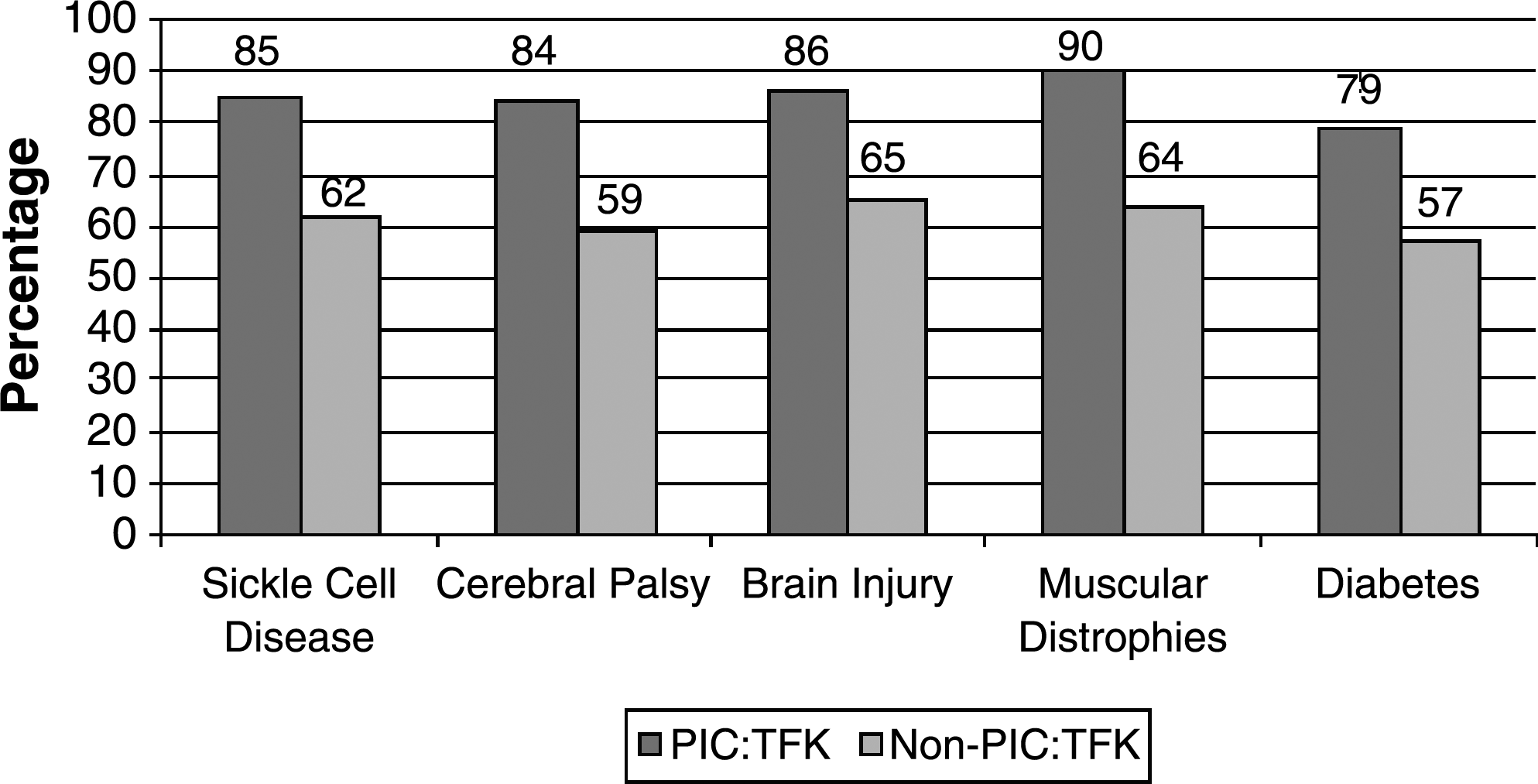
Percentage of nurses who would refer prior to end of life by disease.
Multivariate analysis of referral to palliative care
Table 2 displays the results of the multivariate logistic regressions where the dependent variable indicates that a nurse would refer a child who has cerebral palsy, muscular dystrophy, metabolic diseases, or diabetes. For the other seven diseases, none of the predictor variables were significant. For three diseases, nurses employed at a PIC:TFK site were about 2.9 to 31.4 times as likely to refer children as compared to nurses in a non-PIC:TFK site. Nurses of Hispanic and other races were less likely to refer as compared to white non-Hispanics for muscular dystrophy and nurses of other races were less likely to refer for diabetes. For metabolic diseases, nurses 20–40 years old were more likely to refer than nurses older than 50.
Referent Groups: Age 50+, Female, White, non-Hispanic, RN degree, 20+ years in practice, did not have formal training, does not work in a PIC:TFK area.
Note: —indicates that the variable dropped out of the model.
PIC:TFK, Partners in Care: Together for Kids.
Multivariate analysis of timing of referral to palliative care
Table 3 displays results of the multivariate logistic regressions where the dependent variable indicates that a nurse would refer prior to the end of life. For all 11 diagnoses, nurses at PIC:TFK sites were 3.7 to 10.4 times more likely than nurses at non-PIC:TFK sites to refer a child to palliative care at diagnosis or mid-stage. Nurses aged 41–50 were significantly less likely than nurses older than 50 to refer children with cancer prior to the end of life (p ≤ 0.05). Nurses caseload was a significant, but small factor on referring children with cerebral palsy prior to the end of life (p ≤ 0.05). Nurses of other races/ethnicity were significantly less likely than white non-Hispanic nurses to refer earlier than end of life for genetic diseases/congenital anomaly and metabolic/storage diseases (p ≤ 0.03). Formal training was associated with referral for extreme prematurity prior to the end of life.
p < 0.05.
Referent groups: Age 50+, female, White, non-Hispanic, RN degree, 20+ years in practice, did not have formal training, does not work in a PIC:TFK area.
Note: —indicates that the variable dropped from the model.
HIV, human immunodeficiency virus; PIC:TFK, Partners in Care: Together for Kids.
Although not shown in the table, we included an interaction variable in all of our logistic models equal to highest degree times being employed in a PIC:TFK site to determine if there was an interactive effect of the two variables. The interaction variable was not significant in any of the models (p > 0.05).
Discussion
This study investigated nurses' preferences to refer children with 11 diseases to pediatric palliative care, nurses' preferred timing of referral, and the effect of working in an area with a pediatric palliative care program on those referral preferences. Results of this study extend the literature in several ways.
First, our findings describing the diseases which nurses would refer to pediatric palliative care are novel. Descriptive statistics indicate that 71% or more nurses would refer a child to palliative care for 11 diseases. Bivariate results show that for all diseases, the percentage of nurses who would refer a child did not vary by PIC:TFK versus non-PIC:TFK site. This suggests that nurses' preferences are relatively uniform across all diseases.
Second, it is important to look beyond the descriptive analyses because individual factors, such as race/ethnicity and being employed in a site where the PIC:TFK program operates, might have make nurses more likely to refer. The multivariate results did not find many factors that significantly affected the preference to refer, which should be seen as encouraging to program planners and health care agencies. Being employed in a PIC:TFK site did have a positive and significant effect on referral for diabetes, cerebral palsy, and muscular dystrophies. Diabetes is generally considered a chronic illness and is only life-limiting in rare circumstances; yet, if a child's family life is unstable and the child is having difficulties adhering to a medication regime, than that child should be considered as having a potentially life-limiting condition. Nurses who are employed in site where a PIC:TFK program operates might be more willing to consider the psychosocial aspects of diabetes care when they decide that a child should or should not be referred to supportive care services. Our findings on race/ethnicity suggest that nurses of other races are less likely to refer children with diabetes and muscular dystrophy to palliative care programs. These findings demand further research as it is unlikely that lack of referral is being motivated by unfamiliarity with the diseases, especially with diabetes which has become a common pediatric disease.
Third, our descriptive findings on when nurses would refer certain diseases to pediatric palliative care are novel as well. Our results show that for all 11 diseases, more nurses who work in an area where a PIC:TFK program operates would refer children to palliative care prior to the end of life. Although these descriptive results do not adjust for potential confounders, they do suggest that for an illness such as cancer, which is potentially curable but associated with a high risk of mortality, there is disagreement among nurses as to when palliative care is appropriate. The tendency of nurses in the PIC:TFK program to prefer early referral somewhat indicates that they are in agreement with the fundamental concepts of the program and palliative care in general.
The final unique contribution of this study is the results from the multivariate analyses that describe whether or not a nurse would refer a child to pediatric palliative care prior to the end of life, after adjusting for other potential confounders. Results from the multivariate regression analyses showed that for all 11 diseases, nurses in the PIC:TFK sites would refer earlier than the end of life compared with nurses in non PIC:TFK sites. Moreover, nurses in the PIC:TFK sites were more than eight times as likely to refer children prior to the end of life for cystic fibrosis, HIV, cerebral palsy, and muscular dystrophy. These diseases are progressive and nurses who are not as familiar and comfortable with integrated palliative care might not consider them for referral prior to end of life without receiving training. We also found that younger nurses were less likely to refer children with cancer prior to the end of life versus older nurses. Perhaps our finding on cancer reflects the fact that survival rates for pediatric cancer have increased over time and younger nurses may not view these children as likely to reach terminal states as older nurses.
Several study limitations merit attention. First, the response rate for the survey was 61%. While this response rate is equal to or better than other provider surveys on palliative care, 21 there may be inherent differences between responders and non responders. Second, we did not conduct presurveys and postsurveys so we cannot comment specifically on the effect of the on-site training that the nurses received. As the PIC:TFK program expands to more sites in Florida, postsurveys will be conducted. Third, the nurses we surveyed all work in the State's Title V program that provides care for children for special health care needs. Perhaps the results would differ for nurses who work in a general practice setting. Fourth, we only asked nurses about 11 diseases. Certainly, there are a myriad of diseases that would qualify a child for enrollment into a pediatric palliative care program that we did not ask about. Most importantly, we acknowledge that clinical judgment takes precedence when making referral decisions. Nurses and physicians must consider all of the physical and psychosocial needs, not just diagnosis, for each child before making a referral decision. Finally, we do not have information on the diseases of children who were suggested for referral, but did not enroll in the program.
Despite these limitations, we believe this is the first study to describe nurse referral preferences to pediatric palliative care. Moreover, we believe this is the first study to provide evidence on the effect of a palliative care program on preferences. Our results suggest that not only is being employed in a site with a palliative care program a significant factor, it had the largest impact on referral timing. These findings corroborate existing evidence which suggests that the lack of understanding and knowledge about palliative care is a barrier to early referral. 22 In the United States, referral preferences become increasingly important as more states receive approval to provide publicly funded, integrated pediatric palliative care programs. Colorado received federal approval to provide these services in 2008 and other states are in the process of implementing programs. Recent proposed federal legislation would require all Medicaid eligible children to receive hospice services earlier than the last six months of life. 23 Consequently, our study results illustrate the need to ensure that referrals are more uniform across a variety of diseases and that referrals happen before the end of life.
Footnotes
Acknowledgment
This research is supported in part by a University of Florida Faculty Enhancement Opportunity Award given to the first author.
Author Disclosure Statement
No competing financial interests exist.