
Abstract
Abstract
Background:
Kokua Kalihi Valley is one of the first federally qualified community health centers offering home-based palliative care (HBPC). Kokua Kalihi Valley serves low-income, immigrant populations from Asia and the Pacific Islands, whose end-of-life needs are rarely addressed. Our team includes a palliative medicine physician, nurse, case manager, psychologist, interpreter, and volunteers.
Objectives:
The purpose of this Institutional Review Board-approved study was to measure symptom relief and quality of life, resource utilization, and satisfaction with HBPC.
Methods:
Over 12 months, 91 people including 46 patients with chronic advanced illnesses and 45 corresponding primary caregivers were enrolled. Data were collected prospectively, upon admission, and repeatedly thereafter, using the Missoula-Vitas Quality of Life Index, the Edmonton Symptom Assessment Scale, and the Palliative Performance Scale. Utilization of resources was tracked, including case management, hospice, emergency department, and hospital visits.
Results:
The median age was 71 years, and more than half had chronic neurodegenerative conditions. Most patients (98%) were minority, including Samoans, Filipinos, Japanese, Micronesians, and Hawaiians. Median stay in HBPC was 7 months, with a median of 3.5 visits. Approximately 25% of patients enrolled in hospice (median stay 67.5 days). There was a decrease in hospitalizations (p = 0.002) after HBPC admission. Discussions and documentation of end-of-life wishes increased from 50% to 90% (p < 0.01). Caregiver satisfaction with HBPC was high.
Conclusion:
Data on outcomes and quality indicators of HBPC programs are scant, especially among immigrant Asian and Pacific Islanders patients. Our experience demonstrates the effectiveness of palliative care approaches in this population.
Introduction
In the United States, immigrants are underrepresented in palliative care programs. 6 Yet, palliative care is rarely targeted to immigrant populations, and their end-of-life needs are rarely addressed. Worldwide, there is a serious lack of local culturally appropriate palliative care services for indigenous populations. 7 According to the World Health Organization (WHO), palliative care is an urgent worldwide humanitarian need of people with chronic fatal diseases. 8
Health disparities based on race, ethnicity, and socioeconomic status are well documented in the United States. Federally qualified health centers (FQHC) provide preventive and primary care to the uninsured and underinsured, with a mission to reduce health disparities and improve care for these groups. 9 However, few FQHCs offer palliative care services or home visits, creating a huge gap in care for patients made vulnerable by serious illness and low socioeconomic status.
Hawaii is receiving more immigrants from Asia and the Pacific Islands. In this paper, we describe a program of home-based palliative care (HBPC) serving predominantly low-income immigrants in the setting of a FQHC in Hawaii and present data from its evaluation. We discuss the implications of our findings and urge other health centers to consider replicating HBPC services.
The Home-Based Palliative Care Program
Kokua Kalihi Valley Comprehensive Family Services (KKV) is an FQHC in Kalihi Valley, Honolulu, a medically underserved area and a health personnel shortage area. 10 KKV serves a large immigrant population from the Philippines, Samoa, and Micronesia, many of whom arrive uninsured and unable to navigate the health system without assistance.
KKV established a physician home-visit program in 2002, and this was expanded in 2003 to a structured HPBC program. The goal is to improve access and deliver culturally sensitive palliative care to homebound patients with advanced chronic illnesses so as to reduce the emotional, spiritual, and physical suffering experienced by patients and caregivers. The team includes a physician who is board-certified in geriatrics and palliative medicine, a nurse, a case manager, a psychologist (who is also a pastor), interpreters, and volunteers. KKV can deploy a large interdisciplinary team because as an FQHC, it employs a variety of practitioners, including eligibility and outreach workers who speak the commonly used native languages. KKV serves as a palliative care clinical rotation site for students at the local nursing, medical and law schools. Community partnerships with local pastors living in the valley provide patients and families with spiritual support. Referrals to HBPC come from other KKV providers and from the community. Any homebound adult patient, age 18 or older, with a chronic advanced illness is eligible.
Methods
Funds were received from a local foundation for a 1-year evaluation of the HBPC program. A prospective design was used, in that data were collected from patients and caregivers upon admission to the HBPC program and then every few months thereafter. However, there was no control group; data on medical care utilization prior to admission to the service were collected retrospectively from patient's medical records, and these findings provided a historical control. Prior to the study, Institutional Review Board approval was obtained from the University of Hawaii. Patients or their designated proxy provided consent to participate in this study and authorized researchers to access medical information related to the study.
The objectives of this study were to measure: (1) symptom relief; (2) quality of life; (3) use of community resources; (4) hospitalization and emergency department visits; (5) advance care planning; and (6) satisfaction with HBPC.
Sample
Over a 12-month period (February 2007 to January 2008), 91 HBPC clients were enrolled in the study, including 46 adult patients (ages 27–94) with advanced chronic illnesses and 45 corresponding primary caregivers. All patients met the Medicare homebound definition. Excluded were 2 patients with terminal delirium and 1 who was unable to give informed consent.
Measures
Demographic data were collected upon admission, including age, gender, ethnicity, diagnostic category, insurance status and living arrangements. Research measures were administered prospectively upon admission and every visit thereafter. The Palliative Performance Scale (PPS) was used to measure performance status in palliative care. 11 The PPS assigned a number to the patient that reflects the percentage of functioning. For example, a score of 80%–100% means that the patient is fully ambulatory and independent in self-care.
The Edmonton Symptom Assessment Scale (ESAS) was used to provide a clinical profile of symptom severity over time. 12 The ESAS assesses nine symptoms or conditions, including pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, well-being, and shortness of breath. Each item is rated on a scale from 0 to 10 with 0 being the “best” option for each symptom or condition, for example, no pain, no fatigue, excellent appetite, and best well-being.
The Missoula Vitas Quality of Life Index (MVQOLI) was developed specifically to assess the multidimensional quality of life of patients who are aware of their terminal condition and understand that the goal of treatment is palliative. 13 Five domains are assessed: symptoms, functioning, interpersonal relationships, well-being, and feelings of transcendence. Each item and domain can be scored from −30 (representing no symptom control, well-being, and so forth) to +30 (best symptom control, well-being, and so forth).
We tracked advance directives (AD) and code status. The Hawaii AD allows individuals to give instructions about wishes for end-of-life care in the event of incapacitation (also known as living will) and/or designating a proxy or surrogate to make health care decisions in the event of incapacitation (also know as durable power of attorney for health care). Code status preference were discussed: full code meaning that the health care team perform cardiopulmonary resuscitation in event that heart beat and breathing stop, DNR meaning do not resuscitate, and modified code accompanied by special instructions.
One of the goals of the HBPC program was to reduce the use of emergency department and hospital. In this study, data about emergency department visits and acute care admission were obtained during the study period. There was good accuracy and ease of tracking these data because Hawaii is a small island and KKV providers cared for patients in the hospital in addition to outpatient and home settings. We then examined medical records for a similar period prior to HBPC. For example, if someone was enrolled in HBPC for 6 months, we compared emergency department use over those 6 months with emergency department use during the 6 months prior to enrollment in the study. We also tracked the use of community resources such as respite and hospice.
Our 15-item caregiver satisfaction survey was based on the Famcare scale, a 20-item scale that assesses the family satisfaction of care provided to patients with advanced cancer. 14 Our survey incorporated 10 of the 20 Likert-scored items (related to symptom relief, referrals, and coordination of care) and added 5 more on AD, community referrals, emotional and spiritual support, financial assistance, and overall care. Caregivers were asked to rate their satisfaction with services at most visits.
Finally, bereaved family caregivers were interviewed by telephone 1 month after the death of their loved one. We use the Data Analysis and Report for Toolkit (DART), a tool of the National Hospice and Palliative Care Organization, and followed instructions for creating percentages satisfied with 4 domains: (1) care coordination; (2) attention to family needs; (3) communication; and (4) information. 15
Analysis
Data analysis was performed using SPSS version 14 (SPSS, Chicago, IL). Frequencies and descriptive statistics were calculated for demographic variables and responses to survey questions. Changes in emergency department and hospital admission pre–post study enrollment were tested using paired t test for means, χ2 for distributions, and Wilcoxin signed- rank test for improvement. Changes in AD completion were calculated using χ2. Changes in baseline and follow-up measures for ESAS, PPS, and MVQOLI were tested using paired t tests. DART findings were compared with national averages.
Results
The median stay in the program for enrollees was 7 months, and the median number of visits was 3.5. The demographic and clinical characteristics of the study population are summarized in Tables 1 and 2, respectively. Of the 46 patients 20 were males and 26 females. All had medical insurance. Ages ranged from 27–94 years with the median age of 71 years. More than half had chronic neurodegenerative conditions. The second most common diagnosis was cancer. All patients but one were minority (including Samoan, Filipino, Japanese, Micronesian, and Hawaiian). The mean PPS was 50% at baseline and did not change over time. At the end of the study 37 (80%) of the patients were still alive.
COPD, chronic obstructive pulmonary disease; ADL, activities of daily living; IADL, Instrumental Activities of Daily Living.
The most common symptoms experienced by the patients were nausea and shortness of breath. For most symptoms, there were trends toward improved control. Although none of the change scores were statistically significant (due to the small sample size and large standard deviations), the percentage of patients with “good” scores (less than 3 of 10) increased from 59% to 81% for anxiety and from 57% to 71% for pain.
Findings of the Missoula Vitas Quality of Life survey are shown in Table 3 for the 23 (50%) patients who completed it at least 4 different times. There was an improved sense of well-being (p = 0.03) but no change in the other domains including symptoms, functioning, interpersonal, or transcendence. PPS score was unrelated to whether or not the patient improved in his/her quality of life scores. However, being a Pacific Islander was related to a lower global quality-of-life score (p = 0.03).
A positive number signifies an improvement in score, while a negative number signifies a worsening in score.
SE, standard error.
Significant improvement was found in AD planning before and during HBPC (Fig. 1). At baseline 25 (55%) patients stated they had an AD, but copies were in the charts for only 8 (17%) patients. By the end of the study period, 90% of patients had completed AD, and copies were in the charts of 65% of patients. The percentage of clients with DNR orders increased from 50% to approximately 60% (Fig. 2).
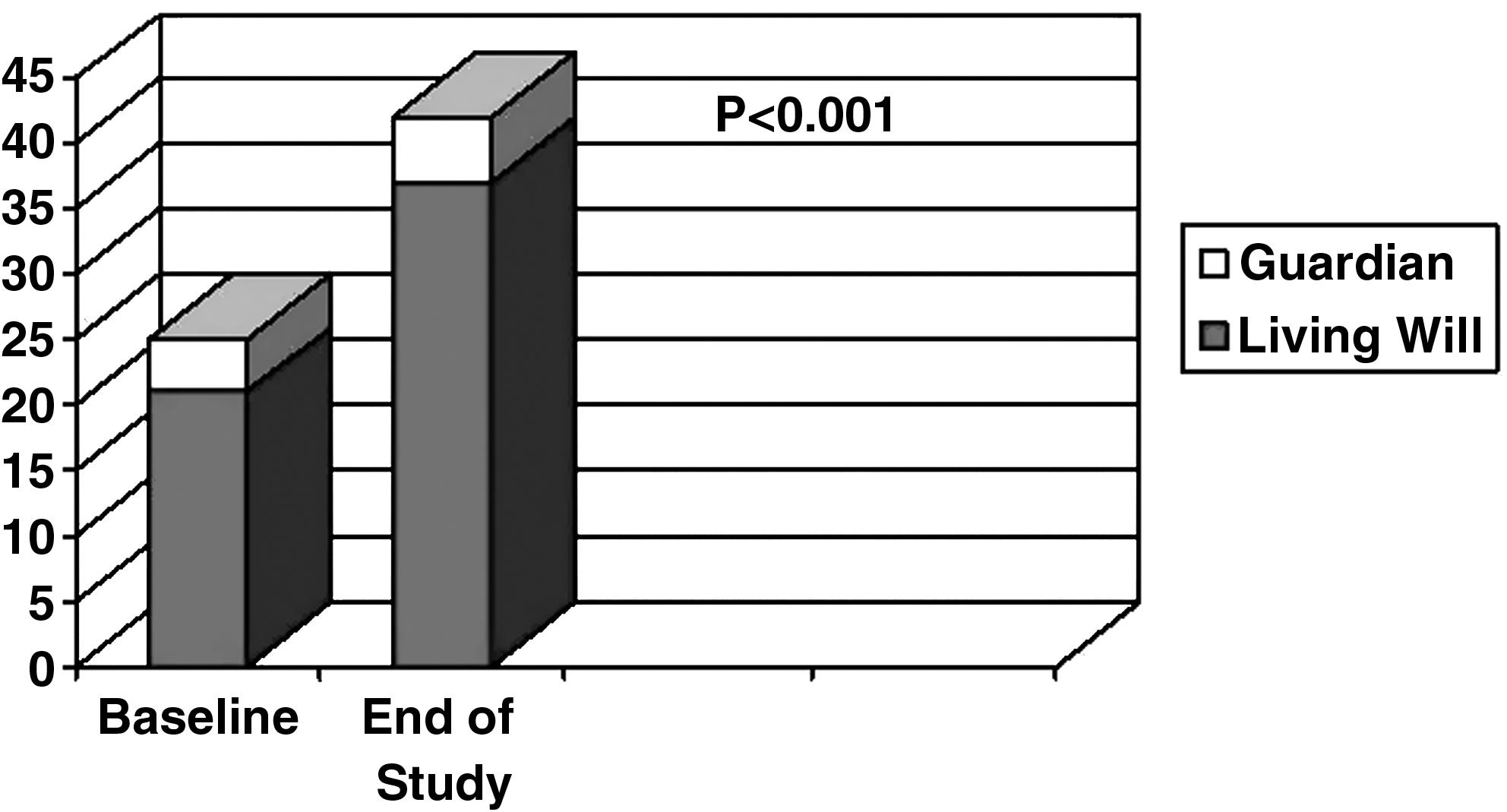
Advance directives.

Code status of participants.
Emergency department use was essentially unchanged; 65% of patients had no emergency department preceding the study, and 67% had no emergency department visits during the study. However, reduction in acute care admissions was significant. The percent of patients who had no acute care admissions increased from about 48% to 74% (p = 0.002), as shown in Figure 3.
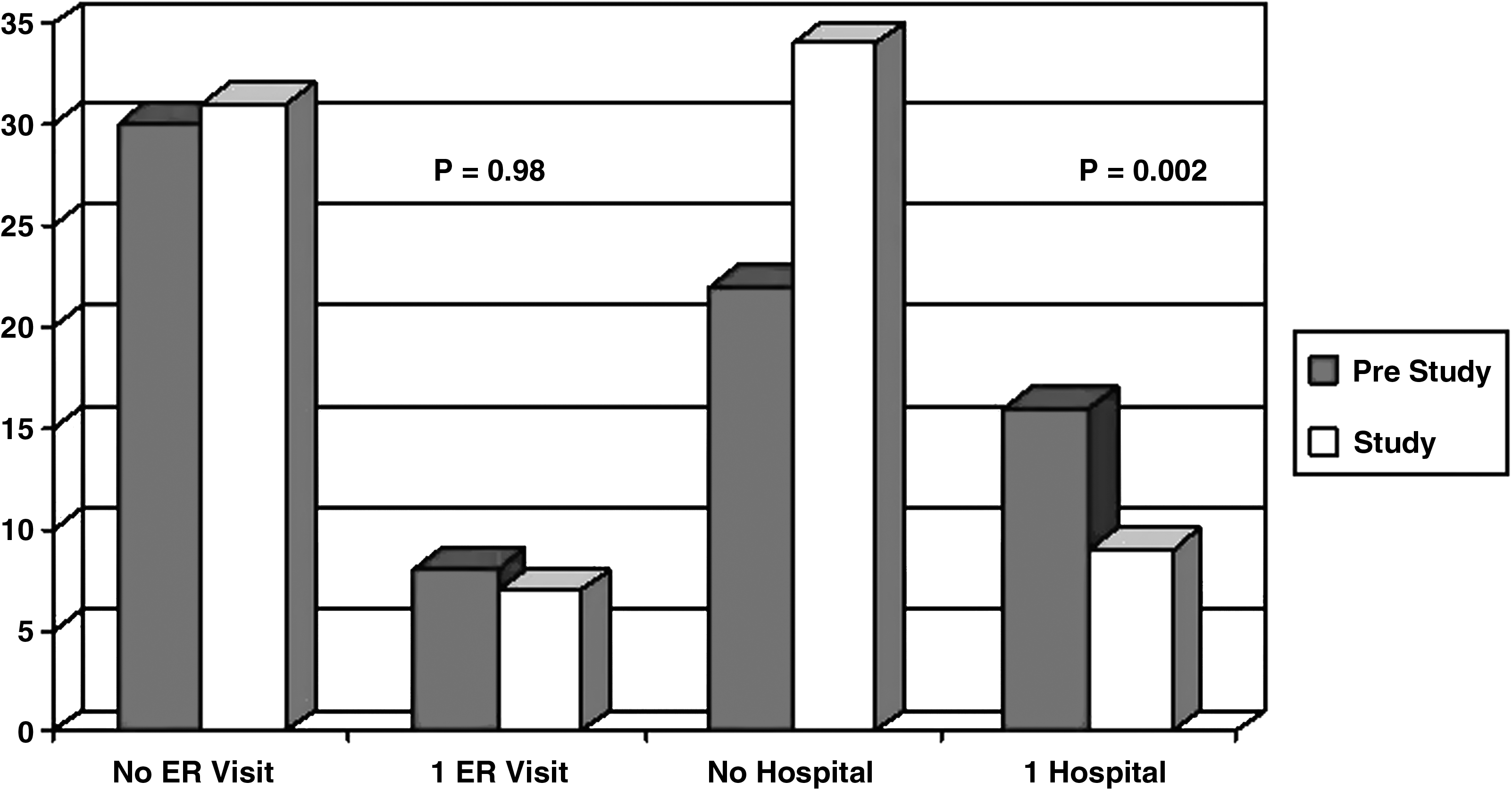
Emergency department and hospital visits.
The most utilized support service during the study year was case management (Table 4). Approximately 85% (39/46) of HBPC patients received case management through various sources; 14 internally from KKV, 11 externally from community agencies, and 3 from both. Patients with a lower level of functioning (based on PPS) were more likely to use case management (p = 0.03) and respite (p = 0.05) during the study period. Pacific Islanders were more likely that other groups to use case management services (p = 0.02). Hawaii has a critical shortage of nursing homes; the majority of long-term care is provided by families, making case management key. Twelve patients were enrolled in hospice, including 7 of the 9 who died during the study period; their median length of hospice stay was 67.5 days.
All 45 caregivers completed the satisfaction surveys at most visits. The level of satisfaction was generally high and stable, hence mean satisfaction scores were calculated for each caregiver. Mean item satisfaction ranged from 4.2 (satisfaction with relief of patient's pain) to 4.8 (satisfaction with the overall care provided by the HBPC team). The DART was completed by caregivers of 8 of the 9 patients who died. Percentages satisfied with the 4 DART domains were comparable to or higher than national averages (Table 5). Caregivers also wrote notes, such as: “I'd like to thank [you]. Without your support we don't know what we supposed to do. May God bless you doctor and your group” and “It's very convenient for Mrs. C since she's having hard time going to her doctors whenever she gets sick. This is the best service we ever get and we appreciate it very much.”
HBPC, home-based palliative care.
Discussion
In 1990, WHO noted that “the ultimate goal of palliative care is the achievement of the best quality of life for patients and their families.” 16 Quality of life serves as the final common pathway for palliative care services, and satisfaction with care and well-being are frequently used outcome measures for both patient and family members.17,18 Despite our small sample size, HBPC patients reported significant improvements in well-being, and caregivers were extremely satisfied. Similar to other studies we too found that the MVQOLI scores did not have any prognostication value, and agree that better prognostication instruments are needed. 19
In addition, the program demonstrated the ability to stabilize the care of seriously and terminally ill patients at home, minimize the pain and anxiety for most clients, improve advance care planning, reduce hospitalizations, and increase appropriate use of community resources. Our findings were similar to those of Brumley and colleagues, 4 who found that within the Kaiser system in-home palliative care significantly increased caregiver satisfaction while reducing costs of medical care at the end-of-life. Along the same line, palliative care case management at a Veterans Affairs Medical Center was associated with decreased use of acute care services for patients dying of cancer. 5 Although we could not conduct a cost analysis of HBPC, we believe that like other palliative care services, our program saves resources by reducing hospitalizations and maximizing use of community-based services.
In organizing a HBPC service, we found a team approach to be of greater value than lone provider home visits. The team comprising of bilingual case managers was key to building trust in the health care system by bridging cultural and language gaps. Delivery of HBPC is best done by routine home visits scheduled every 2–3 months. The team delivers medical care, assesses caregivers for stress and burnout, and provides patient and family education. Case managers visit the family every 2–4 weeks and link them with appropriate community resources. For example, if the client needs companionship and respite, the case manager may assign a volunteer senior companion or respite worker. Counseling may be provided by a case manager or a psychologist. Discussions on AD and hospice are initiated by the physician, with follow up by case managers. Monthly caregiver support groups provide education and help caregivers with coping and relaxation. Home visits by other providers, such as a psychiatrist and nutritionist, can be scheduled; and interventions such as wound care, blood tests, and immunizations are provided in the home. The medical insurance is billed for services provided by physician and psychologist. Local partnerships with universities, churches, and other entities helped us expand the team and provided additional help in screening and monitoring clients.
Research suggests that minority Americans are less likely than Caucasian Americans to complete AD and more likely to prefer family-based decision making (versus autonomous decision-making) about care choices. 20 Our high rate of AD completion was likely due to the ability of team members to establish trusting relationships over time with patients and families, the availability of bilingual case managers to help explain end-of-life concepts to non-English–speaking patients and families, and the team's ability to facilitate family-based decision-making for clients that preferred it. Satisfaction with family inclusion in treatment and care decisions was high (4.5/5).
Also, research suggests that minority Americans are less likely that Caucasian Americans to use hospice care. 21 In this study, of the 46 patients receiving palliative care 14 were terminally ill and eligible for hospice. Twelve patients were ultimately enrolled (85%). These were minority Americans that included: 5 Filipinos, 3 Micronesians, 1 Samoan, 1 African American, 1 Japanese, and 1 Laotian. The median length of hospice stay was 67.5 days, which is in contrast to existing literature on Asian Americans length of stay 32 days. 22 Again, we attribute this success to the team's ability to take patients into HBPC before there is a crisis and demonstrate over time their commitment to providing the right services at the right time to meet patient and family needs.
Burnout is a concern for individuals caring for chronically ill home-bound family members. 23 In this study, caregiver burnout was monitored, and caregivers were provided counseling and/or encouraged to participate in caregiver support groups provided by the FQHC. Although we did not measure caregiver burnout explicitly, findings from the caregiver satisfaction survey suggest that the service was able to help them cope, e.g., mean satisfaction rankings were 4.5 for emotional and spiritual support and for assistance with financial issues.
Our study contributes to the literature in several ways. First, we present a model of a successful HBPC services based in a FQHC, and to our knowledge, this is the first such report. Second, our populations was very diverse and disadvantaged, with 98% (45/46) classified as minority and 67% (31/46) living below 100% of federal poverty level; suggesting that this service is appropriate for homebound, chronically ill Americans from a broad range of backgrounds. This population present challenges that arise from the complex interplay of advanced illness, low functional status, limited English skills, low health literacy, poverty, and cultural consideration. The principal limitation of this study is that data collection was inconsistent at times due to low functional status of the patient, acute medical issues, or caregiver stress. This is similar to other studies in palliative medicine research that face challenges due to recruitment, attrition, and compliance. 24
Conclusions
Future directions for research in Hawaii involve qualitative approaches such as focus groups or structured individual interviews to expand our understanding of the complex interplay of psychosocial factors and palliative care in special populations. Health services research conducted over a longer period of time could further examine the benefits and cost-effectiveness of our HBPC service. In our study, HBPC was found to be an effective and welcomed service provided to clients by a FQHC in Hawaii. Health centers like ours have a potentially important role in providing palliative care services to underserved communities.
Footnotes
Acknowledgments
We thank all the case managers, interpreters, and volunteers at Kokua Kalihi Valley Comprehensive Family Services for their assistance with this study. We are grateful to the HMSA Foundation for funding this pilot study.
Author Disclosure Statement
No competing financial interests exist.