
Abstract
Abstract
Background:
The development of palliative care educational programs is ongoing in Japan. To assess the effectiveness of educational programs for general nurses, it is necessary to develop scales for evaluating them.
Aims:
The aims of this study were to develop two scales to measure the effectiveness of palliative care educational programs and confirm the validity and reliability of the scales.
Methods:
A questionnaire survey was validated with a group of 940 nurses at two facilities. The response rate was 85% (n = 797). This study used psychometric methods such as factor analysis and intra-class correlation coefficients.
Main results:
We selected 18 items in 6 domains, including “dying-phase care,” “patient- and family-centered care,” “pain,” “delirium,” “dyspnea,” and “communication” for the Palliative Care Self-reported Practices Scale (PCPS). For this scale, the intra-class correlation was 0.64 to 0.74 in each domain. For the Palliative Care Difficulties Scale (PDCS), we selected 15 items in 5 domains, including “communication in multidisciplinary teams,” “communication with the patient and family,” “expert support,” “alleviation of symptoms,” and “community coordination.” For the PCDS, the intraclass correlation was 0.61 to 0.69 in each domain.
Conclusions:
The validity and reliability of these scales were established. Therefore, the clarification of actual practices used and difficulties experienced will be possible using these scales.
Introduction
To date, studies of palliative care educational programs in foreign countries have shown that knowledge and skills can be improved.6–9 The dissemination of palliative care for cancer patients is a national policy in Japan. Currently, the Outreach Palliative Care Trial of Integrated Regional Model (OPTIM) study, a nationwide demonstration project, is being conducted in order to improve palliative care throughout Japan. 10
In order to deliver quality educational programs, it is necessary to conduct evaluations to determine whether an educational program is effective. Such evaluations can assess individual achievement, clarify the effectiveness of the program and provide information on whether the program should be continued. Therefore, a valid instrument is needed. One evaluation indicator for an educational program is knowledge. Other indicators of program quality are change in self-reported practices, attitudes and difficulties.11–19 We considered that knowledge, practices, and difficulties with palliative care are interlinked; therefore, an assessment of palliative care would need to include a knowledge test, a self-reported practices scale, and a difficulties scale. In a previous manuscript, we reported on the Palliative Care Knowledge Test (PCKT) for health professionals. 20
Published studies have generally focused on attitudes toward terminal care; however, practices in broader areas of palliative care have rarely been investigated.9,19,21,22 Furthermore, we found little information on the psychometric properties of the measures used. The most frequent measurement for evaluating attitudes about palliative care among nurses is the Frommelt Attitude Toward Care of the Dying (FATCOD) scale. 23 The validity and reliability of this instrument have been confirmed. However, there are some limitations in the assessment of the FATCOD. Some reports have addressed the difficulties nurses experience when providing palliative care11,14,24; however, the scales used in these reports also had some limits. Consequently, we felt that the development of new instruments would be useful for the following reasons: (1) As many studies have shown that terminal patients experience a variety of symptoms,25–27 we wanted to evaluate a wider range of practices, including care for patients with delirium and dyspnea, which often arise in end-stage cancer patients. (2) We wanted to develop instruments that are not limited to terminal care and are more in accord with the recent declaration by the World Health Organization (WHO) that palliative care is applicable even early in the course of illness. 1 (3) We wanted to evaluate the difficulties with community coordination for palliative care that were an aim of the OPTIM study. (4) We wanted to develop instruments to evaluate not only nurses but also other health professionals who participate in educational programs. (5) We wanted to briefly and easily evaluate practices and difficulties with palliative care.
The aims of this study were twofold: (1) to develop and validate the PCPS and the PCDS and (2) to identify factors associated with self-reported practices and difficulties with palliative care in order to improve the curricula of palliative care educational interventions.
Methods
Design
This survey was designed as a cross-sectional, anonymous, self-administered questionnaire. To examine the test–retest reliability of items and domains, the questionnaire was reissued 2 weeks after the first one was completed. The ethical and scientific validity of this study was approved by the Institutional Review Board in one hospital. Because there was no Institutional Review Board in the other hospital, the study was approved by the director of the hospital.
Sample
The survey was conducted in August 2007 in 2 hospitals. The subjects were 940 nurses from a university hospital (661 beds) and a general hospital (634 beds) located in Yokohama City, Japan. Both facilities had inpatient palliative care units. The inclusion criterion for the subjects was that they were registered nurses. The retest was conducted for subjects who had consented to participate during the first assessment (n = 204).
The questionnaire and cover letter were distributed to nurses in each ward. The cover letter explained that this survey was confidential and anonymous. Consent to participate was indicated by the completion and return of the questionnaire. For the retest, the questionnaire was distributed again in each ward. Completed questionnaires were collected in a box placed in the ward.
Procedure
Development of scales
We developed two instruments to quantify self-reported practices and difficulties experienced by general physicians and nurses in providing palliative care. Item generation was based on literature reviews and discussions among nine experts.9,17,24,28,29 Content areas in the self-reported practices scale included pain, dyspnea, psychiatric problems, communication, and care of patients in the dying phase. Also, content areas for the difficulty scale included alleviating symptoms, expert support, communication, and community coordination. A pool of 141 items about self-reported practices and 121 items about difficulties were generated. To achieve face validity, a multidisciplinary expert panel (3 palliative physicians, 4 certified nurse specialists in oncology and 2 home care nurses) rated the appropriateness of each item. First, experts evaluated the appropriateness of each item (0 = inappropriate, 1 = somewhat inappropriate, 2 = somewhat appropriate, 3 = appropriate). Next, the mean, minimum and maximum were calculated, and items that had a mean of less than 2 and a minimum of 0 were deleted. Subsequently, we repeated the discussion with the experts to achieve face validity for the item. As a result, a preliminary list of 40 items was selected from each pool of questions.
Questionnaire
PCPS: preliminary 40 items.
PCDS: preliminary 40 items.
Number of patients with terminal cancer cared for before and in the past year,
Experience of working at a hospice or palliative care unit,
Hours of palliative care education,
Existence of a mentor for end-of-life issues,
Demographic factors.
We included factors 3 through 6 as potentially related to palliative care practices and difficulties experienced by general nurses. The initial questionnaire was in Japanese.
Definitions
In this study, “patients with terminal cancer” was defined as follows: “patients with cancer who are not likely to respond to treatment and whose life expectancy is less than 6 months.” Furthermore, “mentor” was defined as “a person (physician/nurse/family member/friend) with whom a health professional can talk about palliative care.”
Statistical analyses
Item selection
Participants who responded to 90% or more of 40 items (each scale) were the subjects of the analysis. First, item analysis was conducted. We considered the percentage of missing data to enhance feasibility (cutoff: missing more than 1% of data) and ceiling effect to enhance sensitivity (cutoffs: more than 90% of responses are 1 or 5 on a 5-point Likert-type scale). Second, to examine the test-retest reliability of each item, the κ coefficients were calculated. We considered the reliability of each item (cutoffs: κ coefficients of 0.3 or less). Then, to achieve content validity, we repeated the discussion with the experts. Based on the results of the analysis, specific items were selected if they seemed to have high sensitivity.
PCPS
We defined self-reported practices as the level of self-reported adherence to recommended clinical practice guidelines in palliative care. Self-reported practices were evaluated using a Likert-type scale from 1 (not at all) to 5 (always). Because we hypothesized that no single higher structure exists for the 5 domains, we defined the score on the PCPS as the total score of the responses in each domain. Thus, practice subscores ranged from 3 to 15, with a higher score indicating a higher level of performance of recommended practices.
PCDS
We conceptualized difficulties about palliative care. These were evaluated by agreement with statements on a Likert-type scale from 1 (never) to 5 (very much). The instructions described situations when health professionals face difficulties providing palliative care. We defined the score on the PCDS as the total score of the responses in each domain, and thus difficulty subscores ranged from 3 to 15. Higher scores indicated a higher level of difficulties providing palliative care.
Reliability and validity
To determine internal consistency, Cronbach α coefficients were calculated. The test–retest reliability was determined by calculating intraclass correlation coefficients with 2-week interval administrations.
The construct validity of each scale was examined using exploratory factor analysis with promax rotation because a single factor structure had been hypothesized. Standard regression coefficients were taken as the minimum of 0.4. To explore known-group validity, an unpaired t test was done to determine differences between a group of nurses working in palliative care units and a group of nurses working in other units. The total scores of each domain were examined with the unpaired t test.
Related factors
To identify factors associated with palliative care practices and difficulties experienced by general nurses, univariate analyses were conducted using the unpaired t test, analysis of variance (ANOVA), and Pearson product-moment correlation coefficients, where appropriate. Thereafter, the association of each hypothesized factor with the total score of each domain was confirmed using multivariate linear regression. Statistical analysis was performed using SAS version 9.1 (SAS Institute, Cary, NC). The significance level was set at <0.05 (two-tailed).
Results
Of 940 questionnaires delivered to nurses, 797 were returned (response rate, 85%). Of the 797 initial responses, 204 nurses agreed to take the retest and 151 questionnaires were returned (response rate, 74%). The characteristics of the respondents are summarized in Table 1.
The percentages do not add up 100% due to missing values.
Validation study: PCPS
The results of the item analysis are shown in Table 2.
Participants who responded to 90% or more of the 40 items were the subjects of the analysis.
Feasibility and ceiling effect
Missing values that indicate feasibility were less than 1.5% for each item. The ceiling effect was not confirmed.
Reliability of each item
The κ coefficient for the test–retest reliability of each item ranged from 0.34 to 0.58.
Reliability and validity of the PCPS
On the basis of the results of the item analysis and expert discussions, we selected 18 items in 6 domains for the PCPS: (1) dying-phase care, (2) patient- and family-centered care, (3) pain, (4) delirium, (5) dyspnea, and (6) communication. The construct validity is shown in Table 2. The exploratory factor analysis revealed a single structure, which consisted of 6 factors. Table 3 summarizes the internal consistency and test-retest reliability of the PCPS. Cronbach α coefficients were from 0.80 to 0.91 in each domain. The intraclass correlation in the test–retest examination was from 0.64 to 0.74 in each domain. Also, to examine the known-group validity, we compared the scores in each domain for nurses working in palliative care units and other nurses (Fig. 1).
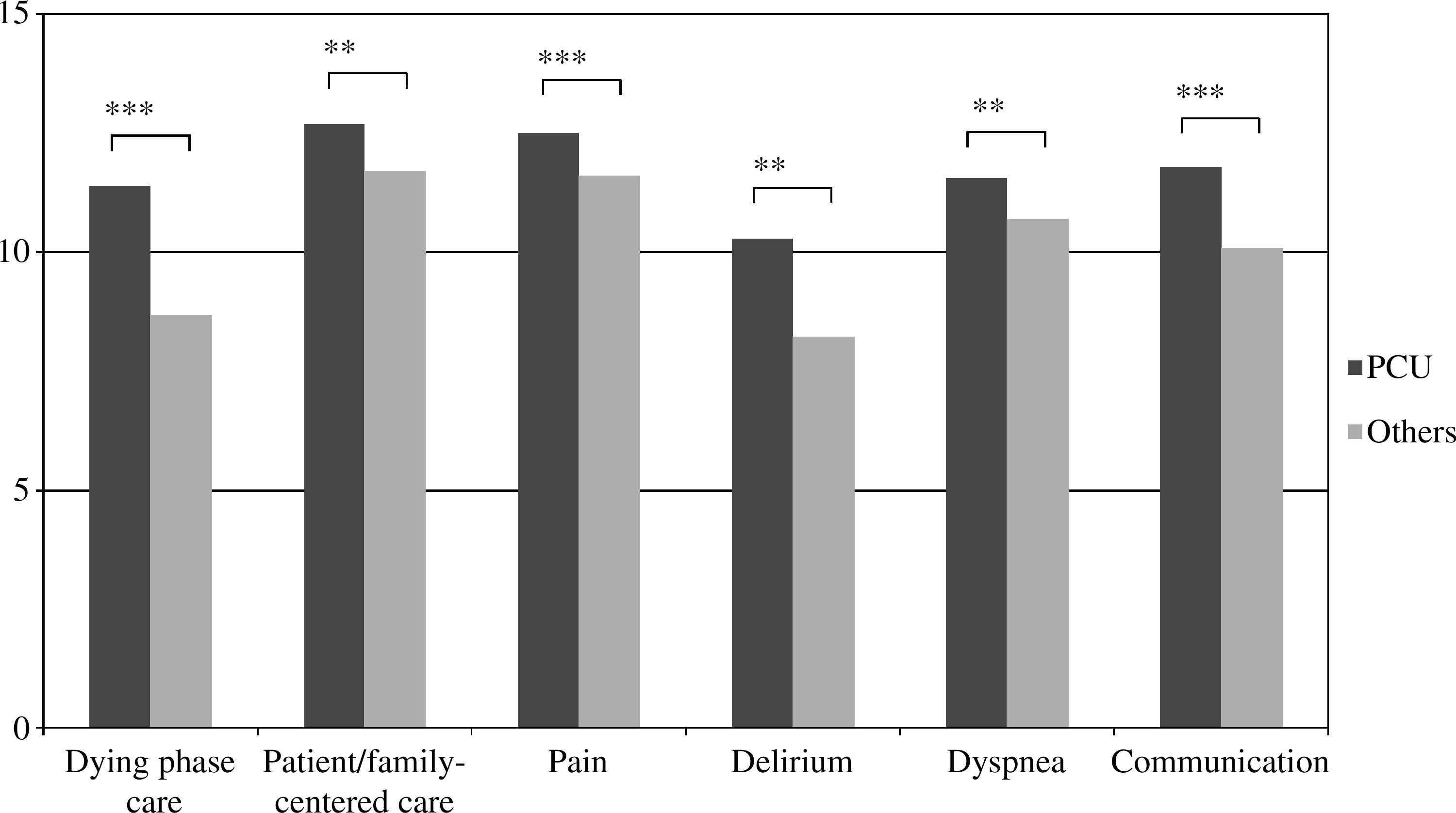
Known-group validity of the Palliative Care Self-Reported Practices Scale. The t test was used to compare the total scores in each domain for nurses working in palliative care units (PCU) compared to other nurses. *p < 0.05; **p < 0.01; ***p < 0.001.
SD, standard deviation; ICC, intraclass correlation coefficients.
PCDS
The results of the item analysis are shown in Table 4.
Participants who responded to 90% or more of 40 items were the subjects of the analysis.
Feasibility and ceiling effect
Missing values that indicate feasibility were less than 1.5% in 40 items. The ceiling effect was not confirmed.
Reliability of item
The κ coefficient in the test–retest reliability of each item was from 0.3 to 0.53.
Reliability and validity of the PCDS
On the basis of the results of the item analysis and expert discussions, we selected 15 items in 5 domains for the PCDS: (1) communication in multidisciplinary teams, (2) communication with the patient and family, (3) expert support, (4) alleviation of symptoms and (5) community coordination. The construct validity is shown in Table 4. The exploratory factor analysis revealed a single structure, which consisted of 5 factors. Cronbach α coefficients ranged from 0.85 to 0.93 in each domain. The intraclass correlation in test-retest examination was from 0.61 to 0.69 in each domain (Table 5). Also, the known-group validity was examined in the same way as for the PCPS (Fig. 2).

Known-group validity of the Palliative Care of Difficulties Scale. The t test was used to compare the total scores in each domain for nurses working in palliative care units (PCU) compared to other nurses. *p < 0.05; **p < 0.01; ***p < 0.001.
SD, standard deviation; ICC, intraclass correlation coefficients.
Related factors
Factors associated with self-reported practices
Univariate analyses of self-reported practices scores identified significant differences for many variables (Table 6). The number of terminal care patients the nurse had ever cared for was associated with a higher score for every domain including “dying-phase care” (r = 0.46, p < 0.001), “patient- and family-centered care” (r = 0.29, p < 0.001), “pain” (r = 0.31, p < 0.001), “delirium” (r = 0.33, p < 0.001), “dyspnea” (r = 0.27, p < 0.001) and “communication” (r = 0.31, p < 0.001). These results were confirmed by multivariate linear regression analysis. Furthermore, the presence of a mentor for palliative care issues was associated with a higher score for every domain. By multivariate linear regression analysis, an association was reported for the presence of a mentor and higher practice level only for “dying-phase care” (β = 0.09, p < 0.05) and “patient- and family-centered care” (β = 0.12, p < 0.01).
p < 0.05.
p < 0.01.
p < 0.001.
Numbers in the table represent means or correlation coefficients.
Factors associated with difficulties
Univariate analyses of the difficulties score identified a significant difference for many variables (Table 7). The number of terminal care patients the nurse had ever cared for was associated with lower scores for the domains “communication with the patient and family” (r = −0.27, p < 0.001), “expert support” (r = −0.09, p < 0.05), and “alleviating symptoms” (r = −0.31, p < 0.001). Many of the nurses who participated in seminars and who had mentors for palliative care had lower scores for “communication with the patient and family,” “expert support,” and “alleviating symptoms.” Furthermore, results of multivariate linear regression confirmed that clinical experience and terminal patient care experience were associated with a lower score for “alleviating symptoms.” Also, multivariable linear regression confirmed the association between frequency of participation in palliative care seminars and lower score for “communication with the patient and family” (β = −0.15, p < 0.01).
p < 0.05.
p < 0.01.
p < 0.001.
Numbers in the table represent means or correlation coefficients.
Discussion
This study validated two scales that evaluate self-reported practices and difficulties experienced by general nurses in providing palliative care. Both these scales have good internal consistency, test-retest reliability, face validity and construct validity.
They add the following to already existing instruments: (1) they provide the ability to evaluate a wider range of palliative care practices; (2) they can be used not only for terminal care but also for palliative care that is given early in the course of illness; (3) they could be used in research to evaluate health professionals other than general nurses; and (4) the scales are concise and easy to administer.
Consequently, these scales can be used to identify practices and difficulties in providing palliative care, assess problems and evaluate educational programs. Results from the evaluations can help improve the quality of education received by health professionals and ultimately the quality of palliative care received by patients and their families. Moreover, these scales can be used as an objective measure for individuals for determining areas in need of improvement. The PCDS can be used to identify difficulties experienced by nurses and to help them develop strategies.
This study explored the factors related to nurses' practices and difficulties in palliative care. One of the most important findings was that the number of terminal cancer patients the nurse had ever cared for was associated with a higher score in 6 domains of the PCPS. Some research has shown that there is a relationship between positive attitudes toward caring for dying patients and nurses' experiences of caring for dying patients, discussion of hospice with patients and the number of terminal care patients a nurse had ever cared for.22,28,30 These results are consistent with our findings. The number of terminal cancer patients the nurse had ever cared for was also associated with a lower score in three domains including “communication with the patient and family,” “expert support,” and “alleviating symptoms” on the PCDS. These results support the view that education is necessary for nurses with less experience who care for patients with terminal cancer.
Furthermore, the existence of a mentor for palliative care was associated with higher scores for every domain on the practices scale. This factor was also correlated with lower scores in three domains including “communication with the patient and family,” “expert support,” and “alleviating symptoms” on the difficulties scale. Previous research has shown that the existence of a mentor decreased the difficulty nurses experienced. 24 We believe that results of the present study further emphasize the need for a palliative care team. The palliative care team provides support for health care professionals and has been reported to have a positive impact on the management of patient symptoms, discharge planning and staff support.31,32 Therefore, the presence of an expert to consult about palliative care, such as a palliative care team or clinical nurse specialist, can help improve care for patients with cancer.
The generalizability of this study and the two instruments is significantly limited by the fact that only nurses were surveyed. The scales developed in this research were also intended for use with health professionals other than nurses who are directly involved with palliative care; however, the subjects of this survey were only nurses, although physicians were included in the design of the questionnaire. Therefore, to provide more generalized scales, these instruments must be evaluated psychometrically with other types of health care providers. Furthermore, subjects were only recruited from two facilities in one country. This sample is not sufficiently representative to allow for the generalization of this study to other populations. Additionally, future research should demonstrate improvement in provider behavior and patient outcomes.
Footnotes
Acknowledgments
The authors would like to express special thanks to Kumi Hasegawa, R.N., O.C.N, Hitomi Higuchi, M.D., Yasuko Nakayama, R.N., Ph.D., Taketoshi Matsumoto, M.D., Mikako Takahashi, R.N., O.C.N., and Chikako Uchida, R.N. for helpful advice.
Author Disclosure Statement
No competing financial interests exist.