
Abstract
Abstract
Background:
Research during the past few decades has greatly advanced our understanding of the cost, quality, and variability of medical care at the end of life. The current health-care policy debate has focused considerable attention on the unsustainable rate of spending and wide regional variation associated with medical treatments in the last year of life. New initiatives aim to standardize quality and reduce over-utilization at the end of life. We argue, however, that focusing exclusively on medical treatment at the end of life is not likely to lead to effective health-care policy reform or reduce costs. Specifically, end-of-life policy initiatives face the challenges of political feasibility, inaccurate prognostication, and gaps in the existing literature.
Objectives:
With the ultimate aim of improving the quality and efficiency of care, we propose a research and policy agenda guided by a new conceptual framework of factors associated with treatment intensity for patients with serious and complicated medical illness. This model not only expands the population of interest to include all adults with serious illness, but also provides a blueprint for the thorough investigation of the diverse and interconnected determinants of treatment intensity.
Conclusions:
The new conceptual framework presented in this paper can be used to develop future research and policy initiatives designed to improve the quality and efficiency of care for adults with serious illness.
Introduction
Meaningful health-care reform is unlikely, however, if focused exclusively on end-of-life care. The inability to accurately predict life expectancy for individual patients with serious illness, the innate human struggle to avoid death, and modern political realities pose challenges to policies designed to improve end-of-life care. Instead, reform efforts should focus more broadly on all patients with serious and life-limiting illness. Therefore, we propose a new conceptual framework to guide research and policy aimed at enhancing healthcare efficiency and promoting goal-directed care of patients with serious illness.
A Model for Research and Policy Development
Based on our collective clinical experience and knowledge of theory, as well as the empirical literature in palliative care, health services, and economics, we used a deductive process to develop a theoretical model of factors affecting treatment intensity for seriously ill adults (Fig. 1). During model development, we conducted a narrative review of existing literature supporting or refuting each hypothesized relationship. We discussed available evidence and noted areas where data were insufficient and revised the model using this iterative process. Here we present each theoretical construct, summarize the existing scientific evidence, and in Table 1, highlight areas requiring further investigation. This model provides a framework for more inclusive and comprehensive studies by describing the simultaneous interactions and effects of region, physician, patient, and family determinants on treatment intensity.
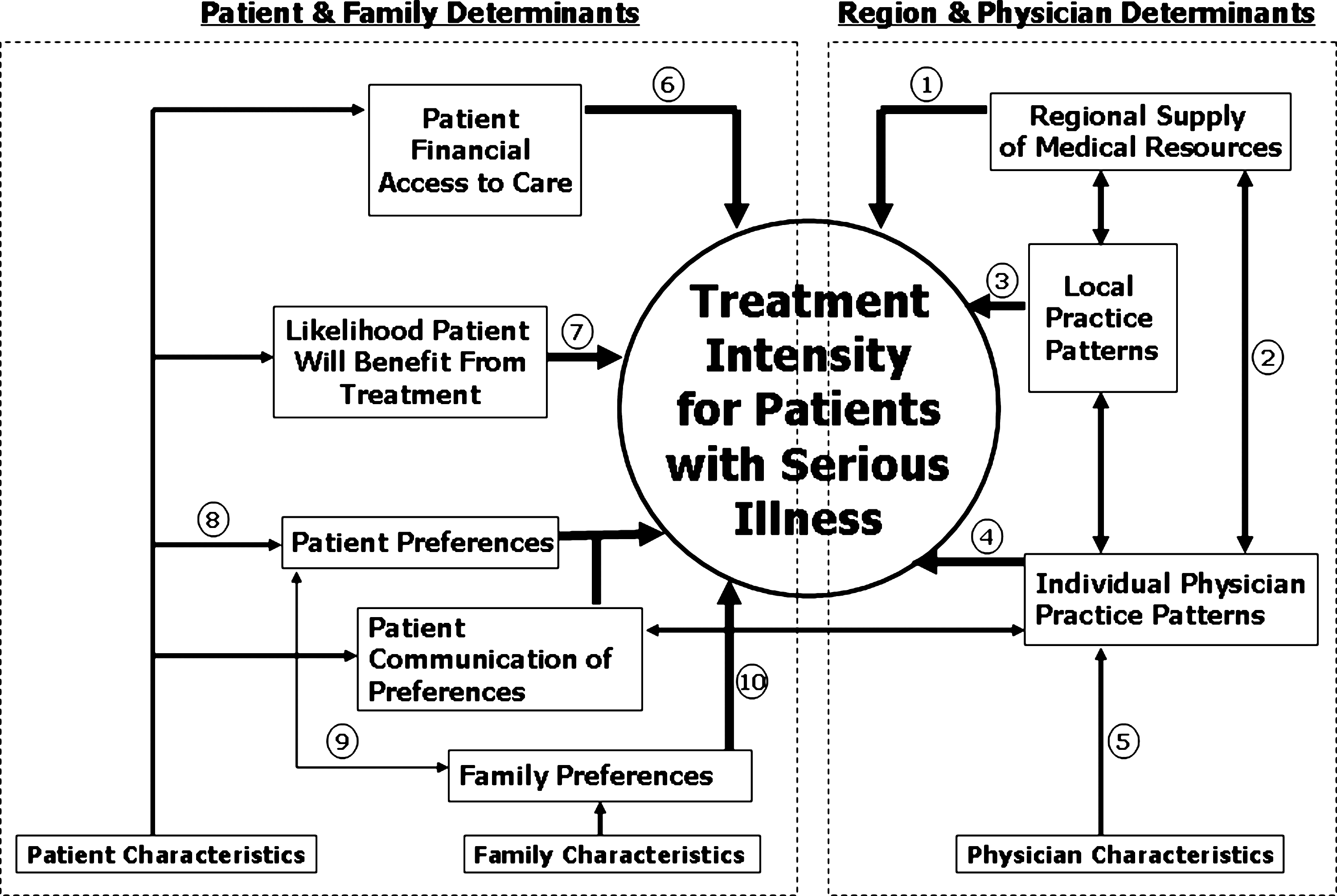
Model of factors affecting treatment intensity for patients with serious illness.
Numbers indicate the area of the model depicted in Fig. 1.
Region and Physician Determinants
Geographic location is highly correlated with treatment intensity.3–5,10 This relationship may be mediated through three distinct but related constructs: regional supply of medical resources, local practice patterns, and individual physician practice patterns. These three constructs may also influence each other through direct or modifying effects. We have depicted these bidirectional relationships in the model with two-headed arrows. Further understanding of these relationships will inform situation-specific interventions and policy and may reveal reform opportunities.
Regional supply of medical resources
Local medical resources (e.g., hospital bed supply, medical specialists per capita) influence treatment intensity. This relationship, referred to as “supply-sensitive care,” is supported by several studies.11–15 For example, patients living in areas with more hospital beds available are more likely to be admitted and die in the hospital. 14 Hospice availability, in contrast, may reduce treatment intensity.12,15 Further investigation is needed to understand this relationship while adjusting for local practice patterns, reimbursement structures, and patient characteristics.
Local practice patterns
Local patterns of care affect treatment intensity; this hypothesis is supported by studies demonstrating an empiric association.10,11,16–23 These patterns may be related to institutional characteristics (e.g., academic affiliation) or availability of specific professional services (e.g., palliative care programs).15,21,24 Local practice patterns can also exist within organizational systems of health care. For example, Medicare Managed Care patients use hospice more frequently than fee-for-service beneficiaries, 25 perhaps due to group practice norms. Further investigation is needed to determine what proportion of observed differences related to local practice patterns is due to local medical “culture” versus reimbursement structures.
Individual physician practice patterns
Individual physicians, even those practicing within the same hospital, may have different practice patterns that influence treatment intensity. These differences may stem from physicians' “intrinsic” characteristics (e.g., race/ethnicity, age, sex, and religion) or “extrinsic” characteristics (e.g., professional specialty, training, years in practice, clinical or personal experiences).26–32 Further research is needed to determine the influence of these characteristics on individual practice patterns.
Patient and Family Determinants
Treatment intensity for patients with serious illness is also affected by patient- and family-related constructs: financial access to care, likelihood of treatment benefit, and patient/family preferences.11,33–38 These theoretical constructs are in turn influenced by specific personal characteristics, including demographic, socioeconomic, medical, functional, and psychosocial factors. The patient- and family-based constructs discussed below provide a theoretical framework for interpreting previously described empiric relationships between patient characteristics and treatment intensity.37–44
Patient financial access to care
We hypothesize that financial characteristics affect treatment intensity. Patients' insurance, benefit design, and ability to pay out-of-pocket for cost-sharing or additional services (i.e., home safety equipment, hired caregivers) influence the care they can access. 45 Healthcare consumption decreases with increased patient cost-sharing, 46 which has important implications for treatment intensity among the seriously ill. Fee-for-service—the predominant reimbursement model—covers most high-intensity services, including doctor visits, hospitalizations, procedures, and surgeries. In contrast, many other services (e.g., home health aide) that might be needed for the delivery of care in accordance with a patient's preference are not commonly covered. We hypothesize that financial constraints may induce a patient to pursue more intensive hospital-based treatments, which are covered, instead of less intensive home-based treatments, which require higher out-of-pocket expense.
Likelihood patient will benefit from treatment
The likelihood that a patient will benefit from life-prolonging treatments also influences treatment intensity. In general, physicians are unable to accurately predict mortality47–49 ; therefore, they are challenged to prospectively distinguish appropriate, high-intensity treatment efforts from inappropriate, overly aggressive treatments.49,50 Furthermore, adults with complicated serious illness, are underrepresented in clinical trials,51–53 making it difficult for clinicians to accurately counsel patients about their likelihood of benefiting from a particular therapy. This uncertainty may also contribute to lower rates of hospice use among patients with conditions for which life expectancy is particularly difficult to estimate, such as dementia or chronic obstructive pulmonary disease.12,54,55
Consideration of treatment benefit is particularly important for patients with complex medical illness. Specialists caring for such patients may inaccurately estimate patients' potential to benefit from intensive treatment because they may not consider the patient's other comorbidities or have failed to coordinate the patients' care with other physicians. Poorly coordinated care, particularly during transitions across sites of care, is thought to be an important driver of high utilization among adults with serious and complex illness.56–58 Other patient characteristics, such as functional status and quality of life, may also influence the assessment of a patient's likelihood to benefit from a given treatment.
Patient preference
Individual patients may prefer treatment focused on extending life, ensuring comfort, or some combination of these goals. Patient characteristics, such as health status and religiosity, have been shown to influence treatment preferences.59–63 Other patient characteristics may influence preferences, including age, sex, education, marital status, social/family support, functional status, quality of life, personal health-care experience, and experience with the death of a loved one. Finally, race/ethnicity have significant relationships with treatment intensity and some evidence suggests this may be mediated by patient preferences or communication of preferences.64–69
Near the end of life, many seriously ill patients are not able to participate in medical decision-making. For such patients, treatment preferences may be conveyed by formal advance directives or advance care planning discussions. The likelihood of these documents or discussions having been completed is influenced by factors such as income, net worth, and location of residence. For example, a living will may be completed as part of estate planning and nursing homes are required to query newly admitted residents about advance directives.
Prior efforts to systematically elicit and communicate patient preferences for treatment intensity have proved insufficient to change care patterns.70–75 Current understanding of the barriers preventing patient preferences from guiding care is incomplete, and this relationship has not been studied while simultaneously adjusting for the region-related determinants of treatment intensity.
Family preferences
Family members frequently act as surrogate decision makers for patients with serious illness; so family preferences may directly impact treatment intensity. The relationship of the primary decision maker to the patient may affect treatment intensity. The family's treatment preferences may also be influenced by culture or filial responsibilities,69,76,77 as well as their own assessment of the patient's quality of life or likelihood to benefit from treatment. Lastly, just as the patients' characteristics may affect their preferences, the surrogates' characteristics and experiences may also influence preferences.
Interactions
Significant interactions between these constructs may exist. For ease of readership, we do not attempt to depict all possible interactions in Fig. 1 but do highlight here the most notable. First, physicians' practice patterns are likely to affect whether patients have communicated preferences for treatment intensity and the extent to which those preferences guide treatment decisions.78–80 Patient characteristics (e.g., age, sex, race, socioeconomic status) may interact with or influence physician practice patterns.81,82 Evidence also indicates possible interactions between patient race and hospital and regional treatment variations.15,30,83,84
Conclusion
Prior research has greatly advanced our understanding of the cost, quality and regional variation in end-of-life care. Yet the current evidence is insufficient to shape effective reform. We have developed a new conceptual framework for determinants of treatment intensity for seriously ill patients as a blueprint for future research and policy. Increased understanding of the relationships among the described factors and their relative impact on treatment intensity will advance efforts to improve healthcare quality and efficiency for adults with serious illness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.