
Abstract
Abstract
Hepatocellular carcinoma (HCC) is a common cause of cancer mortality and morbidity worldwide. Radiation therapy is an underutilized therapy in HCC. A case of a 47-year-old man with locally advanced, chemorefractory HCC with malignant extension into the inferior vena cava and the right atrium, causing cardiac outflow obstruction, which was successfully treated with external beam radiation therapy, is presented. Low-dose radiation therapy is an effective palliative therapy for HCC that is widely available in most developing countries, where HCC is endemic.
Introduction
A case of symptomatic, malignant, intracardiac thrombus from locally advanced HCC successfully treated with external beam radiation therapy is presented.
Case Presentation
A 47-year-old man presented to the emergency department with shortness of breath. He had a computed tomography (CT) of the thorax that revealed malignant HCC thrombus in the inferior vena cava (IVC) extending to the right atrium, with no other cause of dyspnea found.
The patient, who had a history of hepatitis B, was diagnosed 6 years earlier with a 12-cm HCC involving liver segments 8, 7, 6, and 5, with a 7-mm satellite lesion in segment 8. He was treated with an extended right hepatectomy. Two years later, a new 1.9-cm focus of HCC developed in segment 3 and was treated with RFA. Nine months later, a 2.5-cm HCC recurrence adjacent to the RFA area, in segment 2, was retreated with RFA. An isolated metastasis was found in the omentum 4 months later and was resected. Two years later the patient developed intrahepatic recurrence with portal vein and IVC malignant thrombus, as well as diffuse metastatic HCC involving the bones and lung. The patient was then treated with seven cycles of doxorubicin and sorafenib chemotherapy as part of a phase II clinical trial. This was discontinued prior to cycle 8 due to disease progression in the liver and the IVC. He then went on to receive four cycles of bevacizumab in combination with erlotinib. The bevacizumab was discontinued following further tumor progression in the IVC encroaching toward the right atrium as well as progression of the distant metastases in the lungs and bones. The patient continued on erlotinib monotherapy for 6 more months. The erlotinib was discontinued 1 month after completing palliative radiotherapy to the liver and IVC metastases, and no systemic therapy was subsequently offered to him.
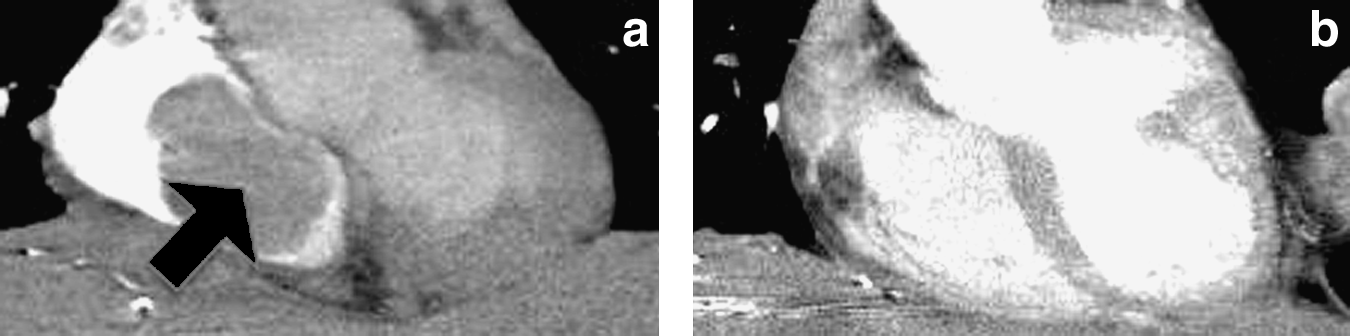
In the emergency department, the CT confirmed a large, enhancing, malignant IVC thrombus extending from the liver into the right atrium, encroaching on the tricuspid valve, measuring 7.0 cm by 5.6 cm and (Fig. 1). The patient was symptomatic with shortness of breath. Blood work demonstrated: ALP 119 U/L, ALT 89 U/L, AST 130 U/L, total bilirubin 20 μmol/L, LDH 714 U/L, platelets 122 bil/L and an international normalized ratio (INR) of 1.18. The patient's most recent AFP was 266. The patient's liver function tests and INR had been gradually worsening over the preceding 6 months. A decision was made to treat this thrombosis with palliative radiotherapy to alleviate his symptoms and prevent further extension of thrombosis.
He received external beam radiotherapy, 2500 cGy in 5 fractions, to the intrahepatic HCC, the IVC and the right atrial malignant thrombus, using a simple two-field, anterior–posterior (AP-PA), arrangement with 18 MV photons (Fig. 2).

Axial image of the radiation treatment plan demonstrating the treatment volume (red), the 2500cGy isodose line (green) and the 2350cGy isodose line (yellow).
One month following radiotherapy the mass in the right atrium had reduced in volume, with continued reduction at 4 months when it measured 3.6 cm by 2.5 cm (Fig. 1). The patient had complete resolution of his shortness of breath 1 month after radiotherapy. The patient had sustained relief of his shortness of breath for the duration of his life. The patient subsequently developed several other site of metastatic HCC, including the scalp, the breast, the neck, and the orbit, which were treated with palliative RT with good relief of symptoms.
Seven months later, due to progressive metastatic extrahepatic disease, the patient was admitted to a palliative care unit where he died.
Discussion
Historically, external beam radiotherapy has had a limited role in the management of HCC. Radiation-induced liver disease (RILD), a syndrome of anicteric ascites, right upper quadrant pain, hepatomegaly, and abnormal liver function tests, has traditionally been a concern limiting the use of external beam radiotherapy to the whole liver. The use of three-dimensional conformal radiotherapy has facilitated the use of safe focal high-dose radiation therapy that has been used to control local HCC, 5 and has led to long-term cure in selected patients. 6 High-dose conformal radiation therapy has also been used to treat local HCCs with portal vein thrombosis. The reported response rates vary from 18% to 79%.7–9 The in-field control rate at 1 year has been reported to be 65%. 10 In another study the local progression-free rates for patients treated with a combination of TACE and radiotherapy at 1, 2, and 3 years was 74%, 57%, and 38%, respectively. 8 Conformal high-dose radiation therapy is predominantly limited to selected centers with advanced equipment, and is not available in most developing countries, where HCC is endemic. However, low-dose radiation therapy is an effective palliative therapy that is widely available. Radiation therapy is well established as an effective therapy to palliate symptoms from bone metastases, brain metastases, and lung metastases. There is far less reported on the ability of low-dose radiation therapy to palliate symptoms from HCC.11,12
In this case report, we have demonstrated how the local symptoms from malignant portal vein and IVC thrombosis from HCC can be effectively palliated with low-dose radiation therapy.
Conclusions
Radiation therapy should be considered in the management of patients with symptomatic portal vein and inferior vena cava thrombosis from HCC.
Footnotes
Author Disclosure Statement
Potential conflict of interest: Dr Dawson has received prior funding from Elekta Oncology Systems and presently has funding from Bayer for clinical research trials, related to liver cancer radiotherapy.