
Abstract
Abstract
Background:
The need for research methods that are suited to evaluate important issues and phenomena in palliative care has established different qualitative research approaches during the last years. This article describes the use and adaptation of a qualitative research methodology in a palliative care setting.
Research process:
The wish for hastened death of terminally ill patients is an important end-of-life issue. Proponents of palliative care have argued that good palliative care would prevent the wish for hastened death. However, this wish is stated by a few patients receiving palliative care, raising a challenging dilemma for patients, relatives and caregivers involved. In order to investigate the motivations of the patients asking for hastened death, we conducted a qualitative study using Grounded theory (GT). This article aims to illustrate the use of a flexible, less burdening qualitative research method and the adaptation of the research process of GT in a palliative care research setting. This is based on experiences and illustrated by examples from the qualitative study on the wish for hastened death in patients receiving palliative care.
Conclusions:
GT allowed a systematic understanding of patients' experiences and attitudes and careful in-depth exploration of this vulnerable population. Conducting a GT study needs high staff resources, a great catchment area for participant recruitment and realistic inclusion and exclusion criteria to allow for theoretical sampling. The use of GT should be facilitated by an experienced researcher familiar with this method because of high methodological requirements and rather complex analysis procedures.
Introduction
In a systematic review of the MEDLINE database with the keywords: “palliative care” or “end-of-life care” and “qualitative research” the authors identified at least 318 publications in the period from 1999 to 2009, with 22 (7%) of them using grounded theory. This specifically underlines the potential value of this particular research approach for the development of new hypotheses and theories on central issues in palliative care. In these research projects grounded theory has been used to explore nurses', patients', or physicians' experiences, for example, with discussing prognosis or advanced care planning, their understanding and management of end-of-life issues such as nutrition or the request for euthanasia.
The wish for hastened death of terminally ill patients is one of the important end-of-life issues and is receiving more and more attention in the palliative care literature. Although this issue raises a dilemma for patients, relatives and caregivers involved, research concentrated mainly on the exploration of quantitative aspects such as the incidence of the wish for hastened death and its stability over time in the context of advanced diseases.2,3
The selection of grounded theory for this study was supported by the discussion in the project group. Our underlying attitude as palliative care experts held the belief that good palliative care would make life worthwhile for patients or at least allow them to bear their suffering. However, we were challenged whether we would be open enough in our research approach to acknowledge if patients would ask for hastened death because they had decided for it after careful deliberation, without any other (hidden) expectations. This confirmed the use of grounded theory, which would not start from preformulated hypotheses, but would focus on the development of a theory as the result of the research.
Grounded theory has the advantage over other qualitative methods to result in an inductively derived theory. This theory should relate to a basic social problem4,5: in our study, the motivations for the wish for hastened death of patients receiving good palliative care.
Hypotheses and conclusions from this project can be used to draft research questions and goals for subsequent investigations on the wish for hastened death. With regard to contents, conclusions on possible adaptations of palliative care settings, treatment options, and caregivers' behavior may lead to interventions. This article concentrates on the use of the methodology and its advantages, challenges, and limitations in a palliative care research process using grounded theory. Examples from the underlying study on the wish for hastened death are used to illustrate the methodology. The theoretical development of the project, its methodological background as well as practical implementation and adaptation are considered.
This article does not present complete data on the arising theory, demographic data on the study population, and general study limitations because of the ongoing evaluation and analysis. This information is being prepared for publication elsewhere.
Research Process with Grounded Theory
Grounded theory (GT) was established by Strauss and Glaser6,7 at the beginning of the 1960s for medical social sciences. GT is a useful research approach focusing on the purpose of inductively generating a theory out of the data material. The generation of a theory is a continuous cyclic analytic process of comparison of data and theoretical sampling.8,9 GT generally offers the opportunity to develop new perspectives beyond existing theories and hypotheses, and for this not only the results and the resulting theory are of interest, but the reflection and analysis of single steps of the whole research process are central. 10 Major interest is the identification of a basic social problem and the generation of theoretical assumptions that are close to reality and fill in the gap between theory and practical implementation.
GT according to Strauss and Corbin was chosen for this study because of its advantage to collect important empirical data in a very open manner on issues not yet well defined. GT produces hypotheses and theoretical frameworks that are not predefined but derived from the original data material. 11 A large number of studies using GT report the resulting theoretical framework and its content categories, but only few reflect the research process discussing advantages and limitations of this method. 12 Nearly all studies report the open exploration of experiences of different populations and different issues as their principal aim.13–15
In this study, a major practical feature was the use of the analysis program MaxQDA 2007 for Windows to support categorization of statements for concept development. Interview transcripts were uploaded in the program, units of text were selected and marked and then allocated to self-generated categories. The software helps the researcher to survey the coding process and easily recover selected sequences of the texts. The program automatically generates a figure showing the category system in detail. Additionally, it offers a feature of generating memos on text passages, which helps to catch the researchers' impressions and highlights from the interviews. This mechanism visualizes structures, similarities, and differences between participants' contexts and perspectives and facilitates the identification of connections and relations between categories.
Recruitment and Performance of the Study
This study was approved by the ethics committee of the University Hospital of the RWTH Aachen University.
From January 2007 until March 2009 team members of the palliative care units in Aachen, Bonn, and Cologne identified patients receiving inpatient treatment who had expressed a wish for hastened death. Once patients had stated such a wish spontaneously, this statement was documented and reported to the investigator if the patient agreed that the information could be communicated to a researcher. Following contact with the researcher and informed consent patients completed the Hospital Anxiety and Depression Scale (HADS), 16 the Mini Mental Status Examination (MMSE), 17 and demographic and clinical data were collected by the Hospice and Palliative Care Evaluation (HOPE).18,19
MMSE had been included in the test battery to exclude cognitive impairment; HADS was used to assess depression as well as anxiety. Both are frequent events in palliative care and the test results may contribute important information to the motivations for the wish to die.
Exclusion criteria were an MMSE sum score below 20, an inadequate knowledge of the German language as well as a physicians' subjective estimate that the patient would not be able to cope with physical or psychological stress.
Information given by the patient during assessment and quantitative test results from the MMSE and HADS were not reported to the palliative care team or used to guide interventions to guarantee the separation of research tasks from the clinical palliative care setting that was described in the written information. All patients had a wish for hastened death but none of them reported to be actively planning to commit suicide so that an acute intervention was not necessary.
Findings
All patients included into the study reached adequate sum scores in the MMSE with a mean value of 29 of 30 points. Among the 12 participants only 3 patients had high positive sum scores on the HADS anxiety scale and 5 on the depression scale. High values in the HADS had not been defined as exclusion criteria, so that no candidate patients were excluded from the study. The assessment with both tests took 7–15 minutes of time and was not reported to be burdensome by the participants. 20 Patients were then interviewed using a semistructured guideline. Main questions were, “How did your ideas and beliefs on life and death change within your disease trajectory,?” “What experiences with physicians let you come to the conclusion, that physicians should offer euthanasia,?” and “What alternative measures may help you to wait for death?” (Table 1).
Inductive Analysis and Theoretical Integration: The Coding Procedure
Trained student assistants performed verbatim transcriptions of the recorded interview material. The program MaxQDA 2007 for Windows was used for data analysis. Descriptive statements from patients were extracted to gain knowledge about predominant processes, changes and turning points in patients' life related to the main research questions (Table 1). These statements were sampled into meaningful units and grouped into descriptive codes. Codes with similar content represent concepts of important topics from the patients' point of view. Concepts were grouped into categories that represent broader or more basic conceptual constructions. Overlapping concepts were redefined and differentiated in a process of constant comparison until no more or different categories or concepts could be emerged. 21 First, working hypotheses about processes and motivations leading to the wish for hastened death were built. They were used to generate a theory that explains the subject of the research (Fig. 2).
The following examples illustrate the analysis procedure from descriptive in vivo codes to concepts and superior categories and theory.
Example for potential motivation for the wish for hastened death
Statements like:
“ … that others are not affected by watching someone else wasting away for 2 month, willing to die and willing to die, but he does not. That is difficult for the family members” “I don't want to burden my wife” “I don't want to get on someone's nerves” and That is somehow a vicious circle. If my wife sees me having a hard time, she is suffering from that. And then, when I see my wife suffering in extreme, and then I am in a bad shape, because after all, it is my fault.”
were grouped as the concept “being a burden to others,” which was summarized together with other concepts to the superior category “family and social networks.” The concluding hypothesis: “The feeling of being a burden to family members and significant others may strengthen the wish for hastened death” was integrated as one aspect into the theory of understanding the motivation of the wish for hastened death.
Example for potential biographic comprehension
Patients' statements like:
“For me a quick death has always been important“, “This is my personality, that I have a quite clear idea of myself” and “The energy that I have always had, the positive (energy), that has made me as a person … but exactly this is getting less and less at the moment”
are grouped as the concept “biography,” which were summarized as one aspect in the superior category “Individual system of norms and values and personal attitudes.” The concluding working hypothesis: “Individual biographic changes and stabilities may facilitate the wish for hastened death” was integrated as another aspect into the theory.
This process of arranging codes, concepts, and categories has been done by two raters who were familiar with the methodology independently. The researchers found consensus on coding in cases of differences. The upcoming hypothesis and theoretical assumptions were further expanded and revised selectively with more interview data being retrieved until saturation of information is reached.
The two presented categories are examples of fundamental parts of the theory which is to be constructed. This theory should elicit and define plausible relationships among sets of concepts. 22
Operational and decisional patterns emerge from these norms and values within the biography. A theoretical conclusion for the illustrated examples might be: being a burden to others as a consequence of biographic changes is not consistent with individual norms and values and personal attitudes. This could be a first hint to explain why the wish for hastened death outlasts successful symptom control. As the theory is still under construction until the evaluation of the interviews is finalized, changes within the hypotheses and theory are possible.
Application of GT
Application of GT in the specific palliative care setting here required adaptation of the methodology throughout the research process. This included changes in the interview schedule and an unusual management of theoretical sampling and data saturation.
The interview guideline was changed after the first four interviews. This is an usual common and necessary adaptation in GT when data collection progresses. 23 All questions that had been asked in these interviews were collected in a common pool and were grouped according to the underlying research question. Two independent raters evaluated the reaction of the patient and selected those questions for the next interviews that seemed to be most comprehensible, best opening up narrative processes and optimally deepening the information. Changes of the interview guideline according to this analysis illustrate theoretical sampling of interview questions.
The two interview parts: “biographic understanding of the wish for hastened death” and “expectations toward caregivers and alternatives to euthanasia” were kept in the interview guideline. They were both broadened by additional and modified questions, others were kept as original. The topic “interaction with family and friends” was raised repeatedly by participants and therefore added as a third topic into the second part of the interview guideline. A few questions were paraphrased by using other interrogatives or different formulations. The research question “What does it mean to you to ask physicians for euthanasia?” was transferred into the second part as rather referring to expectations toward caregivers than to the biographic background (Table 1).
The first four interviews had an average duration of 41 minutes and a range of 31 to 50 minutes. It was decided to add these questions even though this could have extended the interviews and added to the burden of the interviewed patients. However, the following interviews did not take longer with a mean duration of 37 minutes in a range between 23 and 51 minutes. All participants completed the interview interruption or intervals.
Working with GT, researchers usually make use of theoretical sampling to strengthen validity as a fundamental feature of GT. They also check data saturation after each interview to stop patient recruitment if no more information can be gained with additional interviews. In relation to our specific research aim, only a minority of patients fitted the inclusion criteria. From January 2007 until March 2009 only 40 patients from an estimated total of 1200 treated patients in the three participating palliative care units were documented in the screening lists with a wish for hastened death. However, there may have been underreporting of patients, either from lack of communication between patients and staff or related to reluctance from staff to report the wish for hastened death to the study coordinator. Recruiting patients with life-threatening illnesses naturally implies that patients may be too ill to participate even in simple and short studies, unable to provide informed consent or deteriorate quickly and die before they can be included. 24 From the 40 eligible patients in our study only 12 patients were interviewed. (See Fig. 1.)

Flow chart of patient recruitment.
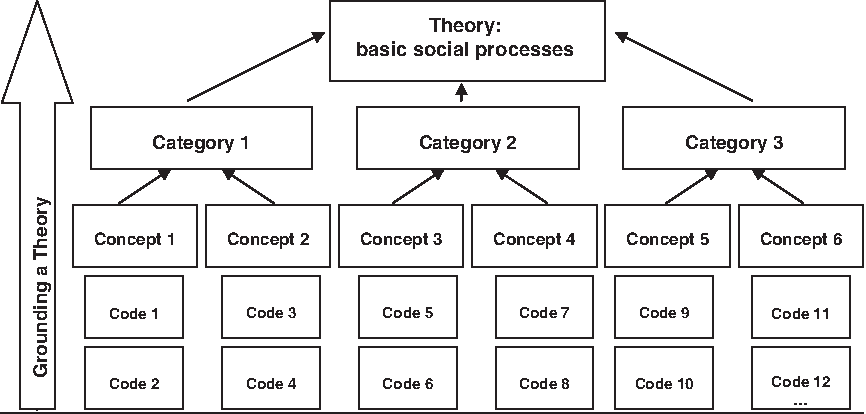
Structure of the coding system of grounded theory.
As the number of patients with a wish for hastened death was rather small and no larger pool of study candidates was available, the researchers had to include all patients with informed consent who were able to participate, and theoretical sampling was not possible.
Lack of theoretical sampling may have put validity of the theory of this project at a risk. However, complete data saturation was reached and the eleventh and twelfth interview did not add new information, so that data evaluation could be stopped according to plan. It is not unusual to reach saturation with a sample of 12 interviews in palliative care research projects with GT.25,26
The set of interviews included two interviews from patients with noncancer diseases, two from outpatients as well as one patient from each of the other two cooperating palliative care units. These patients were different from the first six because of specific characteristics of their disease, care setting, or location of living, and could have added different motivations for the wish to die to the categorization system. 27 However, we decided against any subgrouping of patients in the evaluation, as this would have overemphasized these patient characteristics. In consequence, generalization of the emerging theory has to be discussed critically.
Discussion
Practical and ethical difficulties have to be considered carefully while planning a study in palliative care, as research with severely ill patients and their families puts up specific challenges. Main issues are researchers' and caregivers' concerns about burden and ethical problems, additional demands of ethics committees, keeping methodological accuracy, maintaining the patients' autonomy and protecting them from physical and psychological harm. 28 In this study on the wish for hastened death no concerns were voiced by the ethics committee of the university hospital. However, concern about the burden to patients, the ethical problem of approaching severely ill patients with this topic and the wish to protect patients from harm were discussed intensively in the research group. Therefore, interviews were kept short and interview intermissions or postponement to another day were offered if patients were too weak or tired which was not necessary so far.
Using a qualitative approach required interviews with 20 to 60 minutes of time, and sometimes touched sensible areas in the narrative process. This can be challenged as unethical. However, none of the participants in this study reported additional emotional burden caused by the study participation and most patients had a motivation for participation. These findings are in line with an investigation on the palliative care patients' and caregivers' perceptions of the benefits and problems associated with open interviews in a research setting. 29
Specifically for using GT, the interviewer needs adequate methodical sensibility to find a balance between open questions and guiding process questions. The researcher takes responsibility to enable patients to narrate their story unfettered from the structure of closed questions as well as to evaluate biographic issues in detail by inquiring. There is an inherent difficulty in exploring the patients' world as completely as possible in order to gain the substantial information without interrupting or channeling their narration.
Setting up codes, concepts, and categories in GT requires conceptual clearness. Statements of patients with several meanings have to be allocated consistently to superior concepts and categories, even if these statements are overlapping in content. The differentiation, redefinition and reduction/extension of concepts and categories are fundamental to the peer-reviewed cyclic analysis process. Specifically in GT and in discrimination to other methods such as content analysis, category building is not done according to others empirical data, existing theoretical principles, or hypotheses. This requires a highly neutral and open-minded attitude of the researchers. In addition we used several team meetings, in which experienced researcher from different fields such as theology, public health, palliative care, and ethics reviewed the development of categories. These extensive efforts contributed to keep methodological rigor, which seems to be central to succeed in such an analysis. 30
Some of the methodological problems would have been easier or nonexistent if we had performed the study in patients less ill and less advanced in their disease trajectory. However, the wish for hastened death typically will be expressed in patients with far advanced disease and limited life expectancy. This was confirmed in our study, because we recruited patients with far advanced cancer disease mostly, although we were able to use interviews in patients with noncancer disease and better performance status in the final analysis to confirm the hypotheses in earlier disease stages.
Low recruitment rates impeded the study success even though a full-time researcher was available for the coordination and performance of the study. Reasons for low recruitment have also been reported by a partner project of our study involving the same three study centers. 31 As in our study, main reasons for noninclusion were mainly related to the clinical status of patients with advanced disease, but even GT studies in other medical fields with different patient populations or groups of participants showed similar limitations such as problems with recruitment and low participation rate.32,33
As the number of patients with a wish for hastened death was rather small, theoretical sampling was not possible. These problems were reported in a palliative care context by Sharf et al. 34 and Clover et al. 35 as well. They even had to stop patient recruitment because of time constraints and missing available resources. They were aware of questionable data saturation 34 or reported that “convenience sampling was used rather than theoretical sampling as it was necessary to be resourceful and interview available participants.” 35 These strategies are in contrast to the default use of theoretical sampling, which is recommended in GT. According to the risk of limited validity of data, other researcher in palliative care tried to give rise to more abstract generalizations and trustworthiness of results in case of low recruitment rates by triangulating patients' interviews with professionals' or family members' perspectives.36,37 This was not considered for our study.
Using the qualitative methodology individual priorities and anchor points that moderate the patients' wish for hastened death could be identified in the analysis of the narrations. The methodical approach valued subjective perspectives and allowed in-depth exploration of this vulnerable population and resulted in a theory related to the subjective point of view of the patient. This knowledge will enable the palliative care team to communicate better and respond more adequately to patients. It also can lead to new interventions tailored to the patients' needs.
In summary, we found it challenging to perform a GT study with patients with advanced disease. However, we found the methodology feasible and worthwhile in this setting, gaining rich information from the patients' experiences concerning end-of-life issues, which allowed for the construction of a theory from the data.
Practical implications for the use of GT in palliative care research settings
Planning a GT study in palliative care requires carefully balancing of costs for the patients and benefit for research.
GT should be used in palliative care research projects for investigation of frequent, but less studied phenomena to maximize the chance to apply theoretical sampling.
The study design should allow for access to a broad study population by selecting realistic inclusion and exclusion criteria for this vulnerable population. Expanding the catchment area for recruitment by cooperation with other palliative care units and services improves the chance to conduct a successful study.
Screening, recruitment, and performing the study requires high staff resources as well as a considerable amount of commitment from other staff members. In our study a fulltime researcher was needed for a 2-year period of time in order to include 12 patients in the final evaluation.
The workgroup should include an experienced researcher familiar with GT because of high methodological requirements and rather complex analysis procedures.38,39
Although the wish for hastened death was rare and the recruitment of study participants difficult, GT was applicable and allowed for theory building that would not have been possible with other qualitative methods.
Footnotes
Acknowledgments
This study is supported by a grant of the Deutsche Forschungsgemeinschaft (DFG, 350253). We thank the participating patients, their relatives, and all caregivers from the palliative care units in Aachen, Bonn, and Cologne for supporting the study and dedicating time and energy. We thank all associated researchers for their helpful support, review, and comments to this article.
Author Disclosure Statement
No competing financial interests exist.