
Abstract
Abstract
Objective
: To explore the preferences of competent patients with advanced lung cancer regarding involvement of family and/or others in their medical decision-making, and their future preferences in case of loss of competence.
Methods:
Over 1 year, physicians in 13 hospitals in Flanders, Belgium, recruited patients with initial non-small–cell lung cancer, stage IIIb or IV. The patients were interviewed with a structured questionnaire every 2 months until the fourth interview and every 4 months until the sixth interview.
Results:
At inclusion, 128 patients were interviewed at least once; 13 were interviewed 6 consecutive times. Sixty-nine percent of patients wanted family members to be involved in medical decision-making and this percentage did not change significantly over time. One third of these patients did not achieve this preference. Ninety-four percent of patients wanted family involvement if they lost competence, 23% of these preferring primary physician control over decision-making, 41% shared physician and family control, and 36% primary family control. This degree of preferred family involvement expressed when competent did not change significantly over time at population level, but did at individual level; almost half the patients changed their minds either way at some point during the observation period.
Conclusions:
The majority of patients with lung cancer wanted family involvement in decision-making, and almost all did so in case of future loss of competence. However, as half of the patients changed their minds over time about the degree of family involvement they wanted if they lost competence, physicians should regularly rediscuss a patient's preferences.
Introduction
At the point where the patient is no longer able to make medical decisions, the physician is confronted with a more complex problem: if he wants to respect the patient's preferences about decisions that must be made, their preferences must be clear and the physician may rely on information received from the patient when competent, sometimes in the form of written advance directives, or on the family of the patient, who are assumed to know them well. 2 However, not all medical situations that may arise can be dealt with in advance care planning, nor can it be taken for granted that the family knows the patient's preferences.3,4 Therefore it has been suggested that physicians should not only pay attention to the preferences of the patient in relation to specific medical situations that might arise, but also to how the patient wants medical decisions to be made if he should lose competence, e.g., does the patient wish other people to be involved, who does he wish to be involved and to what degree?5,6
To examine the involvement of family and/or other people in medical decision-making from the perspective of the patient's preferences, we investigated advanced lung cancer patients during the course of their disease. The research questions were:
Who do patients with advanced lung cancer want to involve in medical decision-making while they are competent and are these persons involved? Who do patients with advanced lung cancer want to involve in medical decision-making when they are no longer able to make decisions themselves, and to what degree?
Methods
Consecutive patients with non-small–cell lung cancer (NSCLC), stage IIIb or IV, were recruited by pulmonologists and oncologists at 13 hospitals in Flanders, Belgium, over 1 year. The patients were interviewed by trained interviewers using a structured questionnaire every 2 months until the fourth interview and every 4 months until the sixth interview.
Measurements
Patients were asked whether they wanted others involved in their medical decision-making both while they were competent and if they lose competence in the future, and were asked to select one or more of four possible answers: nurse, family/close friends, no one, other. Patients were also asked whether these people were actually involved. On the assumption of future loss of competence, patients were asked to indicate the extent to which they wanted others involved, choosing one of five possible options representing three categories: a preference for primary physician, shared physician-representative(s) and primary representative(s) control over decision-making. This item is an adaptation of the control preference scale that has been used in other studies.7,8 Quality of life was measured with the Dutch version of the EORTC QLQ-C15-PAL.9,10 The patient interview was pilot-tested and the items were well understood and accepted. Sociodemographic and clinical characteristics were collected upon inclusion in the study.
Ethics
The protocol of the study was approved by the Ethical Review Boards of all the participating hospitals.
Statistical analysis
The characteristics of the patients collected upon inclusion and the quality of life measured during the interviews were tested for association with the involvement preferences with the Fisher's exact test or Mann-Whitney U and entered in multivariate models (random coefficient analysis), together with time (in days since inclusion).11,12
Results
Upon inclusion, 128 patients (68% participation rate) were interviewed for the first time and 13 were interviewed six consecutive times. Figure 1 shows the progression of mortality and loss to follow-up. The characteristics of the patients upon inclusion are reported in Table 1.

Participation in study of patients with non-small–cell lung cancer, stage IIIb or IV.
Three patients reported that they did not have a GP. They were included in the category “Less.”
Comorbidity score using Charlson Index.
Performance status according to ECOG: Eastern Cooperative Oncology Group, ranging from 0 = fully active to 4 = completely disabled.
Estimated by treating physician.
SD, standard deviation; GP, general practioner.
Involvement of others when the patient is competent
At the first interview, 68.8% of patients wanted family to be involved in medical decision-making, 0.0% nurses and 1.6% other; 29.7% wanted no one involved (Fig. 2). These percentages did not change significantly over time until 15 months after inclusion (results of random coefficient analyses), but there were changes at an individual level (not shown in Fig. 2). For example, 17.6% of patients changed their preference for family involvement from not wanting to wanting involvement or vice versa between the first and second interview. Predictors of wanting versus not wanting family involvement were: having a partner (odds ratio [OR]: 4.8, p: 0.027, confidence interval [CI]:1.2–19.5) and having a lower level of physical functioning (OR: 0.98, p: 0.008, CI: 0.96—0.99).
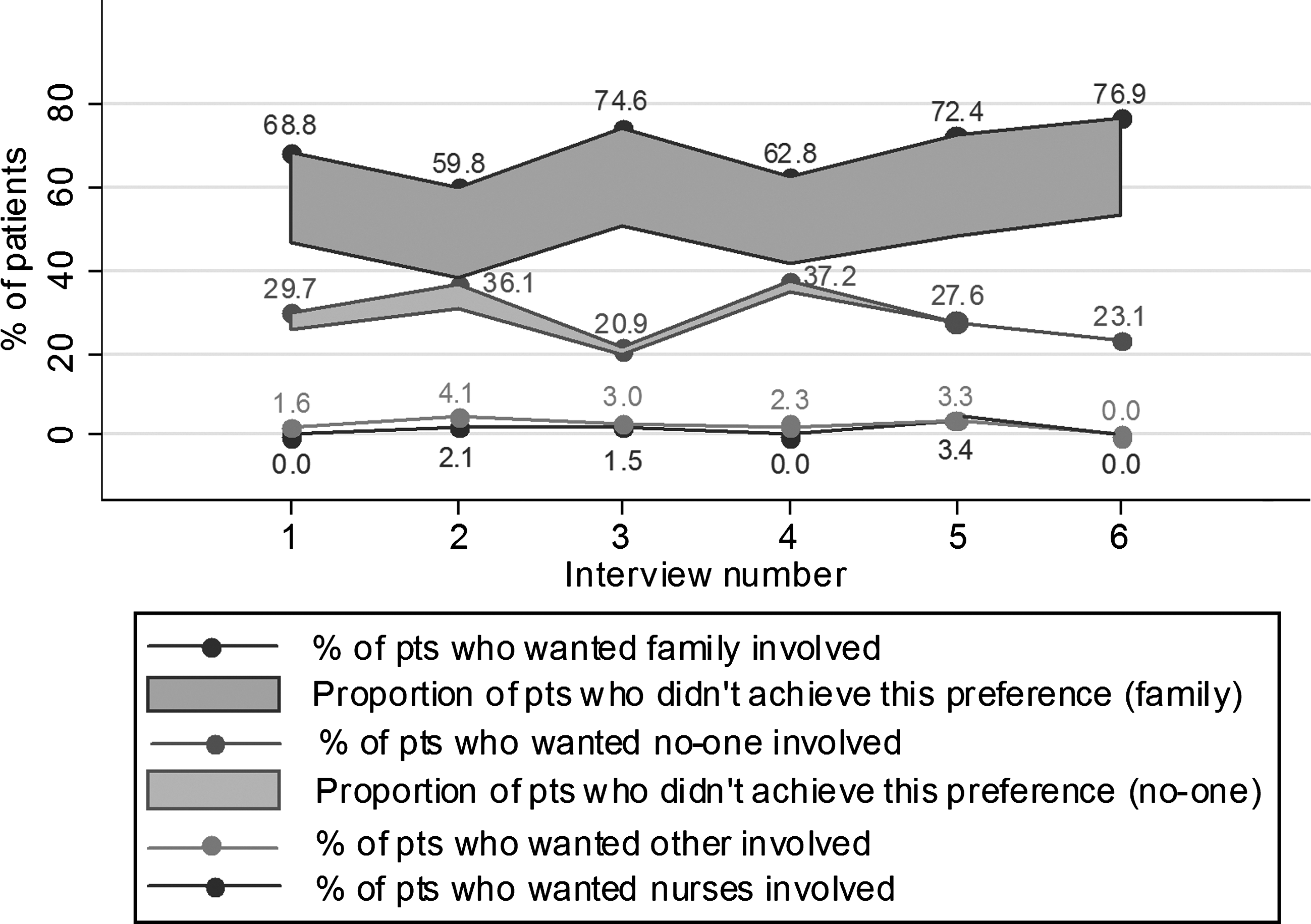
Percentage at interview 1 to 6 of patients with advanced lung cancer who wanted and achieved involvement of others in medical decision-making (while they were competent).
Of the patients who wanted family involvement in decision-making at the first interview, a proportion of 68.2% reported that they had actually achieved this preference and of those who wanted no one involved, 86.8% had achieved it. The achievement rates were similar in subsequent interviews (Fig. 2).
Involvement of others when the patient is incompetent
A total of 93.6% of patients wanted family to be involved in decision-making if they were to become incompetent, 0.8% wanted nurses involved, and 6.4% wanted no one. Of the patients who wanted their family involved at the time of the first interview, 22.6% wanted primary physician control, 40.9% shared physician–family control, and 36.5% wanted primary family control. At population level, the time since inclusion had no significant impact on this degree of preferred involvement (Table 2). There were, however, changes over time at an individual level: 49.4% changed their preferred role for family between the first and second interview and these percentages were similar between the next subsequent interviews (40.0%, 38.1%, 42.9%, and 50.0%). Female patients, those whose emotional functioning was better or improved and those with pain were more likely to want shared physician–family control or primary family control rather than primary physician control over decision-making (Table 2).
Odds ratio resulting from random coefficient analysis.
Time: in days since inclusion (entered as continuous variable).
Scales of the EORTC QLQ-C15-PAL with scores from 0 to 100 (entered as continuous variable).
Discussion
This study succeeded in including 128 patients with advanced lung cancer. Two thirds of the patients wanted family involvement in medical decision-making alongside their own involvement and that of the physician. This is similar to the finding in a study of 50 patients with a malignant disease in Germany. 13 What is new in our study is that this proportion of patients did not change significantly over time after diagnosis.
Of the patients who wanted family involvement, one third reported that they had not achieved this. Reasons for not achieving concordance are not clear, and probably include families who are not able or willing to cooperate or patients who want to avoid burdening their families. 14 A finding of particular interest is that patients with a partner were significantly more likely to want family involvement in decision-making. This suggests that patients without a partner might be at increased risk of having no one to make decisions for them, and thus perhaps need more intensive advance care planning up front.
Practically all patients wanted family involvement if they were to become incompetent and a large majority of these wanted the involvement to be substantial: 41% preferred shared family–physician control, 36% primary family control, and only 23% primary physician control. This is comparable with the finding of a U.S. study in which patients with recent diagnoses of terminal illnesses had to weigh the physician's input against the input of family in decision-making. 15 A possible explanation is that when patients with advanced cancer lose competence, medical decisions are often end-of-life decisions, which are viewed as far more personal than, for example, treatment decisions.
Although the degree of preferred involvement of family in the event of incompetence did not change significantly over time at population level, it did at individual level: almost half of the patients changed their preference at some time between interviews (at intervals of 2 months), toward either more or less family involvement. This finding illustrates the importance of the physician's skills in family communication and implies that physicians should regularly rediscuss a patient's preferred degree of family involvement in the event of loss of competence, or that the physician should tell the patient that a change in preference is not uncommon and can always be communicated to them.16,17
It is noteworthy that although many patients wanted their family involved in decision-making whether they were competent or not, very few wanted nurses involved. This might be in contrast to the findings of studies focusing on actual decision-making in terminal care, where nurses do play a major role. 18
Limitations of the study
There were several limitations. First, caution is needed with generalizing the data beyond the sample: (1) 32% of the eligible patients did not participate and 30% of the patients dropped out during the follow-up; (2) 80% of the patients in our sample were male; and (3) the patients studied were Flemish; culture might have a significant effect on the results. Second, the high loss to follow-up over time also makes it difficult to draw conclusions for the long term, i.e., 1 year or more. Third, patients' preferences for involvement were examined with regard to medical decisions in general and using close-ended questions that did not allow for possible nuances in their answers.
Footnotes
Acknowledgments
This study was funded by the Fund for Scientific Research in Flanders, Belgium (Project No. FWO/AL336), the Research Council of the Vrije Universiteit Brussel (Project No. HOA2 and OZR1218) and the AstraZeneca Foundation. The sponsors had no role in study design, collection, analysis and interpretation of data, in the writing of the report or in the decision to submit the paper for publication.
We thank Christine Pauwels-Delanghe, Eva Michiels MD, and all the patients, caregivers and interviewers who have contributed to this work.
Author Disclosure Statement
No competing financial interests exist.