
Abstract
Abstract
Objective:
The intensive care unit (ICU) experience has been reported to cause adverse health effects in families during and after the ICU stay. The objective of this study was to evaluate health-related quality of life (HRQOL) in relatives of patients 90 days after ICU discharge or death.
Design:
Multicenter observational study.
Setting:
Twenty-one ICUs in France.
Participants:
Among 459 eligible relatives of ICU patients, 284 (62%) were included in the study.
Interventions:
None.
Measurements and Main Results:
During a telephone interview, the SF-36 was completed to assess HRQOL 90 days after ICU discharge or death. The physical component summary score of the SF-36 was normal (89/100 [66–94]) but the mental component summary score showed substantial impairments (emotional role, 67 [50–80]; social functioning, 70 [60–90]; vitality, 60 [45–70]; and mental health, 60 [48–2]). Moreover, 35.9% of relatives were taking anxiolytic or antidepressant drugs, and 8.4% were taking psychotropic agents prescribed since the discharge or death of the patient. Among factors independently associated with a worse mental score, 2 were patient-related (admission for shock or implementation of end-of-life decision), 6 were family-related (older age, female gender, child of the patient, low income, chronic disease, and newly prescribed psychotropic medications), and 1 was related to the ICU experience (perceived conflicts between ICU staff and relatives).
Conclusions:
The SF-36 showed evidence of impaired mental health in relatives of ICU patients 90 days after discharge. Better end-of-life care, psychiatric support after the ICU experience, and better conflict prevention and resolution are potential targets for improvement.
Introduction
Quality of life is a holistic concept that reflects the emotional, social, and physical well-being of an individual, as well as that individual's ability to function in everyday life. Health-related quality of life (HRQOL) is the component of quality of life that depends on diseases and treatments. Measuring HRQOL in family members of ICU patients may contribute to characterize the burden generated by the ICU experience, thereby suggesting means of lightening that burden. In ICU survivors studied 90 days after discharge, the SF-36 scores indicated alterations in quality of life and, furthermore, the prevalence of symptoms of anxiety, depression, and posttraumatic stress were high. 13 However, HRQOL has not been measured in relatives of critically ill patients.
The main objective of this study was to investigate HRQOL in family members of ICU patients 90 days after ICU discharge or death. We looked for factors associated with HRQOL that might suggest effective interventions.
Patients and Methods
This investigation was part of a longitudinal study conducted in 21 medical–surgical ICUs in France in 2003. The protocol and patient characteristics have been described elsewhere. 3 For each patient, we included the family member who was highest in the hierarchy for substitute decision making (spouse; parent/children; other). We obtained informed consent for the 90-day interview near the time of discharge or death of the patient. The ethics committee of the French Society for Critical Care Medicine approved the study.
Patients and families
One family member was included for each patient who spent more than 48 hours in the ICU. We collected the family member characteristics and the variables reported in Tables 1 and 2. Severity of illness at ICU admission was assessed using the Simplified Acute Physiology Score (SAPS) II, which is based on the underlying disease, organ failures, and age and is associated with the mortality rate. 14 Patient health before ICU admission was assessed using the ECOG/WHO performance status scale 15 ranging from 0 (normal activity) to 4 (confined to bed) and all treatment of organ failure occurring in ICU were analyzed. Family members were asked if they consented to a phone interview about possible after-effects of the ICU experience 90 days after patient discharge or death. All phone interviews were conducted by the same sociologist (N.K.B.). The interviewer introduced herself as calling on behalf of the ICU staff as part of a research study on the physical, mental, and emotional well-being of families in relation with their ICU experience. Then, she asked three questions about the effectiveness of the information provided by the ICU staff team during their hospitalization: (1) Was enough time allowed for information? (2) Was the information easy to understand?, and (3) Did the family member feel that the information was complete, in other words that it covered all the points of interest to the family member? In addition, the interviewer asked the family member whether he or she felt in conflict with the ICU staff. For each question, five response options were provided: always, most of the time, from time to time, seldom, never. Information was considered good if answers to questions 1 and 2 and 3 were “always” or “most of the time.” In the statistical analysis, the first two response options were categorized as “yes” and the last three as “no.”
The data are medians (interquartile range).
MCS, mental component summary; ICU, intensive care unit; CoPD, chronic obstructive pulmonary disease; SAPS, Simplified Acute Physiology Score.
The data are medians (interquartile range).
“Consent to research” means that the family accepted to sign an informed consent document for research involving their relative.
MCS, mental component summary; ICU, intensive care unit.
During the same interview, the 36-item version of the Short Form health survey (SF-36) was used to assess the physical and mental components of HRQOL (physical component summary [PCS] and mental component summary [MCS], respectively). The SF-36 was chosen as a reliable instrument that has been used previously in several studies relevant to our topic. 16 The score on each subscale can range from 0 to 100, with higher values indicating better quality of life. Symptoms of anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS). 17
During the same interview, families were asked for psychotropic treatment during or after patient ICU stay. Some recent studies showed a high prevalence of anxiety and depression at the end and months after ICU stay.2,3
Statistical analysis
PCS scores were within normal ranges in our study and we therefore confined the statistical analysis to the MCS scores. Characteristics of patients, families, and interactions between family and ICU workers were analysed. Results are reported as medians (interquartile range) or numbers (%). To investigate associations between MCS scores and characteristics of the patients or relatives, we first performed bivariate analyses, using Mann-Whitney or Kruskal-Wallis tests to compare MCS scores with categorical variables, or to compare MCS beyond or above the median value with continuous variables. Variables yielding p values no greater than 0.20 in the bivariate analyses were entered into a multiple logistic regression model where the dependent variable was an MCS score above the median. All tests were two-sided, and p values smaller than 0.05 were considered significant. Analyses were done using the SAS 9.1 software package (SAS Institute, Cary, NC).
Results
Of the 459 family members in the 21 participating ICUs who were invited to participate in the study, 87 (19%) refused and 88 (19%) were not available for the interview. The remaining 284 (61.4%) family members form the basis for this study. The main characteristics of the family members, ICUs, and patients are summarized in Table 1. ICU mortality was 19.7% (56 patients) and 90-day mortality was 30.9% (88 patients).
Of the 284 family members, 67.6% were women and 48.2% were spouses. Median age was 51 (41–61) years. Psychological support was asked by 8.4% of the relatives during the ICU stay. At the 90-day interview, 102 (35.9%) relatives reported taking anxiolytics or antidepressants and 24 (8.4%) family members took these drugs after the ICU stay. The HADS scores indicated symptoms of anxiety in 49.3% and of depression in 20.1% of the relatives. When asked about the information given to them during the ICU stay, 84.4% of relatives said that the information was clear, 84.8% that the time devoted to providing information was sufficient, and 66.5% that the information was complete. Perceived conflict between ICU team and family concerned 24 (8.4%) relatives.
The 90-day PCS score was within the normal range (89/100 [66–94]) at the 90-day interview. The MCS score was significantly lower than normal. More specifically, scores were 66 (50–80) for emotional role functioning, 70 (60–90) for social role functioning, 60 (45–70) for vitality, and 64.6 (53.2–77.7) for mental health.
Tables 1 and 2 summarize the results of the univariate analysis of factors associated with lower MCS scores. These factors included patient-related characteristics (Fig. 1A) (male gender, poor chronic health status or malignant disease, greater severity of the acute illness [worse SAPS II score], and death in ICU [Fig. 2]) and relative-related characteristics (Fig. 1B) (female gender, being the spouse, having a chronic disease, and having a higher HADS score). There was a significant association between markers for high-quality information and the MCS score.
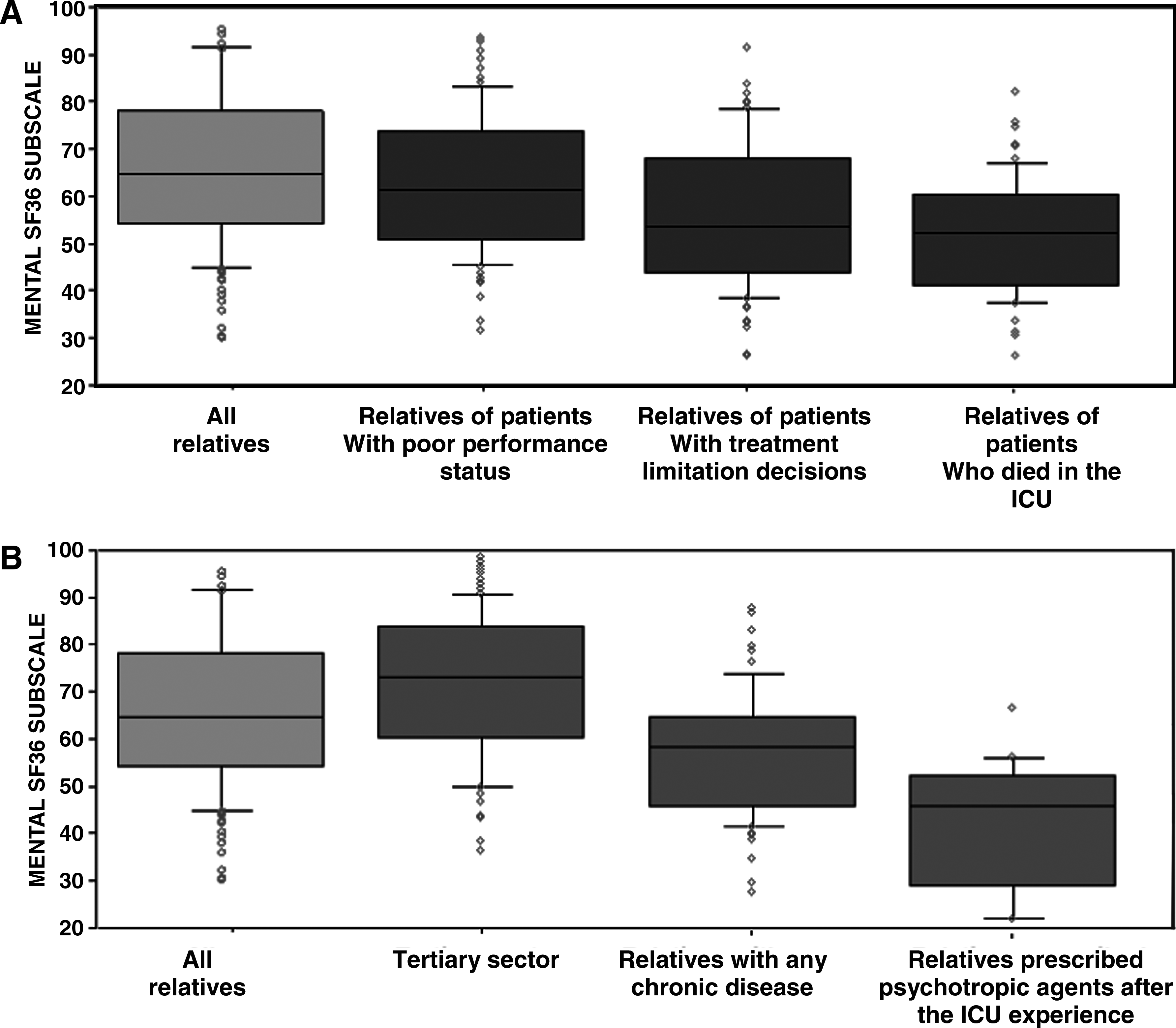
Distribution of the SF-36 mental component summary scores according to characteristics of the patient (
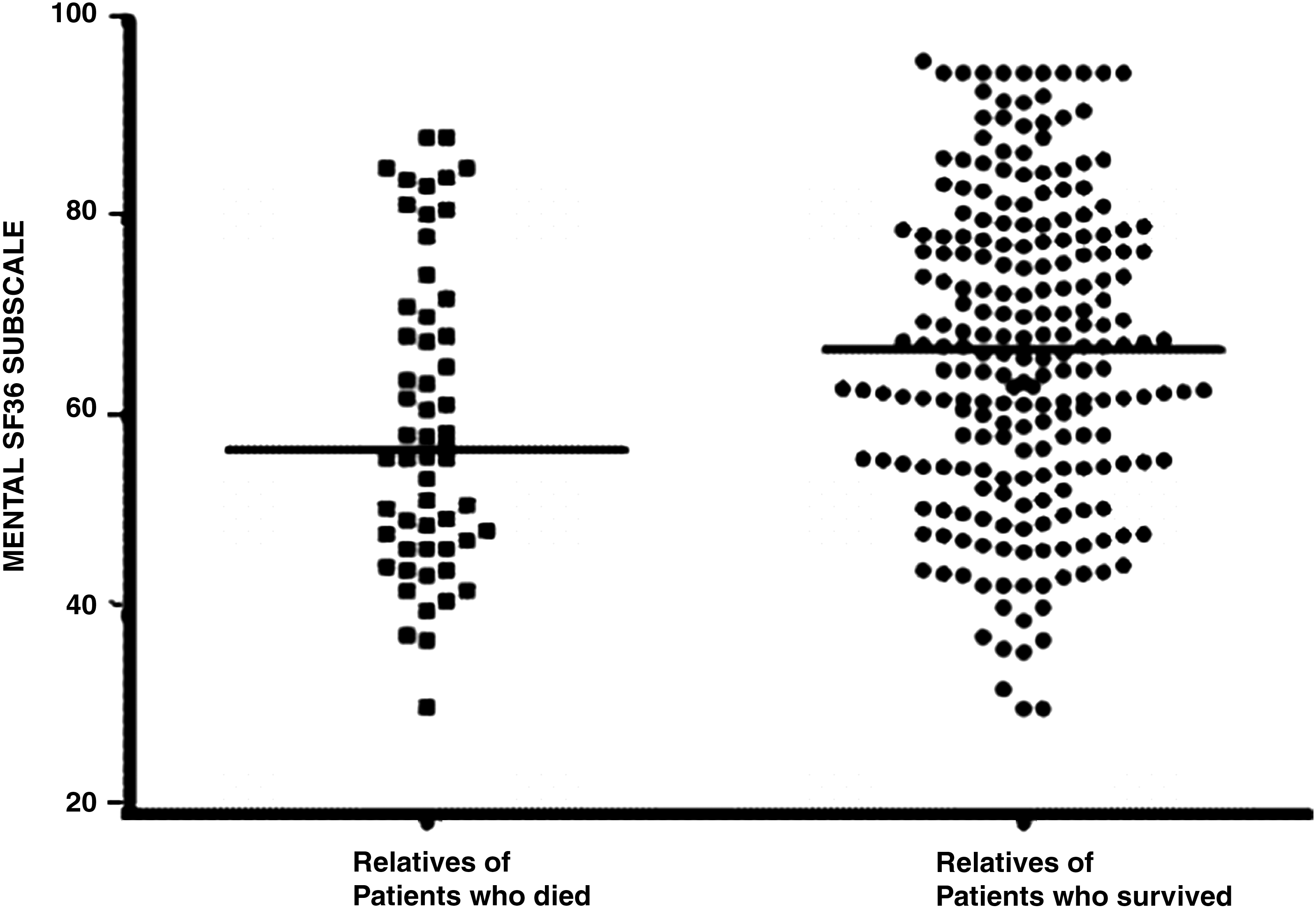
Distribution of the SF-36 mental component summary score according to patient status at ICU discharge. Note the considerable overlap between the two groups of patients. Median values of the mental component summary score differ significantly between relatives of survivors and relatives of non-survivors [66.7 (54.9–78.1) vs. 56.5 (47.1–70.6), p = 0.002].
As reported in Table 3, two patient-related and seven relative-related factors independently predicted having an MCS score above or below the median 90 days after the ICU experience. Relatives of patients who were admitted with shock and/or who received treatment-limitation decisions had worse MCS scores. Lower MCS scores were associated with age younger than 50 years, being a woman, being the child of the patient, earning low income, having a chronic disease, and having been prescribed one or more psychotropic medications since the ICU experience. In addition, relatives who perceived conflicts with the ICU staff had worse MCS scores.
Variables significant in the univariate analysis (p < 0.5) were considered for inclusion in a multivariate logistic regression model, using backward stepwise descending selection. Results are expressed as odds ratio (OR, [95% confidence interval]) and p value of having an MCS score greater than 65.
MCS, mental component summary; OR, odds ratio; CI, confidence interval; ICU, intensive care unit.
Discussion
This study specifically designed to evaluate HRQOL in relatives of ICU patients found significant impairments in mental health, as assessed using the SF-36, 90 days after the ICU experience. Physical health, in contrast, was normal. No previous studies have assessed the impact on HRQOL of having a relative hospitalized in the ICU. Our study is the first to show alterations in HRQOL in this situation. Our findings constitute further evidence that having a loved one in the ICU generates a substantial emotional burden. This study suggests that HRQOL assessments might help to identify relatives who require psychiatric attention.
Among the 10 factors independently associated with worse MCS scores in our study, two suggest possible interventions, namely, treatment-limitation decisions in the patient and perceived conflicts with the ICU staff. Furthermore, in the univariate analysis only, 24-hour visitation and regular nurse–physician meetings were associated with better MCS scores, indicating that practices aimed at improving communication with families probably translate into better family outcomes. Also, we found that worse MCS scores were significantly associated with the way information was provided. Nevertheless In this study comprehension of the information by family was not assessed in this study.
Increased time spent giving information and provision of an information leaflet increased comprehension by family members,18,19 avoiding perceived contradictions, 20 having the staff members directly involved with the patient deliver the information, 21 or giving information more often 6 seems to improve family satisfaction.
Another useful approach may consist in the early identification and treatment of relatives who experience substantial emotional distress after the ICU experience. The high prevalence of symptoms of anxiety and depression in the relatives in our study suggests that the early provision of psychological support and/or psychotropic medications may be in order in some cases. We found an association between worse MCS scores and the use of psychotropic medications after the ICU experience. However, we did not assess the reason for psychotropic medication use (e.g., anxiety, psychiatric disorder, or insomnia). Many studies done immediately after the ICU experience1,21 or 3 to 6 months later3,18,22–24 found high rates of stress symptoms, anxiety symptoms, or psychiatric disorders. In a study of 41 relatives of patients who died in the ICU, 14 (34%) relatives met criteria for at least one major psychiatric disease. 25
We believe that our findings and those from earlier studies indicate an urgent need for creating multidisciplinary collaborative working groups and evaluating the impact of a proactive post-ICU management strategy on the long-term mental health burden in ICU relatives. This strategy could be driven by trained ICU clinicians (nurses and physicians) who would refer family members to psychologists and psychiatrists when symptoms of anxiety, depression, or stress are detected. Evidence that up to one third of ICU-patient relatives may develop mental health disorders after the ICU experience supports this approach. 25 Our results suggest that the SF-36 MCS may be a useful screening tool for identifying ICU-patient relatives who require specialized therapeutic assistance.
Our study has several limitations. First, this study is part of a longitudinal study in which only 61% of included relatives were interviewed. However, in the initial study, the characteristics of interviewed and non-interviewed relatives were not significantly different. Second, we did not obtain baseline HRQOL data. Some relatives, particularly those of chronically ill patients, may have had HRQOL alterations before the ICU admission. However, having the relatives complete the SF-36 at ICU admission might have resulted in spuriously low scores, as ICU admission of a family member may produce severe emotional distress. 2 One way to help determine whether the low post-ICU MCS scores are related to the ICU experience may consist in evaluating post-ICU MCS scores as part of studies of the effects of family-care interventions during the ICU stay. Better ICU scores in intervention-group relatives would indicate that at least part of the emotional burden was related to the ICU experience. Also useful would be an investigation of SF-36 score changes over the year following the ICU experience. Studies of depression and anxiety symptoms showed improvements several months after ICU discharge.2,3
In conclusion, the mental subscale score of the SF-36 is often altered in relatives of ICU patients 90 days after patient discharge or death. Several factors associated with worse mental scores were identified, suggesting interventions for lessening the emotional burden on family members of ICU patients.
Footnotes
Acknowledgments
This study was performed on behalf of the FAMIREA study group. It was supported by grants from the Assistance Publique–Hopitaux de Paris (APHP) and the French Society for Critical Care Medicine.
Author Disclosure Statement
No competing financial interests exist.