
Abstract
Abstract
Background:
Palliative care (PC) programs attempt to improve communication and symptom management, and a consequence has been lower cost of in-hospital death. To date, most research has focused on urban large hospitals. This study reports the clinical and financial impact of a new palliative care service at a 76-bed nonprofit hospital located in rural Virginia, Rappahannock General Hospital (RGH).
Methods:
The RGH PC program started in 2006 with a part-time physician on grant support. We collected the number of consults, physician billing and receipts, and calculated the impact on the hospital's charges for patients treated with concurrent palliative care.
Results:
The program was well accepted clinically with referrals from most of the palliative care physician's colleagues. After the first year of operation, she has about 10 new consults and a total of 45 visits per month. Billings for this year are projected to be $59,070 and her collections are projected to be $29,604 (50%). Hospital charges per patient are reduced about $400 per day, or 25%, after a palliative care consultation, which sums to $80,000 to $130,000 yearly. Referrals to home hospice increased.
Conclusions:
Palliative care by a dedicated practitioner can work in rural areas. The income will be small, but the operational and financial benefits to the hospital can be significant. This is better care at a cost that rural hospitals and practitioners can afford.
Introduction
The Northern Neck region, a 5-county rural farming and seacoast area on the Chesapeake Bay, has one of Virginia's fastest growing elderly populations, with 11,592 of its 50,768 residents (22.8%) over the age of 65 compared to the statewide average of 11.2%. For the entire Northern Neck region, there were 703 deaths in 2003, two times the percentage of deaths statewide. In Lancaster County, one of the largest counties in the Northern Neck, the death rate from malignant cancer (5 persons per 1000 population) is 2 ½ times the state average and the death rate from cerebrovascular disease (stroke) is 1.7 per 1000, (approximately 35 persons in that county), 3 times the state average. In Richmond County, one of the most populous counties in the Northern Neck, the death rate from Alzheimer's is 4.5 times the state average. Due to the increased health needs of this aging population and the inordinate burden of terminal illness, we knew the Northern Neck would benefit from palliative care services.
We started the Rappahannock Palliative Care program in 2006 as a joint project of the Thomas Palliative Care program on the Medical College of Virginia Campus of the Virginia Commonwealth University Health System (VCUHS) and the Rappahannock General Hospital in Kilmarnock, Virginia. The Rappahannock General Hospital is a 76-bed, not-for-profit, community-owned hospital that provides a full range of emergency, medical, surgical, and limited pediatric services. The goal of the joint program was to provide palliative care services to the residents of the rural Northern Neck using an interdisciplinary model of care that offers inpatient, outpatient, nursing home, and home visit services. Our program also educated the community and local health service providers in pain and symptom management and end-of-life care issues.
The palliative care program used existing medical staff, community chaplains, and facilities (Hospital, Northern Neck Free Health Clinic, area nursing homes, and the Massey Cancer Center outreach program). The palliative care physician (J.W.-W.), an internist and former palliative care fellow at VCUHS directed the program with attending physician backup from VCU.
Activities included the following. First, we renovated the existing hospital space (previously an obstetrics unit) into “comfort care suites” (3 private rooms with adjacent rooms for family members, and a conference room for family–physician meetings). Second, we provided inpatient palliative care services using trained nursing, occupational therapy, physical therapy, and social work staff shared with the hospital's medical/surgical units. Third, we provided outpatient palliative care through the Rappahannock General Hospital Cancer Center (a Massey Cancer Center outreach site). A Pain and Symptom Management Clinic was open one half day per week in the outreach center. Fourth, we provided palliative care consults as needed to residents of two nursing home (162 total beds) and home visits for hospice patients to ensure continuity of care. Fifth, we provided palliative care consults at the Northern Neck Free Health Clinic (the only free clinic in the entire Northern Neck). Sixth, we provided training and education about palliative care to the community, local nurses, physicians (54 in the Northern Neck), and chaplains through lectures for physicians, end-of-life-care instruction for nurses, and a workshop for chaplains on bereavement and spiritual counseling at the end of life. Seventh, we partnered with local churches (Kilmarnock Baptist Church, Campbell Memorial Presbyterian, Shiloh Baptist, Irvington Baptist Church, and others) for spiritual care and bereavement counseling. Pastoral care has been provided by local ministers.
This study addresses the impact of the Rappahannock General Hospital and Massey Cancer Center Palliative Care (RGH-PC) program on clinical and financial measures. We hypothesized that Medicare, which was a major insurer in the area, would reimburse the provider costs; that hospital charges would decrease with palliative care consults in a rural facility, and that in-hospital deaths would be replaced with hospice deaths at home as referrals increased.
Methods
The patients, clinical consultations, billing and receipt data are from the palliative care physician's practice management firm. The consult data were first obtained from the palliative care physician's log and billing information, then sent to RGH for matching and capture of the charge detail data. Most (91/102 consults, 89%, for CY2008) were matched in the hospital data and usable for these analyses (the other 11 accounts were not matched or were skilled nursing facility [SNF] admissions, or had incomplete inpatient hospital charge data, or for which the consult fell before the admission date or after the discharge date).
We did not predetermine any values for statistical significance, as when we started the study we were unsure what type of records would be available.
Results
Clinical
For the 91 patients with matched practitioner-hospital data for CY2008, age ranged from 28 to 100, with mean of 77.8 years. Most (88%) had Medicare, 1% had Medicaid, and none were listed as self-pay or indigent. Most admissions were medical (as opposed to surgical) with the following diagnosis-related groups (DRGs) assigned most frequently (accounting for 39% of admissions), as shown in Table 1.
DRGs, diagnosis-related groups; MCC, major clinical complication.
The palliative care services are fully utilized by the RGH oncology program, where they are truly integral to improved supportive care, and utilized by much of rest of the hospital internal medicine staff. The palliative care physician sees approximately 10 new inpatient and outpatient consults a month, and has a total of 45 visits per month (540 yearly).
Impact on physician finances
The program saves money for the hospital through cost avoidance and generates a small income to the practitioner. Her billings for this year will be approximately $59,070 and her collections are estimated from past billings to be $29,604 (50%). These receipts are about the same per consult and visit as at VCUHS, just a much smaller volume. The palliative care physician has modified her work schedule so that she rounds on inpatients, schedules outpatients, and responds to consultations as needed at the hospital and nursing homes. This amounts to approximately 15 hours per week. She sees inpatient consults within 24 hours of the request. Based on Medical Group Management Association and community expectations, the money earned from clinical revenue is inadequate to sustain the service, as discussed below in Discussion section. Without the opportunity to serve as a local hospice medical director, which has synergy with the hospital-based palliative care program, this clinical revenue may not have been sufficient to be sustainable for this physician.
Hopefully, there will be fewer difficulties with Medicare reimbursement for palliative care consultations now that palliative care is a CMS-certified specialty. In January 2006, Medicare changed the rules such that there were no special consultant daily bills allowed. Whoever billed Medicare first for that patient as an internal medicine specialist would be paid, but no other. Since there was no separate Medicare distinction for palliative care, nearly all of the physician's bills were rejected as being a second internal medicine consultation. In the end, most of them were paid by Medicare after lengthy and costly arguments with the carrier, bill by bill. This unexpected and irksome complication occupied much of the time of the PC physician time during the project, and had the side effect of reducing referrals, as internists were reticent to call in another internist. Most claims are paid promptly now but approximately a third still require resubmission after denial.
Impact on hospital finances
The length of the hospital admission (“length of stay” or LOS), is shown in Table 2. The 91 palliative care patients were in the hospital for an average of 5–6 days. The time from admission to palliative care consult averaged 2–3 days. Palliative care programs nationally are reporting 5–12 days on average for this time to referral, with some reporting averages as high as 18 days. 6
RGH, Rappahannock General Hospital; PC, palliative care; LOS, length of stay.
This palliative care program includes a palliative care suite. Twenty-six (29%) of palliative care patients spent at least 1 day in the palliative care suite, for an average of 4 days among those 26 patients. Thirteen (14%) of palliative care patients spent their entire inpatient admission in the palliative care suite. This program serves many frail or gravely ill patients being admitted from the emergency department or physician offices; for these palliative care-appropriate patients, there is zero “delay” from admission to palliative care.
Twenty-three (25%) of palliative care patients had spent at least 1 night in the intensive care unit (ICU) prior to palliative care consultation. In most of these cases, the palliative care consultation appears to have facilitated a transfer to the palliative care suite or other medical-surgical room. Their average LOS in the ICU was 3.1 days (for those 23 patients). Nationally similar results have been reported: palliative care specialists help attending physicians, patients, and families to understand the implications of prognosis and the benefits and burdens of procedures and tests relative to their own values and goals. 7 In many cases this reduces the use of expensive resources such as ICU beds when they are no longer beneficial or the burdens outweigh the possible benefits. From the patients' and families' perspective, the PC specialist is helping them to ensure that their values and goals are driving the kind of hospital care they receive. From the hospitals' and society's perspective, the specialist is helping to ensure that the care provided is evidence-based and cost-effective.
RGH does not have a cost-accounting system so we conducted our financial impact analysis using gross charges as shown in Figure 1 (n = 77). Charges were reduced by about $400 per day, or about 25%. The analysis excludes day of admission and day of discharge so that only “complete” hospital days are included.
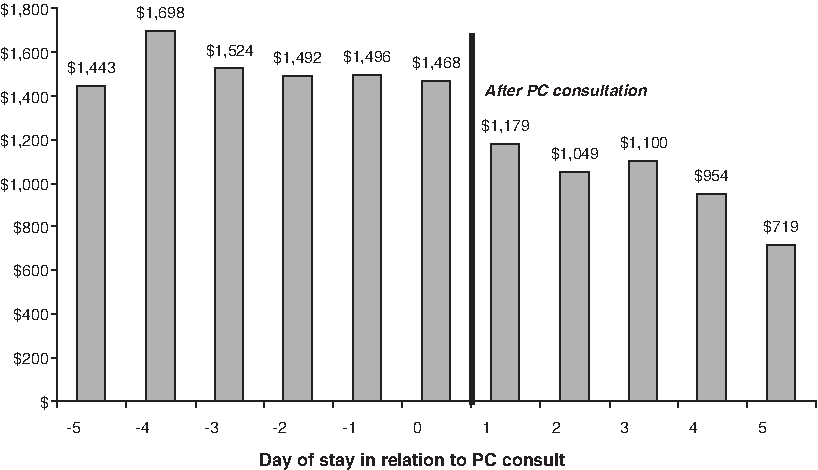
Median charges per day before and after the palliative care consult.
In the days prior to or on the day of PC consult, median charges (inclusive of all aspects of care) were consistently between $1,468 and $1,524 per day. In the 2 days immediately following consult the median charges dropped to between $1,050 and $1,180 per day over the next 2–3 days (the typical LOS following consult). This is between $288 and $474 dollars charged per day less than prior to consult. Extrapolating this to the roughly 100 patients a year seen by the palliative care specialist, with a mean LOS of 2.8 days after consult, we believe this program produces avoidance of between $80,640 and $132,720 in gross charges per year. This is in line with published reports of 25% to 50% savings for end-of-life care hospitalizations involving palliative care consultation.6,8
To determine whether dying patients who did not receive palliative care consultation showed a similar decline in charges per day toward the end of their final hospitalization, we also did a between-patients analysis. We had data for 20 RGH patients who died in-hospital in CY2008, did not receive palliative care consult, were not on the palliative care suite, and had LOS of 4+ days; we compared them to 15 palliative care-consulted deaths from CY2008 which had at least 1 full day in-hospital between consult and death. These other decedents were similar in age (79 years old on average), in the hospital the same number of days (median of 7; mean of 8.45 days), more likely to have ICU days (60% versus 25%). As shown in Figure 2, the usual care patients do not have same decline in intensity and costs per day that palliative care-consulted patients have following consult. Despite the fact that all the patients died, the usual care patients continued with usual costs of care.
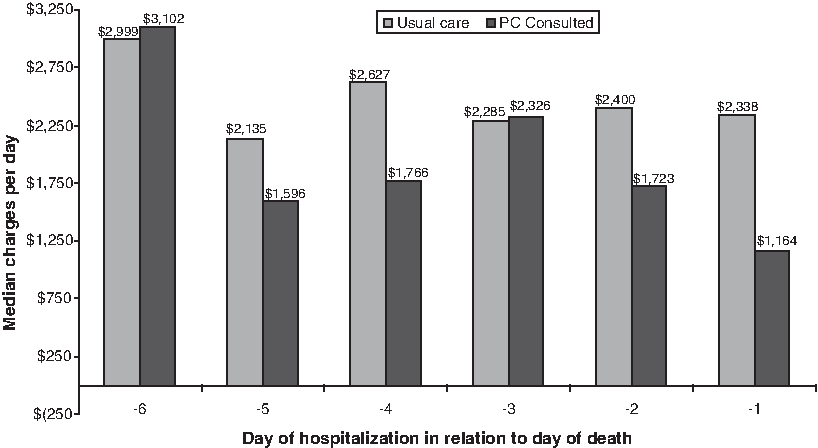
Comparison of patients who died with and without a palliative care consult.
In CY2008, approximately 40% of patients died during the palliative care-identified admission (19%) or were discharged to hospice (20%). Another 40% were discharged to skilled nursing facilities (SNF; 24%) or to home without hospice (15%). The site of discharge changed with the start of the Rural Palliative Care Program: the percentage of patients who were discharged to home hospice increased, as shown in Figure 3, and the in-hospital death rate did not increase.

Referrals to home hospice increased.
Although hard to measure, the program raises community goodwill and provides a special service that distinguishes RGH from competitors, as well as meeting a medical need.
Discussion
Our goal was to pilot a model for rural palliative care that was sustainable to the health system, similar to our goal for the Thomas Palliative Care Unit and the Rural Cancer Outreach Program, since financially sustainability is key to long-term success. The RGH PC program was clinically successful with approximately 10 new consults a month and 500 visits a year. This generated about $30,000 in clinical receipts for the approximately 15 hours per week work by the palliative care physician, or about $100,000 for 50 hours. By comparison, the average palliative care physician received a mean salary of $199,059 ± $39,737 in annual compensation in 2008 (Medical Group Management Association survey of 17 physicians in 9 practices), but rural salaries tend to be 5% lower than urban salaries. 9 The program also generated $80-130,000 savings in reduced hospital charges each year. From the available data, and actions of the hospital, the program is sustainable for the rural hospital. RGH supports the program financially with full support of the Oncology Center nursing salaries and continuing the palliative care program as an integral part of the Oncology Center. In addition, they pay approximately $3,000 for the palliative care physician's malpractice insurance, and cover her billing expense and continuing medical education. For the right person, the salary and support structure is sufficient to continue the work.
The program appears to have changed the patterns of care at the end of life; hospice referrals increased and the in-hospital death rate did not increase. This will be an advantage as hospitals are increasingly compared on mortality rates, and fits with published reports that palliative care units do not worsen in-hospital mortality.10,11 The fact that more than 80% of the patients are surviving their inpatient admission means that referring physicians do not see the PC program solely as a form of end-of-life care. Given the relatively recent development of this program at RGH, this is a testament to the palliative care specialist's ability to correctly frame palliative care as advanced care for the seriously ill patient, not just comfort care at the time of death.
The caveats are that the program success is highly dependent on the expertise (to get consults) and the entrepreneurial spirit of palliative care practitioner (to make ends meet so the program can be sustained financially). This cannot be a full-time job for anyone in a rural area, but must be incorporated into another job, e.g., family practice, hospitalist, etc. As Smyth et al. 12 recently noted in New Zealand, palliative care for the average rural practitioner constituted just 7.3 patients in 12 months; specialist consultation was available and used by 77% of rural practitioner, but in the United States would only help sustain the program if compensated. The success of the program will depend on the drive of the practitioner, willingness for flexible work hours, ability to survive on what most doctors would find a paltry income, and the support of his or her family.
A challenge in evaluating rural hospital-based palliative care programs is that many small hospitals do not have cost-accounting systems that allow for the analysis of direct or variable costs, and the small number of patients precludes complex case control studies. Demonstrating that the impact on hospital charges is in the same direction and degree as published studies of hospital costs, and that patients not consulted by a palliative care service show the same flat or upward trend as “usual care” patients elsewhere, will need to be sufficient in such projects.
Our conclusion is that palliative care in rural communities is better care at a cost that rural hospitals and practitioners can afford, and can be clinically and financially sustainable under some circumstances.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.