
Abstract

Dear Editor:
Palliative consulting teams provide support and care for patients outside palliative care units (PCUs). These interdisciplinary teams provide evaluation, support, or orientation for palliative patients managed in other settings than specialist PCU, or at home. The palliative care teams (PCTs) intervene on requests made by health care professionals (HCPs) and provide specialized palliative care support. (For the purpose of this study, the term “health care professional” (HCP) includes any referring or attending professional (nurse, physician, etc) who has responsibility of the patient and requests a consultation from a palliative care consultant (PCC) or team (PCT), i.e., nurse, physician, etc.) The work of the PCT is therefore to improve patient care and family support through the assistance of HCPs. The goals of PCTs are the same as those of PCUs but the means of achieving them is very different. In addition to the clinical mission, the PCTs aims are pedagogical, supportive, and even probably diplomatic in acute settings where end-of-life issues need to be negotiated. From different palliative care specialists' points of view it is important to diffuse and integrate this approach in various systems of care, to ensure that patients, wherever they are, can benefit from palliative care quality.1–3 In their daily reality, what are the challenges that PCTs must face to respond to their different missions, and especially those of a university hospital? Two clinical vignettes will be used to illustrate the complex issues between HCPs and palliative care consultants (PCCs). We will then reflect on daily PCTs' challenges in an acute tertiary hospital and propose a model that may help enhance communication and PCT's diverse missions.
Clinical Vignettes
A senior resident is caring for a hospitalized 39-year-old woman who has extensive metastatic renal cancer. She suffers from pain, nausea, and vomiting. As a result, chemotherapy cannot be initiated. The patient wishes to be discharged home. The referral addressed to the PCT is: “Which place of care for this patient?” The PCC notices many symptoms and important psychological distress. In addition to the suggestion to remain in the hospital, the medical PCC makes some suggestions to alleviate the patient's multifactorial suffering. The next day, the senior resident asks the PCC to let him continue the care autonomously and asks the PCC to withdraw from the case.
A registered nurse calls the PCT for a 55-year-old patient suffering from pancreatic cancer. She wants to offer some support to the patient who has just been informed about the presence of liver and bone metastases. The nurse PCC asks about the emotional status of the patient. The registered nurse cannot provide any information because of a lack of exploration. When the nurse PCC asks her colleague to meet the patient together, the latter replies: “I prefer that you see the patient alone.”
The Challenges of a PCT
These two vignettes highlight different challenges faced by a palliative care consult team in its daily work with HCPs2–4
:
The integration of palliative care philosophy in a world in which the vision of care is predominantly curative. Responding to palliative care patients' global needs while dealing with those of HCPs.
5
The management of different levels of stress and tension when a consultant arrives in a ward where HCPs feel defeated, unskilled, or helpless (often not verbalized or recognized).6,7 Disagreement among medical and nurse teams about the goal in patient's care. The identification of the HCPs
8
underlying request. The identification of the clients' priority in clinical interventions.
9
The understanding of which collaboration is desired by PCCs and HCPs. The pedagogical mission and palliative care support to HCPs.2,4 The clinical mission and palliative care support to patients and relatives.
Why Develop a Model for PCT Interventions?
To our knowledge, there is no specific training that prepares PCCs for this field. It seems that they learn by having a variety of experiences. Many challenges (see above) concern the relationship developed between PCTs and HCPs. 5 As palliative care professionals take care of the relationship with patients and families using an interdisciplinary approach, is it enough to transfer this knowledge into the job of PCCs when they deal with different interactions? Would they need other tools to guide them? In addition to the recommendations made by some authors it is obvious that a good collaboration between professionals around the patient allows a better quality of care by increasing one's resources, by opening the vision of care, and finally by building a meaningful and common goal of care.8–11 In this sense, transferring palliative care philosophy to other professionals is a constructive advantage for the consultant in the strength of collaboration. Nonetheless, each interaction between PCCs and HCPs does not need the same level of collaboration and differs each time. The Latin roots of the word can offer another complementary point of view, with “consultant” coming from the verb to consult, which means “to deliberate” and “to collaborate,” which means “to work with.” We think that a model of modes of intervention and the use of a common language could allow the consultant to find the best answer during each consultation by supporting the deliberation and collaboration. Indeed, it respects the HCP's request and role. A model may also avoid a PCTs' “role drift,” which could consist with time in replacing one's function in a palliative mission.
The model of practice is the first theoretical part of a pilot study; results of the second part (face validity) will be presented in a later article. Three major modes of interventions emerged of our daily clinical practice following an observation of hundreds of consultations made since 2007 in a tertiary hospital for in and outpatients. Those three modes of intervention (a pure consultation mode; a substitution mode; a partnership mode) represent three major ways of answering a referral request made by another health care professional. Those three modes of intervention generally respect three clinical pathway phases of a consultation: phase 1: the referral, which is the request's reception and the collection of data; phase 2: the clinical assessment, which is the period of the patient's evaluation (it can sometimes be done only on chart)’; and phase 3: the postclinical assessment, which is the period of deliberation or suggestion to the referring HCP and the follow-up decision.
We will first describe those three major modes of intervention in more detail and list their hypothetical benefits and disadvantages from our point of view.
Pure consultation mode
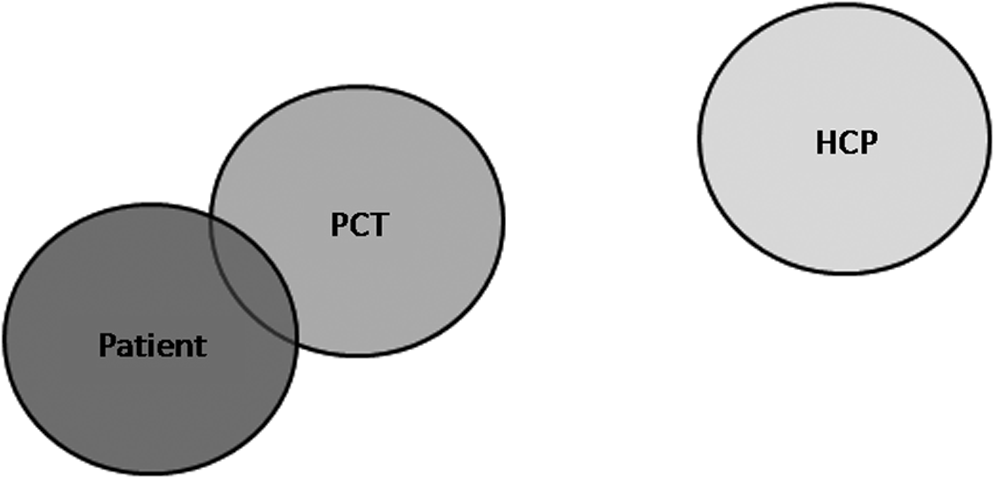
Intervention mode in which a consultant responds to a request from a health care professional (HCP). The goal of care remains totally under HCP's control (see Fig. 1).

Pure consultation mode.
Examples
How do we switch from one opioid to another one? Should we introduce an antibiotic? How do we technically put a subcutaneous hydration? It is usually a specific question concerning a special issue.
For the patient, symptoms identified by the HCP are managed. It reduces the number of professionals; therefore it may generate less confusion and contradiction. However, the patient may not be receiving the best care as other needs might not have been identified.
For the HCP, this interaction may provide him/her with the answer he/she was looking for, but his/her vision of patient's care is not challenged. By asking for help with closed questions, the HCP saves time (helpful if the HCP is in a hurry) and the control of goal of care. As there is a limited exchange between professionals, the opportunities to learn and develop new skills are few.
For the consultant, he/she is recognized as an expert and will have a “up” position in the relationship. This interaction does not take much time and is generally a “one off.” It is difficult for the consultant to evaluate the impact of the proposed interventions. The consultant does not develop a relationship with the patient as he/she has an indirect, minor role with the patient.
Substitution mode
Intervention mode in which the consultant replaces the HCP in the patient's palliative care. The goal of care is totally under the consultant's control (see Fig. 2).
Substitution mode.
Example
The HCP requests that all the palliative care management (bio-psycho-social and nursing issues) is entirely laid in the palliative care consultant's hands.
In this mode of intervention, the patient has the benefit of having the palliative specialist's care. The patient can build a close relationship with the consultant. As the relationship is turned toward the specialist, the patient risks alienating the HCP and not continuing this relationship. The HCP may then feel rejected and begin to disinvest (vicious circle). The patient may not know to whom he/she can ask for help.
In this consultation mode, the HCP is removed from the patient's palliative care, and loses control of it. This can be viewed as a benefit (saves time, greater efficacy) but it can also be a disadvantage. Indeed, the HCP can feel deprived of his/her role and/or feel incompetent, which may lead to a sense of frustration. This mode provides little opportunity to learn about or gain some autonomy in palliative care.
The consultant can feel a sense of satisfaction, and direct validation from the patient. The consultant can assess and respond to all the patient's needs. The consultant has the “control” of the palliative care. The intervention with the patient is regular and based on consultant's appreciation of patient's wishes. The consultant can build a therapeutic relationship with the patient. The relationship between the HCP and the consultant may become distant and create a barrier to further communication.
Shared care mode
Intervention mode in which an HCP and a consultant share point of views and control the goal of care (see Fig. 3).
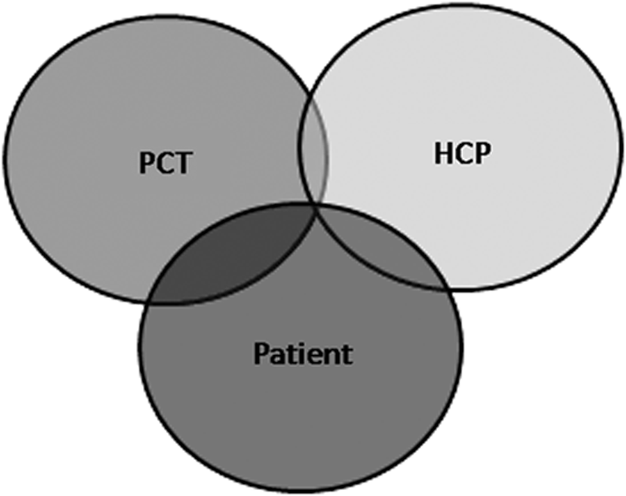
Partnership mode.
Examples
Shared assessment of patient's needs, shared understanding of goals of care, shared meetings, etc.
In this mode of intervention, the patient has the benefit to continue receiving care from the HCP who is himself well supported by the consultant. The patient should feel coherence in the patient-centered care but may be bothered by the presence of another caregiver.
The HCP maintains the relationship with the patient, and collaborates with the consultant to optimize the palliative care. The HCP remains the referring caregiver and shares control with the consultant. The patient is followed by both the HCP, and the HCP is supported by the consultant. The HCP can be educated by the consultant's expertise and, at the same time, informs the consultant of his/her own expertise in his/her field. This interaction takes time for relationships to be developed, which is not always feasible. It also requires a certain amount of maturity to be able to express one's expectations, limits, and needs.
Having relationships with both the HCP and the patient, the consultant may be able to respond to both their needs at the same time. Beside clinical skills, the consultant needs to develop skills in providing support and education. The consultant can support the HCP, however, interventions with the patient must be negotiated between the two partners (collaboration). The consultant can also learn from the HCP. Both the consultant and the HCP may become frustrated to work at each other's rhythm if they are not used to this kind of practice or if they do not know each other.
Back to the Clinical Vignettes
Through the lens of this model, the first clinical vignette corresponds to a pure consultation mode. The resident simply looks for the place of care when he asks the medical PCC to intervene. The first reaction of PCC after stating the place of care as the hospital is to give some advice about symptom management although that was not the obvious need expressed by the resident. A way of dealing with this challenge would have been to first identify the requested mode of intervention then ask the resident: “Although you just asked me to help you deal with the place of care, are you interested in talking about symptom management since the patient is not comfortable enough?” The resident is invited to reconsider his recognized request and is given the possibility to share without being in self-defense.
In the second vignette, we face a request of substitution mode. It would be easy for the nurse PCC to achieve the patient's support by replacing the registered nurse. In this consultancy role, it would however be more appropriate to first focus on the registered nurse, assessing how she sees the situation and what her difficulties are in assisting the patient. The nurse PCC would then evaluate the support she can give and help the registered nurse to overcome her obstacles. If, despite these efforts, the registered nurse does not wish to participate, it would be necessary for the PCT nurse to accept the request by defining a possible shared time between the two nurses, which would be essential after the patient's visit. It would also allow the registered nurse to remain invested in the patient's palliative care.
Hope and Future
Having a reflective practice about the role of mobile PCCs is a first step to improve the care offered to palliative patients by facilitating the collaboration with health care professionals. In this way, the three identified and modeled modes of consultation described in this article can help teams be aware of their position in clinical practice and succeed in their different missions. From our point of view, the shared care mode is an ideal of work for palliative care mobile teams. Nevertheless, it is not always possible to implement a shared care collaboration. The two other modes of intervention seem to be valuable in order to initiate a relationship, but they are called for progressing in a more partnership-like collaboration. It would be unfortunate for mobile palliative care teams to use those “pure consultation” and “substitution” modes of intervention as an institutional or main way of working.
This model can also be an opportunity to share a common language with other consultants. Psychometric phases of a future instrument measuring practice will follow this model. This will allow us to later compare one's practice to another and study the impact on health care professionals and palliative care patients.
Footnotes
Acknowledgments
We are very grateful to the palliative care mobile team of Lausanne and Dr. José Pereira for their input at different moments in the elaboration of this model. Thanks also to Rose-Anna Foley for her assistance in preparing the manuscript.