
Abstract
Abstract
Introduction:
Percutaneous stenting is established in the palliation of malignant biliary obstruction. We examined the indications, success rate, complications, and long-term postoperative course of patients undergoing this procedure.
Methods:
All patients undergoing percutaneous transhepatic cholangiography (PTC) and metal stenting over a 12-month period in a tertiary referral center were studied. Data regarding diagnosis, number and type of procedures, complications, and survival were collected from multidisciplinary case notes and general practitioner records.
Results:
There were 21 patients of median age 70 (mean, 71; range, 54–93), 56.5% (11) had pancreatic cancer and 33% (7) cholangiocarcinoma. The mean number of PTC procedures was 2.43 and mean length of stay in hospital 20.66 days (range, 3–99). Serum bilirubin fell post drainage from 397 to 226 (μmol/L; p < 0.001) on discharge, however, in 19% (4) there was no significant reduction. Complications included cholangitis (19%) and acute pancreatitis (10%). Mortality was high and 9 patients (43%) died within 30 days, of whom 2 died in the hospital (1 from ascending cholangitis and another from pneumonia). The median time between discharge and death was 25 days (mean, 59.1 days) and no patient was alive after 193 days.
Conclusions:
The prognosis following PTC stenting of malignant biliary obstruction is extremely poor despite adequate drainage. The procedure can lead to significant morbidity and a lengthy hospital stay. Patient selection is therefore of paramount importance and an expedient treatment protocol and early return home recommended.
Introduction
PTC biliary drainage involves the cannulation of a peripheral biliary radicle under local anaesthetic. Image guidance is used to manipulate a drain or stent over a guidewire into position.2,3 Metal stents have longer patency than plastic alternatives and result in fewer septic complications, but are more expensive. 3 Many patients require a number of staged procedures to achieve adequate drainage, necessitating a lengthy hospital stay and often resulting in significant morbidity. We reviewed the results of PTC drainage of malignant biliary obstruction in a tertiary referral center with long-term clinical follow-up.
Methods
All patients undergoing PTC and stenting over a 12-month period (2006–2007) in a tertiary referral center (Royal Victoria Hospital, Belfast) were included. The study was conducted retrospectively and involved chart review and communication with the patients' family doctors.
Data regarding diagnosis, number and type of procedures, and complications together with demographics were collected from recorded data at weekly multidisciplinary meeting and from case notes. The charts were reviewed to assess the patients' knowledge of their disease upon admission. General practitioners were contacted regarding the progress of the patient following discharge and survival post discharge calculated. Long-term survival was analyzed on the basis of pathology and compared using the unpaired Student's t test (SPSS version 11, SPSS Inc., Chicago, IL). Statistical significance was taken as p < 0.05.
Results
Demographic details and diagnosis
Twenty-one patients underwent PTC drainage, 11 (52%) were female, ages ranged from 54-93 years (mean 71, median 70).
Many patients (8/21; 38%) were unaware of their diagnosis upon transfer for PTC. Tissue diagnosis was achieved in 13 of 21 (62%), 5 (24%) had pathologically confirmed pancreatic cancer, 4 (19%) had pathologically confirmed cholangiocarcinoma, 4(19%) had biopsied liver metastases (2 from colon, 2 from gastric primary). Two patients (10%) had a diagnosis of cholangiocarcinoma based on history, examination, tumor markers, and imaging and 4 (19%) had a diagnosis of pancreatic cancer based on the same criteria. Two patients had liver metastases from an unknown primary with biliary obstruction.
Clinical progress
The average in-hospital stay was 20.6 days (range, 2–99; median 15) An average of 2.4 procedures was required to achieve biliary drainage (range, 1–7). Internal metal stenting was the final drainage modality in 18 patients (86%), external drainage in 2 (10%) and internal plastic stenting in 1(5%). Serum bilirubin decreased postdrainage from 397 to 226 (μmol/L; p < 0.001; Student's t test) on discharge, however, in 4 (19%) there was no reduction.
Complications
Thirteen (62%) patients suffered a complication prior to their discharge. These included bile leakage (2), acute pancreatitis (2), ascending cholangitis (2), pneumonia (2), bleeding or symptomatic anaemia postprocedure (3), colonic pseudo-obstruction (1), and sepsis of unknown source (1). Two patients died in hospital following their procedure: 1 from pneumonia and 1 from ascending cholangitis. Nine patients (43%) died within 30 days of their procedure.
Long-term survival
The mean time between discharge and death was 59 days (median, 25 days; range, 0–193). No patient was alive after 193 days. The 30 day mortality was 43%. Survival statistics are presented in Table 1 and Kaplan-Meier mortality curve is demonstrated in Figure 1. There was no difference demonstrated in survival between those with pancreatic cancer or cholangiocarcinoma (p = 0.667). There was also no significant difference in survival between those with pancreatic cancer or cholangiocarcinoma compared to those with biliary obstruction secondary to liver metastases (p = 0.864). Patients in whom the bilirubin failed to decrease postdrainage procedure had a mean survival of 19 days (range, 5–46) postdischarge. Patients in whom bilirubin had a significant decrease (>30%) had a mean survival post discharge of 58.2 days (range, 0–192) although this difference was not significant (p = 0.29).
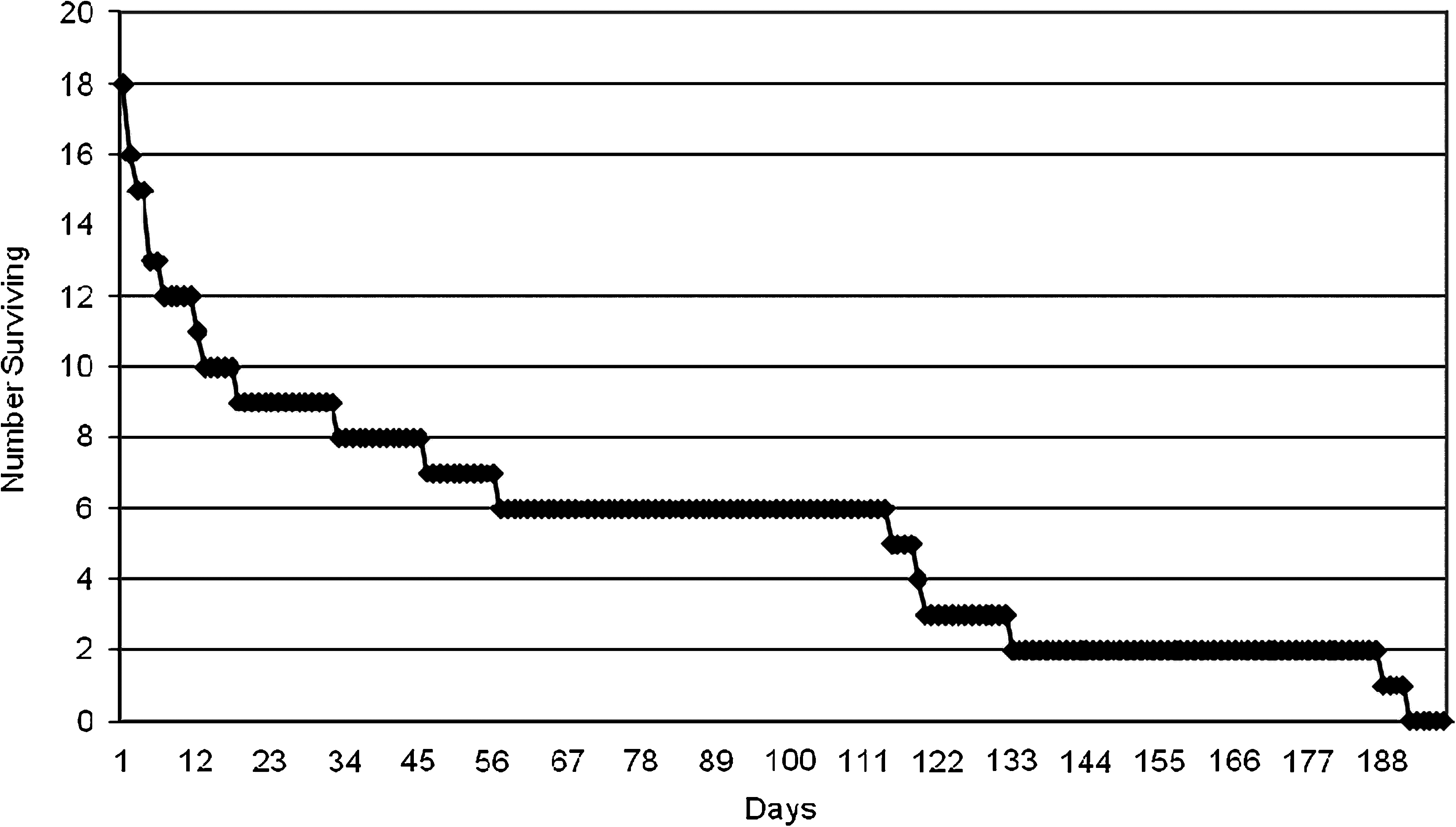
Kaplan-Meier mortality curve.
Discussion
Survival of patients with malignant biliary obstruction unsuitable for surgical resection is poor.3–5 Pancreatic cancer has a 1-year mortality of over 80% and cholangiocarcinoma a 3 year mortality of 90%. 3 Biliary obstruction leads to cholangitis, pruritis, liver failure and malabsorption. Relief of biliary obstruction by stenting attempts to palliate these symptoms and potentially prolong life. 6
Compared to plastic, metal stents reduce the frequency of complications, remain patent for longer but are more expensive. 5 A Cochrane Review concluded that when considering endoscopically placed metal stents that they should be used when the estimated life expectancy was greater than 3–6 months. 3 When considering PTC, there is often debate as to whether unilateral or bilateral drainage is required for patients with hilar obstruction. There is evidence that unilateral drainage is sufficient in the absence of sepsis.5,6
The patients in our study had biliary obstruction secondary to either pancreatic cancer, cholangiocarcinoma or from liver/hilar metastases from other primaries. We did not demonstrate a better outcome in those patients with cholangiocarcinoma. Survival postdischarge from hospital was short and 30-day mortality was high (43%). This is contrasted to the long inpatient stay experienced. Multiple procedures were often necessary to achieve adequate drainage and many patients suffered complications. This study was retrospective and limited to patients referred to a single tertiary referral center over a 1-year period. The accuracy of our results depended on the quality of multidisciplinary note keeping and general practitioner records.
The small prospective studies that measure quality of life in this cohort of patients have yielded conflicting results. Robson et al. 7 reported that PTC drainage produced no improvement in quality of life at 4 weeks. However Saluja et al. 8 reported that PTC drainage in gallbladder carcinoma was significantly more effective than endoscopic drainage, resulting in an improved quality of life and fewer septic episodes.
The presented data aim to facilitate an informed discussion between patients, caregivers, and clinicians prior to proceeding with PTC. Given the palliative intent of the biliary decompression, we recognise the importance of expediency in obtaining biliary decompression and early return home with early involvement of community palliative care services.
Conclusion
The prognosis following PTC stenting of malignant biliary obstruction is poor despite adequate drainage. The procedure aims to reduce symptoms but can lead to significant morbidity and a lengthy hospital stay. It is the clinician's responsibility to ensure patients and families are well versed regarding the risks and benefits of PTC decompression so that expectations are realistic and informed decisions made. The early involvement of palliative care services in this group of patients is advocated.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.