
Abstract
Abstract
Introduction:
This is the first case study to report on using stereotactic body radiotherapy as an alternative and novel treatment modality for embolization to reduce the risk of operative bleeding for a metastatic renal cell tumor.
Case presentation
: A 58-year-old woman presented with an asymptomatic large 7-cm tumor on the parieto-occipital vertex of the skull. Given the location of this lesion along with its vascular histology, it was a challenge to provide safe and effective treatment using conventional management strategies.
Conclusion:
We report on a rare presentation of a metastatic renal cell cancer and the use of stereotactic body radiotherapy as an innovative radiation approach to deliver high-dose radiation safely to control this large aggressive and vascular metastasis. The success of this management strategy allowed for minimal intraoperative blood loss, and the patient continues with local control 1-year posttreatment.
Introduction
Case History
A 58-year-old woman with good performance status was referred to the Rapid Response Radiotherapy Program cancer clinic in Toronto, Canada, in March 2009 for a radiotherapy consultation regarding a large 7-cm protuberant asymptomatic mass in the parieto-occipital aspect of her cranium (Fig. 1). Her history begins approximately 1 year prior to presentation when she hit her head against a cupboard resulting in a small bump that gradually increased in size. A computed tomography (CT) scan and magnetic resonance imaging (MRI) scan of the head revealed a 7.1 × 6.8 cm vascular tumor centered at the skull vertex associated subcutaneous infiltration, and mass effect on the underlying brain (Fig. 2). A large renal mass and presumed metastatic lesions to the liver and bone were found on subsequent staging CT scans.
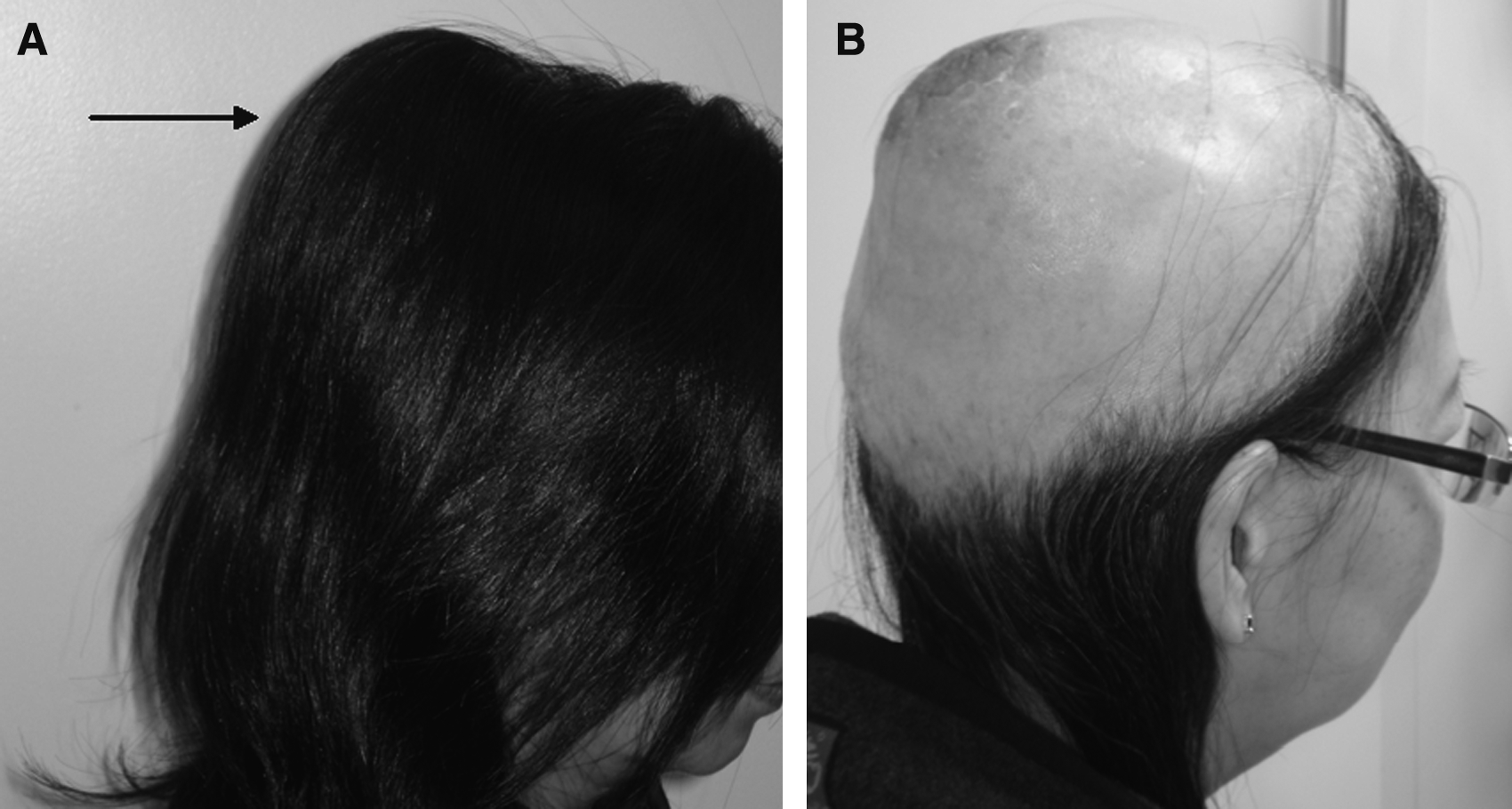
Seven-centimeter skull lesion involving the parieto-occipital region before and after stereotactic radiotherapy treatment. (
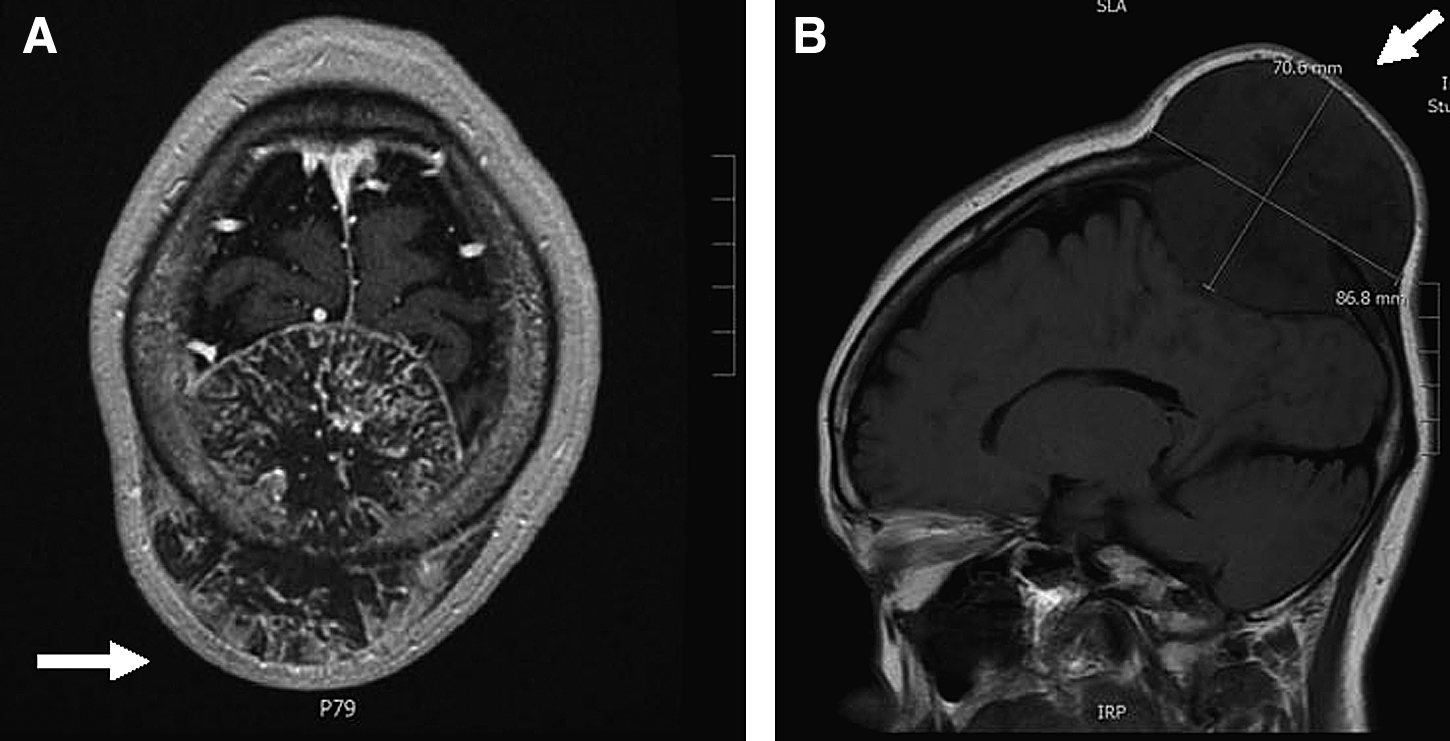
Magnetic resonance imaging at time of presentation. (
To obtain a pathologic diagnosis, an excisional biopsy of the skull lesion was attempted; however, excessive bleeding complicated the procedure and confirmed the highly vascular nature of the metastasis. As a result, only a small tissue sample was obtained sufficient to diagnose a spindle cell malignant tumor consistent with mRCC. The neurosurgeon deemed it to be unresectable due to an excessive risk of bleeding associated with a gross total resection. The patient was referred to the radiation oncology service the following week, and their decision was to treat using SBRT. A hypo-fractionated course of radiation prescribing 35 Gy in 5 fractions was delivered to the tumor with the goal of stopping tumor growth and potentially reducing the risk of bleeding at the time of resection, which was contingent upon tumor response. A conformal dose distribution maximized radiation coverage of the primary tumor, while sparing the underlying normal brain tissue as shown in Figure 3.

Stereotactic body radiation treatment plan of the skull lesion demonstrating a conformal dose of 35 Gy around the tumor alone.
Immediately after completion of treatment, the patient experienced a grade 3 skin erythema and alopecia reaction. The skin toxicity resolved within a few weeks following SBRT. Four weeks later, the tumor mass was clinically smaller in size and was proven to be controlled. The patient was taken to surgery a week later (5 weeks post-SBRT), and under general anesthetic a gross total posterior craniotomy was performed. No significant bleeding was observed during surgery, and the tumor was grossly necrotic. Histologically, the tumor was found to be largely avascular and necrotic (Fig. 4). Four weeks postsurgery she was started on Sutent therapy, and at the time of this report continues therapy (for 1 year) without clinical or radiograpghic recurrence (Fig. 5).

Extensive tumor necrosis and residual viable tissue is visualized focally (arrows) on hematoxylin and eosin staining postradiation treatment.

Magnetic resonance imaging illustrating no recurrence 1 year after treatment.
Discussion
Malignant renal cell carcinoma accounts for 3% of all adult malignancies.1,2 Only 1% of mRCC cases manifests to the head and neck. 3 Currently there are only two reported cases of mRCC presenting as a cranial metastasis.3,4 Some mRCC lesions are declared unsafe to treat with surgery alone due to their highly vascular nature, and typically a preoperative procedure such as embolization is frequently performed to reduce the risk of bleeding. In this case, the tumor was located in the midline over the sagittal sinus and located in the feeding territory of multiple dural branches including bilateral middle meningeal and vertebral arteries. Extensive transgression of tumor under scalp also raised the possibility of multiple scalp feeders. Therefore, embolization was not felt to be effective in substantially reducing the risk of hemorrhage in this case.
We report a rare presentation of mRCC and, moreover, the use of SBRT as an innovative radiation approach delivering high-dose radiation safely with the aim of controlling this large aggressive and vascular metastasis. SBRT was successful and rendered within 5 weeks. The subsequent surgery was associated with minimal intraoperative blood loss. Therefore, based on this case study we propose the potential for SBRT is an alternative to embolization of vascular mRCC, in particular for locations where embolization is not feasible. However, this treatment option should first be tested for safety and feasibility in the context of a randomized clinical trial.
Retrospective clinical studies have reported on the idea of radioresistance in mRCC, and the use of a higher total radiation dose over a protracted period of time to overcome the assumed radioresistance of mRCC. 5 Often, clinicians will prescribe conventionally delivered radiation treatments of 10 to 25 daily fractions (2–5 weeks) to a total dose of 30 to 50 Gy (1.8–3.0 Gy/day fraction sizes). This is often prescribed for pain and symptom control, as opposed to lower palliative doses of 8 Gy in a single fraction or 20 Gy in fractions. 5 The recent emergence of SBRT has challenged the practice of traditional fractionations schemes for patients with metastatic radioresistant disease by delivering a high biologically effective dose to a tumor in 1 to 5 fractions. 6 Generally the dose per fraction is greater than 5 Gy. Fundamentally, SBRT aims to deliver a curative dose to small metastatic lesions over 5 days. Longer courses of radiation are not optimal for a patient that needs to start palliative systemic therapy treatment as soon as possible to control the cancer. High rates of local tumor control have been reported for patients with mRCC to the spine.6–8 However, there is limited evidence to guide the use of SBRT to other bony metastases.
There may be additional benefits of SBRT in vascular tumors, given the potential for an enhanced biological effect specifically on the tumor vasculature. Tumor endothelial cells are more sensitive to large dose per fraction radiotherapy as compared to conventional fractionation,9,10 which may explain the profound avascular response we observed post-SBRT. In this case the tumor vasculature was shut down within 5 weeks to allow minimal bleeding at surgical resection. This suggests that high-dose SBRT could be a viable alternative to procedures such as preoperative embolization.
Conclusion
We report on the success of the use of upfront SBRT in the treatment of a large vascular skull mRCC, and in rendering a highly vascular tumor essentially avascular within 1 month of treatment. We propose SBRT as a potential alternative to preoperative embolization to reduce the risk of operative blood loss
Author Disclosure Statement
No competing financial interests exist.