
Abstract
Abstract
Although religiousness may, to a certain extent, be expected to alleviate emotional suffering in the last week of life, some religious beliefs might also provoke emotional distress. For the current study, after-death interviews with proxy respondents of deceased sample members of the Longitudinal Aging Study Amsterdam provided information on depressive mood and anxiety in the last week of life, as well as on the presence of a sense of peace at the approaching end of life. Proxy respondents also were asked about serious physical symptoms in the last week of life of the respondent, the respondent's cognitive decline, and their estimate of the salience of religion for the sample member. Other characteristics were derived from the last interviews with the sample members when still alive: depressive symptoms, chronic diseases, religious affiliation, church attendance, belief in Heaven, belief in Hell, and salience of religion. None of the characteristics of religiousness was significantly associated with depressive mood or anxiety, as estimated by the proxy respondent. A sense of peace, however, was predicted by higher church attendance, belief in Hell (among church-members), and the proxy's estimate of the salience of religion. It can be concluded that religiousness did not affect depressive mood or anxiety in the last week of life in the current sample. It is possible that religiousness supports a sense of peace, which may be a more-existential facet of mood and is discussed as relevant in the last phase of life and in palliative care.
Introduction
Following Pargament's concise, but inclusive, definition of religion as a search for significance in ways related to the sacred, 4 an important aspect of religion is its intended potential to assist people to face, manage, and accept the inevitable facts of existence, such as suffering and death. The Netherlands represent a highly secularised country, but the older generation has still grown up in a society in which religious traditions had a prominent role, and many older people still endorse religious beliefs. 5 Detailed figures from a study among older US citizens showed that religion remains important for older adults: Rates of church attendance only declined in the last half year of life, while levels of subjective religiousness were stable or increased. 6
The last phase of life may follow different trajectories, such as with a gradual or rapid physical decline, and the mental demands will vary along the different types of illness. The last phase of life is characterised by inevitable adjustments for many older adults. There is a large need for informal and formal care, and many have to face a transfer to a different living environment and may help in coping with that change. 7
How do individuals respond emotionally to these circumstances? The stages of grief, as identified by Kübler Ross, may still offer a point of departure in the psychology of the last phase of life.8,9 Nevertheless, Maciejewski and colleagues provided evidence that the stages could be better considered as states that can co-occur. 10 As Prigerson and Maciejewski summarised, denial, anger, bargaining, and depression represent a constellation of highly inter-correlated grief indicators. 11 When grief falls, acceptance of the loss rises. For empirical studies with relevance in a period of loss, it is therefore important to assess grief or distress, but also acceptance or inner peace.
Several studies among terminally ill patients have shown associations between “spiritual well-being” and lower levels of psychological distress. 12 –17 Some content overlap may, however, occur between spiritual well-being – with items on the meaning of life, inner peace, and the supportive role of religion in coping – and emotional well-being (or its reverse, psychological distress). Therefore, some studies included statistical adjustment for depressive symptoms.12,13 It is difficult to say which aspects of religiousness and spirituality specifically determine the association with psychological distress in the terminally ill because the measure of spiritual well-being combines several aspects. One study included the belief in a hereafter as a distinct variable, which was associated with lower levels of hopelessness, but not with feelings of anxiety or depression. 15 In a palliative care study, a significant association with the presence of depression or anxiety disorder was found for church-attendance, but not for religious affiliation, prayer, or subjective religiosity. 18
The current, population-based study aims to explore whether aspects of religiousness affect mood in the last week of life, as has been estimated by surviving relatives of deceased sample members of the Longitudinal Aging Study Amsterdam (LASA). 19 Information on religiousness was also obtained from LASA respondents when they had been interviewed during the patients' lifetimes about several aspects of religious life, as well as about depressive symptoms.
Methods
Sample
The present study is part of LASA, an ongoing interdisciplinary study on predictors and consequences of changes in autonomy and well-being in the aging population. The LASA cohort is based on a nationwide random sample of older adults between the ages of 55 and 85, stratified for age, sex, and expected mortality five years into the study. Registries of 11 municipalities in areas in the West (mostly secularized, including Amsterdam), Northeast (predominantly Protestant), and South (predominantly Roman Catholic) of the Netherlands provided the sampling frame.20,21
The realized number of respondents in the LASA baseline interview cycle in 1992/1993 amounted to 3,107. Respondents were interviewed in their homes by intensively supervised interviewers. Three years later, in 1995–1996, all respondents were approached for the T2 interview cycle. The participation rates and numbers of decedent respondents are shown in Figure 1. Between T2 and T3 (1998–1999), 342 respondents died. The database of LASA contains contact information about two people close to the sample member, such as the partner, a child, sibling, or other person who had had close contact. Wherever possible, one proxy respondent was selected who had been involved in the last three months of the sample member's life, and who was willing and able to participate. The proxy respondent was approached with a letter and information, and then by a telephone call, to make an appointment for the interview, which was held in the home of the proxy respondent. This research method is known in the literature as “retrospective/afterdeath approach” or “proxy-interview.” 22 The number of proxy respondents amounted to 277 – mainly children (50%) and spouses (33%) of the sample members.
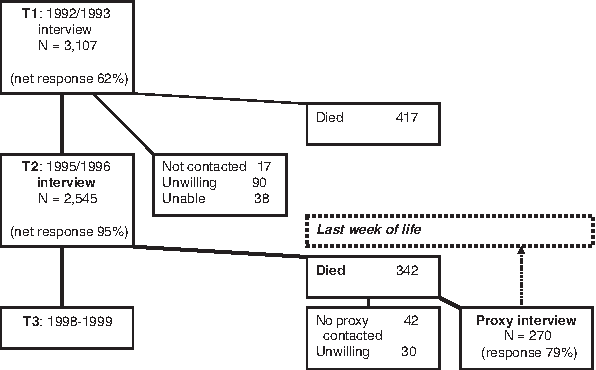
Flowchart of sampling times of the proxy interviews of the deceased respondents of the Longitudinal Aging Study Amsterdam between T2– T3. Significant results are printed in
Measures
Mood in the last week of life
The interview with the proxy respondent included one-item questions on whether the sample member showed feelings of depression or anxiety in the last week of life. Scores were 0 (absence of negative mood) or 1 (presence of negative mood). The proxy respondents also were asked to estimate whether the sample member experienced a sense of peace at the approaching end of life. This was scored as 0 (no sense of peace present) or 1 (sense of peace present).
Religiousness
Data on religious affiliation and church attendance were obtained during the first assessment cycle of LASA. Religious affiliation included Protestant, Roman Catholic, and non-religious. The Protestant group consisted of several denominations, most with origins in the Reformed/Calvinist Protestant tradition. Church attendance was assessed using five response categories, ranging from “once a year or less” (0) to “once a week or more” (5).
The second LASA assessment cycle contained questionnaires on orthodox religious beliefs and salience of religion. Two items of the Orthodoxy Scale 5 were selected for the current study: “Do you believe in heaven” and “Do you believe in Hell.” Response categories were “yes” (1) and “no” (0). Salience of religion was assessed using two items of a religious salience scale [23]: “My religious faith/philosophy of life has a pronounced impact on my daily life” and “When I make important decisions, my religious faith/philosophy of life plays a considerable role.” Response categories ranged from “totally disagree” (0) to “totally agree” (5). Salience of religion was also probed in the proxy interview, using the same items.
Covariates from the LASA respondent interview
Demographic characteristics included were: age of death of the sample member, sex, education in years, marital status (being married versus widowed, divorced, or never married).
Depressive symptoms were measured using the Center for Epidemiologic Studies Depression Scale (CES-D). 24 Subjects were asked how often they experienced each of 20 symptoms during the previous week. The response categories ranged from 0 (“rarely or none of the time”) to 3 (“most of or all the time”), yielding a score range of 0 to 60 (Cronbach α = 0.83).
The number of major chronic diseases was assessed at T2, by explicitly asking the respondents whether or not they had or had had any of the following seven conditions: chronic non-specific lung disease, cardiac disease, peripheral atherosclerosis, stroke, diabetes mellitus, arthritis, and cancer. 25
Covariates from the proxy interview
Physical state. The proxy respondents were asked about the presence of serious physical symptoms in the last week of life of the sample member: fatigue, pain, shortness of breath, confusion, and nausea and/or vomiting. Responses (0 “no”’ and 1 “yes”) were added to obtain a sum symptom burden score (range 0–5).
Cognitive change between the measurement in 1995–1996 and at three months before death was assessed using the six-item short form Informant Questionnaire on Cognitive Decline in the Elderly. 26 For every item, the proxy respondent answered on a five-point scale (range 1-5; Cronbach α = 0.93). Higher sum scores indicate cognitive decline.
Time intervals. The duration of the periods between the T2 interview and death, and between death and the proxy-interview were included to verify for any influence of time on the outcomes.
Whether the sample members had expected death and had been aware of the approaching end was estimated by the proxy respondents, with “yes,” “no,” or “more or less” as response categories. When both questions were answered with “yes,” it was assumed that the sample member clearly realized the approaching end.
Statistical procedure
After inspecting bivariate associations using t-tests and Chi-square tests, associations with the three independent variables on mood (feeling depressed, feelings of anxiety, and sense of peace) were analysed for each of the religious variables, using logistic regression analysis, computing odds ratios (OR) and 95% confidence intervals (95% CI). Adjustment was made for variables with significant associations with the outcome variables. As there was variation in item non-response between the variables, the maximal number of sample members was included in each of the analyses.
Results
Characteristics of the sample
The majority of the sample (Table 1) was male, which conforms to expected higher mortality among males. Mean age of death amounted to 80 years. About one-third were Protestant, one-third Roman Catholic, and one-third unaffiliated. One-third of the sample members used to attend church on a weekly basis. At an earlier measurement, 57% of the sample members reported a belief in Heaven, and 30% reported a belief in Hell. Salience of religion received higher scores by the sample members at their last LASA interview, compared to the report by the proxy respondents. The Cohen κ for inter-rater agreement was low for both salience items (.27 and .25).
High scores indicate more problems.
Depressive mood in the last week of life was reported for 28% of the sample members, anxiety for 31%, and sense of peace for 76%. Depressive mood was strongly associated with feelings of anxiety (χ 2 ; = 30.7, df 216, P < .001) and modestly with sense of peace (χ 2 ; = 4.3, df 182, P = .038). Feelings of anxiety were significantly associated with sense of peace (χ 2 ; = 11.6, df 174, P = .001).
Bivariate associations between covariates and mood in the past week of life
Depressive symptoms, assessed in previous LASA interviews, significantly predicted the presence of depressive mood and anxiety in the last week of life, as well as the absence of a sense of peace (Table 2). Serious physical symptoms and cognitive decline were significantly associated with depressive mood and anxiety in the last week of life. In contrast, cognitive decline and higher age were positively associated with a sense of peace. The time intervals (between T2 and death of sample member, and between death of sample member and proxy interview), were not associated with the outcome variables. No significant associations were found for education, sex, or marital status (on request). Expecting death and being aware of the approaching end were not significantly associated with depressive mood (P = .086) or anxiety (P = .067) in the last week of life, but were clearly associated with a sense of peace (P = .003).
Religiousness and mood in the past week of life, multivariate analyses
The results of the multivariate analyses are shown in Table 3. None of the characteristics of religiousness was significantly associated with depressive mood or anxiety, as estimated by the proxy respondents.
Adjusted for effects by depressive symptoms and number of chronic diseases at the last LASA respondent interview, and physical distress and cognitive decline according to the proxy respondent.
Adjusted for effects by depressive symptoms and number at the last LASA respondent interview, age of death, and cognitive decline according to the proxy respondent, and for expectance of death and awareness of the approaching end, according to the proxy respondent.
Protestant affiliation was associated at the trend level with a sense of peace. More-robust associations with a sense of peace remained significant after multivariate adjustment and were found for weekly church attendance previously in life and the proxy's estimate of the salience of religion. The direction of one association, although not significant, was opposite to what had been expected: Belief in Hell was associated with a sense of peace, according to the proxy respondents. When specified for church members only (product term for church membership and belief in Hell: B = 2.9, P = .040), this association reached significance (OR 4.70, 95% CI 1.19 – 18.51, Wald = 4.9, P = .027).
Discussion
The current study focused on older participants who died during the course of an ongoing prospective gerontological study. Information about the last periods of their lives was obtained from interviews with relatives of the deceased sample members. With respect to the research question of whether aspects of religiousness affect mood in the last week of life, the answer is clearly negative for depressive mood and feelings of anxiety. The data do, however, indicate that some aspects of religiousness may support a sense of peace in the last week of life. This pertained in particular to regular church attendance, the traditional belief of the existence of Hell among church members, and religious salience, as rated by the proxy respondent.
With respect to the outcome variable, the results demonstrate that it may be relevant to include measures of grief or distress, but also measures of acceptance or peace. 11 In a recent trial comparing meaning-centered group therapy with supportive group psychotherapy, 27 a similar pattern of results emerged, with more-prominent effect sizes for the meaning/peace outcome variable than for measures on psychological functioning, such as anxiety or hopelessness.
Supposing that religiousness has a beneficial impact on achieving a sense of peace as one approaches the end of life, it is helpful to ask how this effect could be understood in the process of grief when facing the end of life? Apparently, there was no parallel between the association and any protective effect of religiousness against depressive mood or anxiety. Based on empirical research, Prigerson and Maciejewski rephrased the “stages” of grief as “states” of grief, which appear to co-occur, instead of to succeed each other. 11 It is possible that religiousness relates simultaneously to the other three states of grief as well. Some religious convictions might contain an element of denial of death, such as expecting eternal life. Expressing feelings of anger may be more of a challenge to those who are involved with religion. The stage of bargaining may be more apparent for Roman Catholics, who would consider an investment in realizing good works during life, compared to, for instance, pietist orthodox Protestants, who would refuse such ideas, along with the Calvinist doctrine of predestination (i.e., God's sovereign decision for eternal salvation or eternal damnation).
One may assume that the proxy respondents (especially the spouses) used to have religious beliefs and practices similar to those the respondents had during their lives. The findings about the salience of religion seem to support this assumption: Salience of religion, as reported by the proxy respondent, but not salience as reported by the sample member, was associated with a sense of peace in the last week of life. The results of the current study also may show how religiousness of the proxy respondent helps to cope with the loss of the relative.
One limitation of the current study is that mood in the last week of life was not directly observed in the respondents when they were terminally ill, but was assessed retrospectively. As Addington-Hall and McPherson point out in their review of the validity of after-death interviews, some studies provided evidence that there is little correspondence between the sample member and the proxy respondent on topics such as pain or depressive mood. 28 For the current sample, Klinkenberg and colleague verified some information obtained from the proxy respondents against reports from physicians. 29 The proxy respondents seemed to provide accurate information with respect to chronic physical conditions.
According to research on the concordance of patient and caregiver reports, both patient and caregiver depression was a common predictor of disagreement. 30 Although the results of the current study were adjusted for possible effects of depressive symptoms at an earlier assessment, further reasons for non-concordance could not be ruled out. The same is true for recall bias by the proxy respondents, many of whom were interviewed two years after the patient died. An important dilemma in research about the end of life remains that few respondents can be identified in time, and, even if they are, few will be able or allowed to participate. Interviews with relatives, therefore, will remain a source from which to obtain knowledge about someone's last phase of life.
Another limitation is that all three outcomes consisted of one-item measures. One recommendation for future research is to examine the state of mood more extensively. Meanwhile, psychometrically acceptable measures of the quality of the dying experience have become available, such as two versions of the Quality of Dying in Long-Term Care instrument. 31 Furthermore, more aspects of religiousness (e.g., such as on God image or prayer), spirituality, and secular sources of meaning in life may be included in further research.
Kastenbaum (author of The Psychology of Death) holds that the stage of “acceptance” does not necessarily imply a deep philosophical point of view. 9 More often, it embodies a sense of rest, after the emotional turmoil of previous stages. The recent guidelines and recommendations for the quality of spiritual care as a dimension of palliative care provide suggestions for screening questions that can be used to assess spiritual life in patients in palliative care, to keep an eye on spiritual distress or religious struggle, and to integrate spiritual issues into the treatment plan. 32 For professionals in a hospital setting, the question “Are you at peace,” as a phrase to open with, 33 has received empirical validation. Such a question may meet with some hesitation among health care professionals in a predominantly secular context such as in the Netherlands. Nevertheless, this phrase may offer a rightful appeal: As a complement to accurate somatic care, some understanding of existential matters seems to be feasible and humane.
Footnotes
Acknowledgments
The authors would like to thank the editorial board of the Tijdschrift voor Gerontologie en Geriatrie (Dutch-Flemish) for their cooperation in submitting the current manuscript, which is a translation into English of a previous version of the current paper, published in the Tijdschrift voor Gerontologie en Geriatrie, 2006; 37:254–262.
Author Disclosure Statement
The data reported on were collected in the context of the Longitudinal Aging Study Amsterdam (LASA), which is financed primarily by the Netherlands Ministry of Welfare, Health, and Sports. The study of religious resources and common mental disorders was supported by a grant from the Netherlands Organisation for Health Research and Development (ZON-MW grant 2003-05769).