
Abstract
Background:
The factors for assessing the utilization rate of a palliative care service are various and complex. Several authors have described different methods to address this problem. McNamara and colleagues have proposed criteria to determine “minimal,” “mid-range,” and “maximal” palliative population estimates. In order to evaluate the utilization of our intrahospital palliative care consult team (PCT), it appeared necessary to better describe and define the population who dies in our institution, a Swiss university hospital. The goal of this pilot study was to determine what percentage of patients who died in our hospital over a 4-month period in 2007 was seen by the palliative care consult team (PCT), using “minimal” and “maximal” population estimates.
Methods:
The hospital database was searched for all adult patients who died during that period and the “maximal” and “minimal” populations determined. The PCT's database was searched to identify those patients who had been seen by the PCT. The charts of a random sample of patients who did not initially meet the “minimal” criteria were hand searched.
Results:
A total of 294 adult deaths were reported: 263 (89%) met the “maximal” criteria and 83 (28%) met the “minimal” criteria initially. The random search of 56 charts of the 180 patients who did not meet the “minimal” criteria revealed that 21 (38%) should have been included in the “minimal” population. The PCT saw 67/263 (25.5%) of the “maximal” palliative patient population and 56/151 (37.1%) of the “minimal” palliative population.
Conclusion:
This study highlights the usefulness of the method proposed by McNamara and colleagues to determine palliative populations. However, it also illustrates an important limitation of the “minimal” estimate and reliance on the accuracy of the cause of death as noted on the death certificate. A strategy to address this limitation is suggested. The “maximal” estimate suggests that the PCT is being underutilized.
Introduction
While the numerator is relatively easy to determine (patients referred to the palliative care service, taken from the service's database), the patient population that would benefit from a palliative care approach, either from their attending team or a specialized palliative care service, is more elusive. In some cases, patients who require palliative care are easily identifiable. This is the case with people admitted for complications related to advanced cancer or end-stage neurological diseases. Other cases are easily excluded: people dying suddenly and unexpectedly of trauma or a myocardial infarction. However, appropriateness for receiving palliative care is not always straightforward. Palliative care could be appropriate for a patient who later dies after a prolonged stay in an intensive care unit because of injuries sustained in an accident. Death certificates may state the cause of death as being cardiac arrest but fail to highlight that cardiac arrest followed a prolonged cancer, pulmonary, cardiac, renal, or neurological illness.
The optimal rate of referral to a specialized palliative care consult team and use of such services is also elusive. While it would be inappropriate for a specialized palliative care consult service to see every patient deemed to have a progressive incurable or life-threatening illness (i.e., deemed “palliative”), a low rate of referrals to such a service would generally be a concern and would suggest that many patients are missing the opportunity of benefiting from the team's expertise. Recent studies, for example, have noted that specialized palliative care services are able to identify previously unrecognized problems and needs,2–5 reduce hospital costs when consulted early, 6 reduce number of inappropriate interventions, 5 and improve symptom control.2,4,7
The factors for assessing the usage rate of a palliative care service are multi-factorial, various and complex. Several authors have described different methods for addressing this problem.
One approach to determining a palliative care service's level of use is to identify the percentage of patients with anticipated deaths in the hospital who were seen by the palliative care service. For example, in an Australian study, Le et al. classified deaths as expected or unexpected according to whether there was evidence in the medical record that the death had been anticipated by treating physicians. 8 Of the 45 anticipated deaths over a period of one month, 17 (38%) were referred for consultation by the palliative care team. Fifteen deaths had been deemed unexpected (mainly deaths in the emergency department and intensive care unit from acute myocardial infarctions, sepsis, and trauma) and were excluded from the analysis.
Lagman reported similar results and proposed that these rates represent underuse of in-hospital palliative care mobile services.9,10 Santa-Emma and colleagues reviewed referrals to palliative care services in an acute care system that consists of three hospitals in the United States (total of 1036 beds). 11 In both 1999 and 2000, the palliative care service was involved in the care of 44% of all non-trauma–related inpatient deaths. In all three studies, however, the inclusion and exclusion criteria were not described precisely.
Due to concerns that our intra-hospital palliative care consult team is being underused at the Centre Hospitalier Universitaire Vaudois (CHUV), we initiated this study to better describe and define the population who may benefit from our intra-hospital palliative care consult team (PCT). The CHUV is an 850-bed referral and teaching hospital in the Canton of Vaud, Switzerland, with approximately 37,700 admissions per year. It does not have an inpatient palliative care unit. The palliative care consult team (PCT) is an inter-professional team of nurses, physicians, a psychologist, a chaplain, and a social worker.
This pilot study aims to characterize the patients who die in our hospital by using the diagnosis codes listed on their death records. The study represents a substudy of a larger anthropological study on the status of palliative care in the canton. Important methodological considerations are reported.
Methods
We used the framework proposed by McNamara et al. to identify the “palliative population.”1 This framework relies largely on the causes of death as reported on death certificates. These, in turn, are based on the International Codes for Diagnosis International Statistical Classification of Diseases and Related Health Problems (ICD). “Minimal,” “mid-range,” and “maximal” estimates of the palliative care population can be determined.
The “minimal” estimate, which is condition-specific, includes all patients with deaths from 10 diseases. These illnesses include cancer, heart failure, renal failure, liver failure, chronic obstructive pulmonary disease, motor neuron disease (including amytrophic lateral sclerosis), Parkinson's disease, Huntington's disease, Alzheimer's disease, and HIV/AIDS. The mid-range estimate uses a needs-based approach. This estimate includes patients in the “minimal” estimate and those admitted to hospital during the 12 months preceding death, with the reason for admission matching the underlying cause of death on the death certificate. The “maximal” estimate provides the least-restrictive definition of a palliative care population and includes all deaths, excluding those not considered amenable to palliative care (i.e., deaths due to poisoning, trauma, or originating during pregnancy, childbirth, or the puerperium or perinatal period). Conceptually, therefore, the “minimal” and “mid-range” estimates are subgroups of the “maximal” population estimate (see Figure 1). The “minimal” and “maximal” estimates were determined in this study.
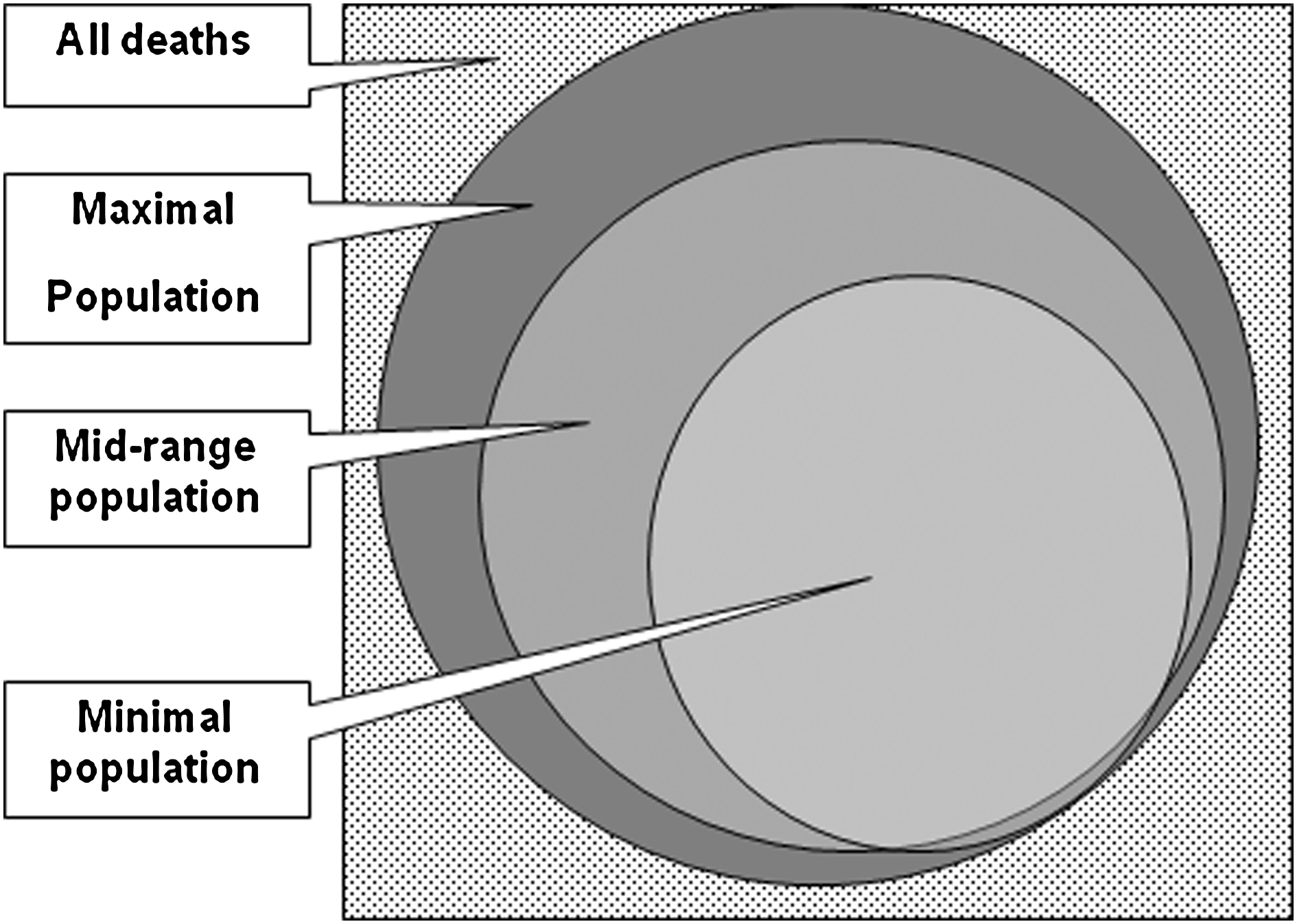
“Minimal” versus “mid-range” versus “maximal” palliative population estimates. 1
We used a four-month period (1 February–31 May 2007). While this was chosen for convenience, a review of the PCT's level of activity revealed that this four-month period appeared to adequately represent the team's activities for the entire year. The hospital's patient database was searched, using McNamara et al.'s criteria, to determine the “minimal” and “maximal” patient populations. The CHUV's use of the ICD-10 coding system facilitated the process. Consistent with McNamara et al.'s recommendations, which allow for minor modifications to address local circumstances, some minor adjustments were made to the original criteria. These included adding: a) dementia in the “minimal” criteria list, as these types of cases are occasionally seen by the PCT; b) hypertensive cardiopathy with heart failure to the list of congestive heart failure codes; and c) alcoholic cirrhosis to the hepatic failure list of codes. The PCT's database was also searched to identify the patients referred to and seen by the service during the four-month period and their charts reviewed.
On rare occasions, the PCT is consulted for advice on non-palliative patients (patients without progressive, incurable, or life-threatening illnesses). These patients were excluded. Although the hospital also has a separate pediatric palliative care consult service, the study focused on the adult population (≥18 years of age).
A pilot search of the database and manual review of a set of 10 patient charts revealed that, while it was relatively unproblematic to determine the “maximal” patient population, estimating the “minimal” group was more challenging. Some patients clearly met the criteria for the minimal group; their causes of death were among those listed in McNamara et al.'s criteria. However, for others, the cause of death as represented on the death certificate did not necessarily exclude the patient from the “minimal” criteria.
Some patients with causes of death entered as “cardiac arrest” or “pneumonia,” for example, had, in fact, been admitted to the hospital because of complications related to illnesses listed amongst McNamara et al.'s minimal inclusion criteria. These patients, therefore, should have been included in the minimal population even though the death certificate did not indicate so. Patients were, therefore, allocated to one of two groups, depending on the causes of death listed in the hospital database (which had, in turn, been extracted from their death certificates). Group A included patients whose cause of death was one of those listed in the minimal criteria (and, therefore, clearly met the inclusion criteria), while Group B were those patients whose causes of death were not on the list. To explore the extent to which Group B patients should have been included in the minimal population, the charts of 31% of patients in Group B were randomly extracted and manually reviewed together by a physician (MB) and a social scientist (RF). Those who should have been included in the minimal patient population were identified.
The hospital's research ethics committee approved the study.
Results
A total of 932 deaths were recorded in the CHUV in 2007; 318 in the 4-month period studied. Of these, 294 were of persons aged 18 years or older and 26 of these (8.8%) died within 24 hours of being admitted into hospital. As shown in Figure 2, 263 patients out of the 294 adult deaths (89%) met the maximal criteria.
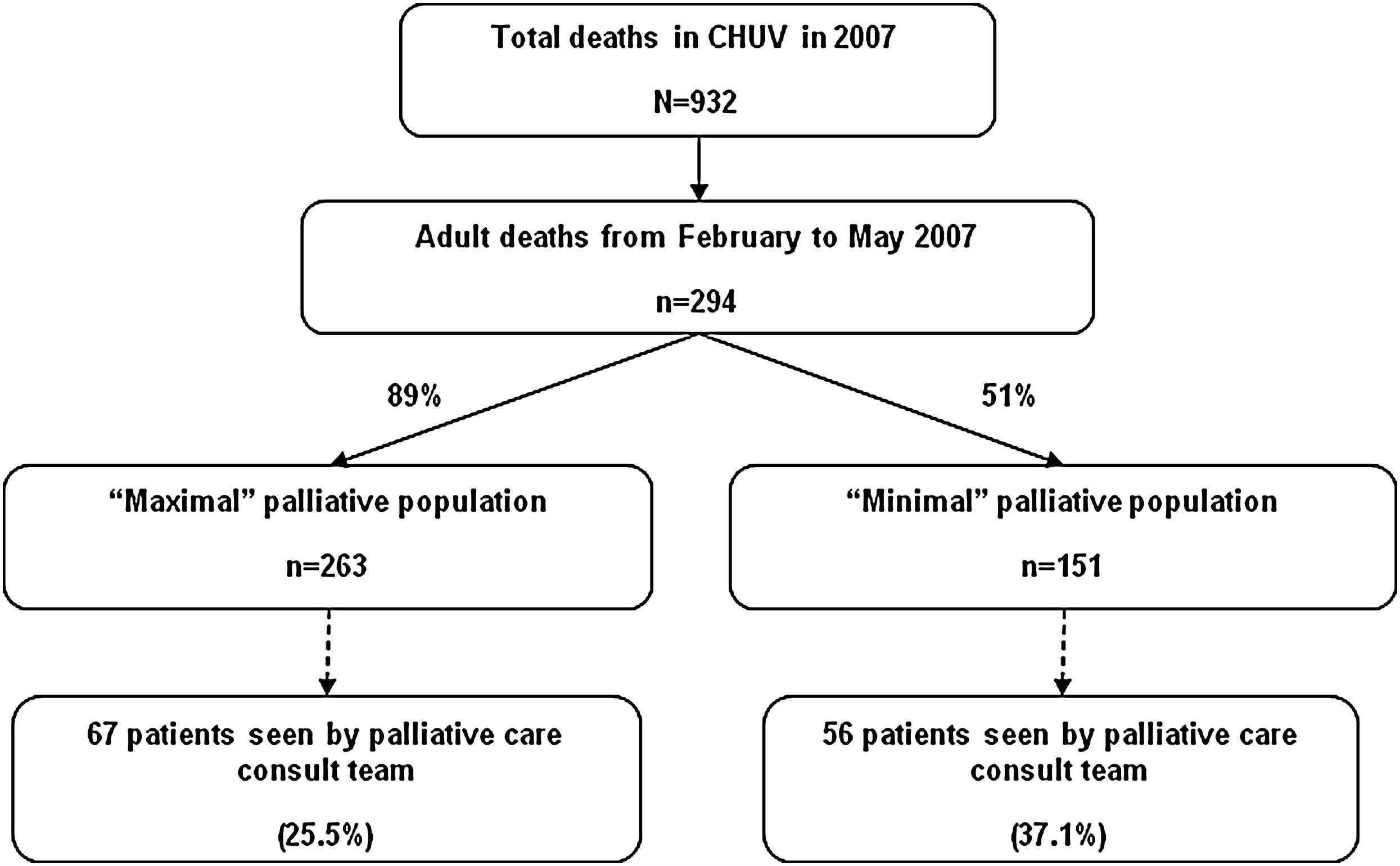
“Minimal” versus “maximal” palliative patient populations during the period February–May 2007 and number of these patients seen by palliative consult team (using McNamara et al.'s criteria 1 ).
Figure 3 summarizes the calculations undertaken to arrive at the “minimal” population. Eighty three out of the 294 (28%) adult deaths met the “minimal” criteria from the outset (i.e. were allocated to Group A), while 180 patients (66%) were allocated to Group B (primary diagnoses/causes of death needed to be verified). The charts of 56 of the patients allocated to group B (31%) were randomly selected and reviewed in detail manually (Using a confidence level of 95%, this sample size yielded a confidence interval of ± 10.6; which would be acceptable). Twenty-one out of 56 of these charts (38%) were found to be appropriate to be included in the “minimal” population estimate as their primary diagnoses corresponded with those listed in McNamara's list of diagnoses. Furthermore, their hospitalizations were related to these diagnoses. Based on this 38% result, it was inferred that 47 out of the 124 patients in Group B whose charts were not reviewed should be included in the “minimal” patient population estimate. The final “minimal” population estimate therefore came to 151 (83 from Group A, 21 from the sample review of Group B, and 47 from the “non-reviewed” Group B). This constituted 51% of all the adult deaths over the 4-month period (See FIG. 3).
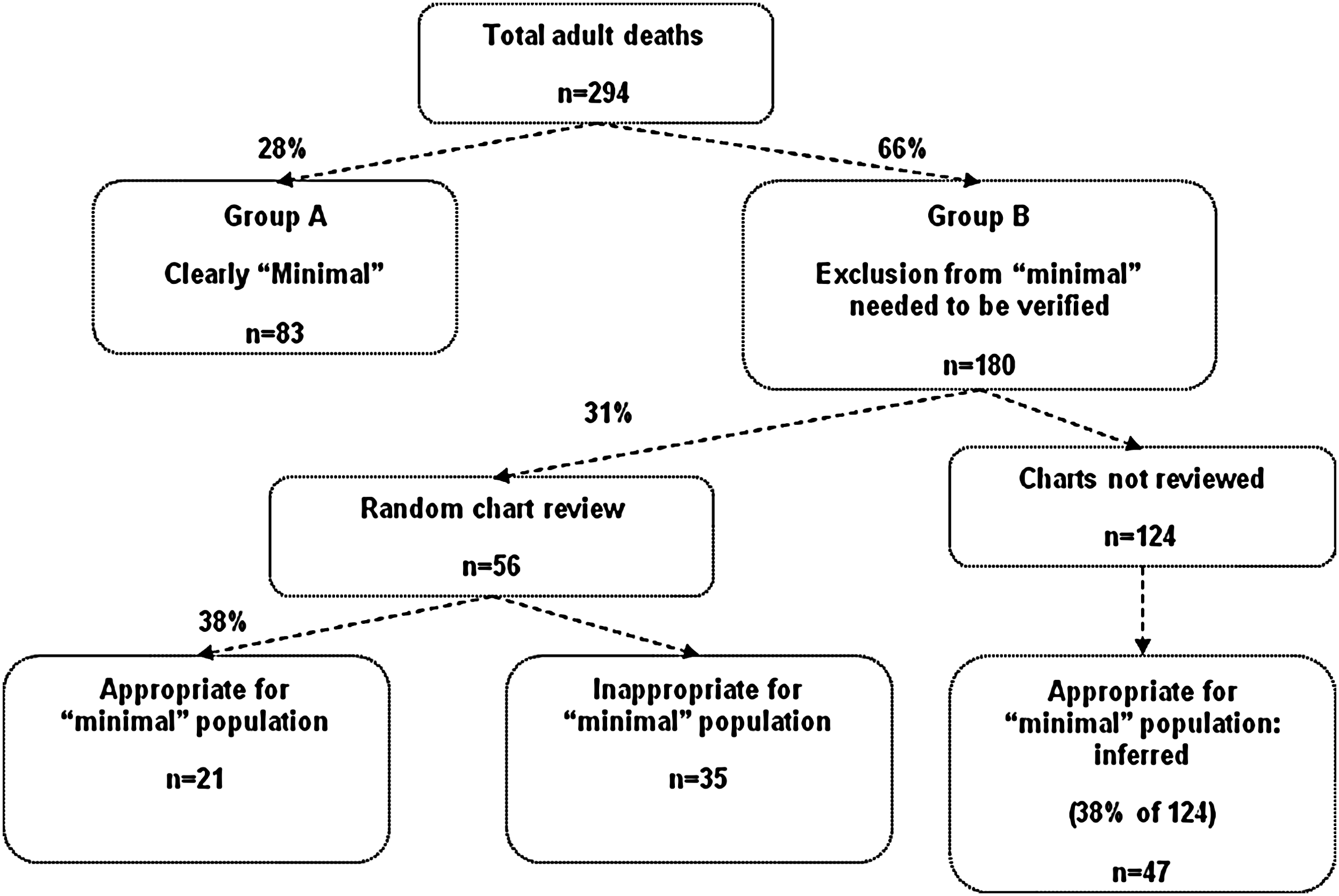
Calculation of “minimal” palliative population.
The PCT received a total of 439 consultation requests in 2007; 143 during the 4-month period studied. Of these, 2 patients' charts were not available. Sixty-nine of the patients who had died in the CHUV during that time period had been seen by the PCT (23% of all the deaths). Of the 69 patients seen by the PCT, only two did not meet the “maximal” criteria. Both patients had died of trauma; one following a motor vehicle accident and the other following a fall. The team therefore saw 67 out of 263 (25.5%) of the “maximal” palliative patient population.
Of the 69 patients seen by the PCT, 56 met the “minimal” criteria. Two patients had died of trauma (previously described) and eleven of diagnoses not usually included in the “minimal” criteria (4 patients of strokes, 2 patients of a intra-cranial hemorrhage, 1 of a stroke and myocardial infraction, one of heart failure secondary to broncho-aspiration, one of intestinal ischemia and one of a myocardial infarction with heart failure). Therefore 56 out of 151 of the “minimal” population were seen by the PCT (37.1%).
Discussion
The criteria for determining “minimal”, “mid-range” and “maximal” palliative population estimates proposed by McNamara and colleagues is a useful standardized approach in an process seeking to assess the utilization of a PCT. 1 However, as our study demonstrates, a cautionary note is advised.
In this study, 31% of patients initially excluded from the “minimal” population on the basis of what had been written on their death certificates as the cause of death were indeed appropriate for inclusion in the population. Had they been excluded, the population would have been significantly under-estimated. The problem relates to the accuracy of the cause of death as entered by the attending physicians on the death certificate, rather than McNamara et al's approach. Concerns with the quality of the data derived from death certificates have previously been noted. Myers and Farquhar, for example, identified major errors on 32.9% of the death certificates completed in an inpatient teaching hospital setting, a rate that was comparable to previously reported rates for internal medicine services in teaching hospitals. 12 Coronary heart disease has been overrepresented as a cause of death on death certificates, 13 and the underlying cause of death as coded on the death certificate has been found to be accurate for only about 65 per cent of the cancer deaths. 14
Given these inconsistencies, it is important to ascertain whether or not a problem exists with the accuracies of the causes of death in the database being used, particularly when using Mcnamara et al's “minimal” population estimate. If, as in this study, a significant problem exists, an adjustment may be required. The strategy undertaken by our group provides an approach. We separated the patients that definitely met the “minimal” criteria from those that did not at first glance. We then randomly hand searched a sample of these that did not appear to meet the criteria to identify the number of patients who should actually have been included. This information was used to calculate, by means of inference, the “true” minimal population. Random sampling may be particularly useful when a large database is being studied and sample size formulas may be used to determine an adequate sample size. These generally require a predetermined confidence level (usually 95%), a confidence interval and the population number (in this case the deaths not initially included in the “minimal” criteria).
Having made the necessary adjustments, the size of our “minimal” palliative patient population estimate was 51% of all adult deaths in the hospital. This figure is consistent with the 50% found by McNamara and colleagues in their Australian-based study with a valid population of over 27 000. 1 Our “maximal” population estimate, namely 89% of all adult deaths, is identical to that reported by McNamara et al in their large study in Australia. These similarities are reassuring and suggest consistency of this method of estimating palliative patient populations across different countries, health systems and cultures.
Our team was called to see 26% of the “maximal” patient population. This number is concerning and appears to represent an underutilization of our service when compared to previous reports that noted rates of 38% to 44%.8–11 A comparison with these reports is justifiable because they appear to approximate a “maximal” patient population in that they focussed on all “anticipated” deaths in their respectful hospitals and excluded sudden, unexpected deaths.
A number of factors influence utilization of palliative care services and these should be accounted for when comparing utilization across different services. Rodriguez et al has explored some of these in the hospital setting. 15 Services may use different models of practice; one may practice in a purely consulting role while another may use a shared-care approach. Hospitals may differ in the services they offer. Some, for example, may focus only on cancer care. Of the patients seen by our PCT, 35% have non-cancer diagnoses. Furthermore, admission rates and mean durations of hospitalization may vary from centre to centre. It could also be argued that some patients included in the “minimal” estimate by virtue of the death causes should perhaps be excluded, particularly those who died within only a few hours of being admitted to hospital. In these cases there may not have been sufficient time for a palliative care consultation.
This small study has some limitations. Focussing on only deaths excludes services rendered to patients who were discharged. In some cases this may be significant and a “minimal” or “maximal” approach may underestimate the utilization of a palliative care service. The study also brings to attention an important limitation of the “minimal” estimate; namely the reliance on the accuracy of the cause of death as noted on the death certificate.
Conclusions
This study highlights the usefulness of the method proposed by McNamara and colleagues to determine palliative patient populations. Its more widespread use as a standardized approach to evaluate palliative care service utilization in hospitals is encouraged. However, dependence on the stated death cause on the death certificate may, in some cases, significantly underestimate the “minimal” patient population. A hand review of an adequate sample of charts may be required to explore the extent to which the causes of death do not reflect the underlying diseases which were responsible for the death. If significantly large, adjustments may be required. The study also suggests that the utilization of the palliative care consult service at the CHUV is being underutilized. We intend to carry out a broader prospective study using the same method in order to deepen the results of this pilot study.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.