
Abstract
Abstract
Objectives:
Many patients with amyotrophic lateral sclerosis (ALS) develop progressive difficulty swallowing secretions, leading to drooling. Although external beam radiation is considered to be an effective and well-tolerated treatment, the optimum schedule in terms of dose, target, radiation type, and number of fractions is unknown. The aim of this observational study was to define the most effective schedule for salivary gland irradiation and to compare electron and photon radiotherapy.
Methods:
Sixteen patients with ALS (12 females and 4 males) with drooling, enrolled for external radiation of salivary glands between 2002 and 2007, were included. Patients received different treatment protocols according to the decision of their radiotherapist. Efficacy and safety were assessed at 1 and 6 months after treatment by a neurologist and a radiotherapist using a 4-point Likert patient improvement scale, as follows: 0 (no change), 1 (slight improvement), 2 (good improvement), and 3 (very good improvement).
Results:
Radiotherapy for drooling was shown to be safe and effective in ALS patients with duration of effect expected up to 6 months. Eighty percent of patients felt improved at 1 month and 43% at 6 months after external radiation. Patients with sustained improvement at 6 months were treated with electron therapy (>8 MeV; p = 0.02).
Conclusions:
Electron-based radiotherapy, delivered as five 4Gy fractions to a total dose of 20 Gy, encompassing the whole of the submandibular gland and sparing the upper part of the parotid gland, can be proposed as a safe and effective schedule for the treatment of sialorrhea in patients with ALS.
Introduction
Various treatments have been proposed.1–3 Systemic anticholinergic drugs may have side effects when higher doses are required with progression of the disease. 4 Injection of botulinum toxin into the salivary glands (directly acting on parasympathethic postganglionic activity in parotid and submandibular glands) has given interesting results,5–11 but acute deterioration of bulbar function may occur. 12 Surgery, consisting of salivary gland removal, could be invasive for medically compromised patients. 13
In ALS, as in Parkinson's disease, external radiation had been proposed, as a dry mouth is a well known side effect of radiotherapy for head and neck cancer. Moreover, the short life-expectancy of patients with ALS reduces the risk of radiation-induced neoplasia. External beam radiation is considered to be an effective and well-tolerated treatment.14–19 However, the optimum schedule in terms of dose, target, radiation type, and number of fractions is unknown. The aim of the present study was to define the optimum modalities for external radiation.
Methods
Subjects
All patients with ALS, between 2002 and 2007, with an Amyotrophic Latreral Sclerosis Functional Rating Scale (ALSFRS) score for sialorrhea 2 or more, enrolled for external radiation of salivary glands, were included in the study. All patients fulfilled the El Escorial criteria for definite diagnosis of ALS. Data were collected prospectively every 3 months between 2002 and 2007. They were stored in an electronic database and analyzed retrospectively.
Before radiotherapy, all patients had undergone pharmacologic therapy with anticholinergic drugs or injection of botulinum toxin with unsatisfactory results. In all cases, the patient's head was fixed with a thermoplastic head mask during radiotherapy (approximately 10 minutes). Fixation was necessary in order to accurately define the irradiation area and for dose planning by tomography or three-dimensional computed tomography (CT). Because the best radiation schedule is not well defined, patients received different doses, fractions, and radiation types according to the choice of their radiotherapist. Patients were treated with either electron (6–15 MeV, a total dose of 20 Gy) or photon (5.5 MV, a total dose ranging from 4–48 Gy) radiation. The target volume included the submandibular and two thirds of the parotid salivary glands.
Assessments and outcome
The results were assessed at 1 and 6 months posttreatment by a neurologist (N.G. or P.C.) and a radiotherapist (N.B. or M.L.). The effect of the treatment was assessed in three different ways: the subscale salivation ALSFRS score, the 4-point Likert scale, and the type and number of undesirable effects. The subscale salivation ALSFRS score, which measures sialorrhea, is a 5-point-scale ranging from 4 (normal) to 3 (slight but definite excess of saliva in the mouth; may have night-time drooling), 2 (moderately excessive saliva; may have minimal drooling), 1 (marked excess of saliva with some drooling) and 0 (marked drooling; requires constant tissue or handkerchief). ALSFRS score was measured before and 1 month after radiation. The 4-point Likert scale was used to assess patients' satisfaction. It varies from: 0 (no change) to 1 (slight improvement), 2 (good improvement) and 3 (very good improvement).
Data recorded included demographic and nosological characteristics (age, body mass index [BMI], ALS clinical form, disease duration, pCO2, delay from diagnosis to onset of sialorrhea), radiation procedure (delay from diagnosis to treatment, total dose, number of fractions, radiation type, target), and outcome at 1 and 6 months posttreatment (satisfaction score, adverse events). Capillary pCO2 was used to assess respiratory status, as vital capacity or maximal inspiratory pressure was difficult to measure in bulbar patients.
Statistical analysis
Comparisons were carried out using the Student's t test, Fisher's test, and Spearman correlation test. All analyses were carried out using the Excel* statistics program.
Results
Study population
Sixteen patients with ALS (12 females and 4 males) with severe hypersialorrhea or drooling underwent external radiation between 2002 and 2007. The mean ALSFRS scores for sialorrhea were 0.43 ± 0.50 and 9 patients had a score of 0. Mean age at disease onset was 61 ± 11 years. Fourteen patients had bulbar onset. Mean disease duration before the development of early sialorrhea was 12.5 ± 5.1 months. All patients were initially treated with anticholinergic drugs and 1 patient also received botulinum toxin.
Radiation modalities
The median delay to onset of radiotherapy was 21 months (range, 13–86). Seven patients were treated with electrons and nine with photons according modalities resumed in Table 1. At the time of treatment, 11 patients (68%) were receiving enteral nutrition. Mean BMI at radiotherapy was 20 ± 3. All patients had a capillary pCO2 less than 43 mm Hg.
Four point Likert scale: 0 (no change), 1 (slight improvement), 2 (good improvement) and 3 (very good improvement).
Gy, Gray; MeV, mega-electrons-Volt; MV, mega-volt.
Although the choice of radiation type (photons or electrons) was arbitrary and depended on the radiotherapist, there was no difference in patient characteristics according to the type of radiation given (Table 2).
All values shown are mean ± standard deviation, or number of patients.
ALSFRS, Amyotrophic Lateral Sclerosis Functional Rating Scale.
Efficacy
Using Likert scale, 80% of patients felt improved at 1 month and 43% at 6 months posttreatment. The efficacy data are summarized in Table 1.
Nevertheless, although there was no significant difference between the electron group and photon group at 1 month, patients with sustained improvement at 6 months had been treated with electrons (p = 0.02; Fig. 1A). A decrease in effect was observed in the photon group between 1 and 6 months (p = 0.04; Fig. 1B).
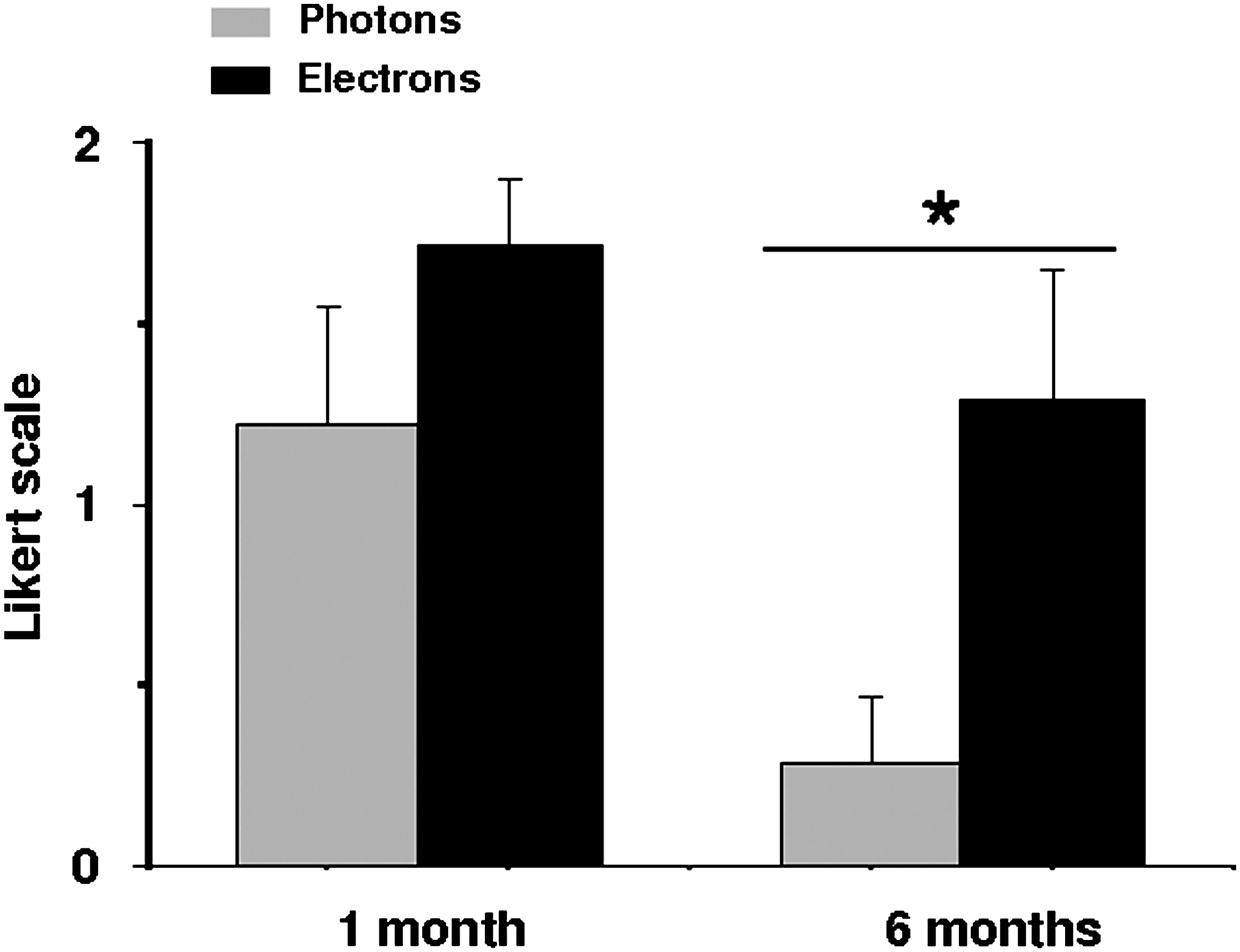
Improvement status according to radiation type and time. *p < 0.05.
One month after radiation, the mean ALSFRS subscore improved, although not significantly, from 0.43 ± 0.50 to 0.62 ± 1.08. However, a significant improvement was obtained in three patients receiving electron therapy while no improvement was observed in patients receiving photon radiation.
All patients in the electron group received 20 Gy in five fractions. The best improvement scores at 1 and 6 months were obtained with a radiation penetrating power of more than 8 MeV. The radiation area encompassed both the submandibular and parotid glands bilaterally with an ipsilateral field except for two patients (numbers 13 and 14, Table 1) who were treated with 6 MeV. Dose planning for these two patients revealed that radiation did not encompass the entire submandibular gland.
In the photon group, all patients were treated with 5.5 MV. There was no significant correlation between total dose and improvement score at 1 month (Spearman: S = 94.9, p = 0.59; ρ = 0.2) and 6 months (S = 121.2, p = 0.97, ρ = −0.01).
Adverse events
In the electron group (n = 7), two patients reported slight mouth dryness, a consequence of efficacy (Table 1). None complained of pain, edema, or erythema. In the photon group (n = 9), one patient reported pain and edema requiring interruption of radiotherapy after three fractions (Table 1). Another did not tolerate immobilization due to respiratory failure, and stopped treatment after the first fraction.
Two patients died between 3 and 6 months. These deaths were not related to radiotherapy but were due to ALS-related respiratory failure.
Discussion
Palliative radiotherapy was effective at reducing sialorrhea in ALS, in accordance with previous reports.14–17 However, these observations should be interpreted with caution because of the small sample size and because objective measures were lacking. Nevertheless, in palliative care, a perception of improvement and increased comfort, although subjective, appear to be the best end points, as suggested previously by Postma et al. 18 in Parkinson's disease.
To our knowledge, this is the first study to compare two radiation types in ALS. The objectives were to alleviate drooling with as few adverse events as possible and to assure the best comfort, for as long as possible.
Improvement of drooling after electron therapy appeared to be sustained for significantly longer than after photon therapy, with no serious adverse events. This is reinforced by the lack of a difference in patient pattern and treatment delay between groups even although patients were not randomized.
Several previous studies have shown that photon14–17 or electron 16 therapy can improve drooling in ALS. However, it was not possible to determine whether the study populations were comparable in these studies. One study evaluating the efficacy of photon therapy at 6 months showed that two thirds of patients had sustained improvement at this date. 17 Mean survival without drooling was 9 months in another study although photons and electrons were not compared. 16 No other studies in ALS have provided follow-up to 6 months. In the study of Neppelberg et al., 15 a 21% reduction in salivary secretion was measured at 3 months with sustained perceived improvement in 57% of patients. The follow-up periods in other radiation studies were substantially shorter.
In our study, two patients given 6 MeV electron therapy delivered as five 4Gy fractions to a total dose of 20Gy had unsatisfactory results. CT dose-planning and volume delineation for these two patients revealed that radiation did not encompass the entire submandibular gland.
Three major pairs of salivary glands (parotid, submandibular and sublingual) produce over 90% of saliva. The parotid glands are the largest and are located between the mandible and mastoid process and below the external auditory meatus. The submandibular glands are located below the buccal floor near the body of the mandible. At rest, the parotid glands contribute 20% of total secretions and the submandibular glands 65%. During meals, the parotid secretion flow rate increases to 50% of total secretions. 19 Thus, total submandibular radiation may be necessary to diminished the secretion flow at rest and suppress drooling. Because electrons are highly absorbed by tissue, they need sufficient energy (>8 MeV) to reach the entire submandibular gland. Conversely, the development of thick secretions can be avoided by sparing the upper part of the parotid glands in the radiation field.18,19 A number of adverse events, such as erythema, sore throat, pain, aching, or burning sensations, have been reported previosuly.14,15,17 In our study, except for dryness, these adverse events occurred in only one patient treated with photons. The 5.5 MV photons are much more penetrating than electrons and this could explain the slightly higher incidence of local pain, erythema, and burning sensations (Fig. 2). The use of electrons was proposed by Borg and Hirst in 1998 to treat drooling in elderly neurological patients. 20 The lower penetration of electrons allows more precise targeting of radiotherapy with better tolerance.

Dose planning for (
One patient in our study did not tolerate immobilization and treatment was stopped after one fraction because of respiratory impairment. Two others died of respiratory failure between 3 and 6 months. All three suffered from orthopnea before treatment. Because radiotherapy of salivary glands requires head fixation on a horizontal plane for approximately 10 minutes, good respiratory function is essential, particularly the absence of orthopnea. Physical examination is necessary to detect accessory muscle recruitment, supine abdominal paradox, and encumbrance of the upper and lower airways. Spirometry with measurement of maximal inspiratory pressure and supine vital capacity may improve the detection of diaphragmatic involvement, but this evaluation is difficult to perform in bulbar patients. Sniff nasal inspiratory pressure is easier to measure and can be performed in association with capillary or arterial blood gases to detect hypercapnia. 21 Radiotherapy should not be proposed to patients with clinical orthopnoea, hypercapnia greater than 45 mm Hg or severe diaphragmatic involvement, even in the presence of noninvasive ventilation.
Radiotherapy for drooling is safe and effective in patients with ALS without risk of bulbar function deterioration. Although there is no comparative study in the literature, radiotherapy appears to be a good alternative to botulinum toxin when anticholinergic drug therapy has failed. Furthermore, a sustained effect up to 6 months is observed after radiotherapy. Between 8 and 15 MeV electrons, delivered as five 4-Gy fractions to a total dose of 20 Gy, after CT-based three-dimensional dose planning, encompassing the whole of the submandibular gland and sparing the upper part of the parotid gland can be proposed as a therapeutic scheme. Further prospective studies comparing different radiation schedules over as long a follow-up period as possible are required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.