
Abstract
Abstract
Background:
Clinical experience and a limited number of studies suggest that a cancer diagnosis confers a high risk of accidental falls. The negative sequelae of falls in older persons are well documented; risk factors for falls in this population have been extensively investigated and evidence for the efficacy of interventions to reduce falls is steadily emerging. It is not known whether the risk factors for falls and effective interventions for falls risk reduction in patients with cancer are different from those in older persons.
Methods:
Electronic databases MEDLINE, Embase, and CINAHL were searched for studies of risk factors for falls or effective interventions for falls risk reduction in patients with cancer. Assessment of study quality was performed. Data analysis was descriptive.
Results:
Seven studies designed to identify the risk factors for falls in patients with cancer and one study to determine the predictive validity of a screening tool for falls in patients with cancer were included. All had methodological shortcomings, precluding the generation of a new synthesis from this review, but highlighting important design and statistical issues.
Conclusions:
Further research is needed to identify patients at risk and inform the design of an interventional model to reduce falls risk. Investigators should be cognizant of the limitations of using cross-sectional study design to answer this research question, should employ validated tools to measure exposure variables, use reliable methods to ascertain the occurrence of falls and appropriate statistical models to adjust for confounding variables.
Introduction
Falls represent a serious problem in older people; one third of community dwelling persons aged 65 or older fall annually and approximately 10% of falls result in fracture, head injury, or serious soft tissue injury.1,2 Even noninjurious falls have significant negative consequences for the individual with up to 40% of those who fall subsequently experiencing a fear of falling. Fear of falling is associated with self-imposed activity restriction, which although in the short term may protect against falls, ultimately leads to decline in physical performance, independent of baseline function, and to development of gait and balance problems. 3
The high incidence of falls in older persons is attributed to a complex interaction of intrinsic and extrinsic risk factors, and the risk of falls increases with each additional risk factor. Intrinsic risk factors include cognitive impairment, neurological conditions, polypharmacy, the use of psychotropic or cardiovascular medications, impairment in balance, gait, and functional mobility, muscle weakness, decline in visual function, and low blood pressure states such as orthostatic hypotension and carotid sinus hypersensitivity. 4
Evidence of effective interventions for reducing falls risk in selected or unselected populations of older persons, is steadily emerging. Multicomponent interventions that target multiple risk factors, targeted exercise interventions, home hazard modification, reducing psychotropic medication and correction of vitamin D depletion have all been shown to be effective interventions for community-dwelling older persons.5,6
Do Patients with Cancer Have a High Incidence of Falls?
In the course of our experience of provision of palliative care services we observed falls to be a common occurrence in people with advanced cancer. A preliminary look at the literature revealed evidence of an association between a cancer diagnosis and falling; in a longitudinal study of 146,959 postmenopausal women, Chen et al. 7 found the hazard ratio for falling after incident breast cancer diagnosis to be 1.15 (confidence interval [CI] = 1.06–-1.25) and 1.27 (CI = 1.18–1.36) after other cancer diagnosis. In a study of falls risk factors in hospital inpatients, a diagnosis of cancer was associated with a relative risk of falling of 2.7. 8 Based on analysis of incident forms over a 1-year period, researchers in the United Kingdom reported fall rates of 15.6 falls per 1000 bed-days in palliative care inpatient units (IPU) within a single cancer network. 9 This far exceeds the average rates of falling in acute and community hospitals in the United Kingdom of 4.8 falls per 1000 bed-days and 8.4 per 1000 bed-days, respectively. 10
The susceptibility of patients with cancer to falling has not gone unrecognized. There are many references in nursing literature to the need to recognize and address the high risk of falling associated with a cancer diagnosis. Authors advocating evidence-based practice have made recommendations pertaining to identification of at risk cancer patients and modification of risk factors based on the risk factors for falls in older people.11–14 However, it is not clear if risk factors for falls, the strength of their association, or the profile of reversible risk factors are the same in patients with cancer as in older people. To enable us to design effective interventions to reduce the risk of falls in patients with advanced cancer, we need to know what the risk factors and modifiable risk factors are in this population.
Our objective was to conduct a systematic review of published literature to identify research designed to (1) ascertain the risk factors for falls in adults with cancer or (2) demonstrate effectiveness of falls prevention strategies in this population. We wished to identify the extent and validity of current evidence, common challenges to researching falls in this population and to offer guidance, based on these, for researching in this area.
Methods
Criteria for selection of studies
Table 1 shows the criteria for selecting studies to be included in this review.
NHMRC, Australian National Health and Medical Research Council.
Search strategy
Electronic databases MEDLINE (1950 to third week of June 2010), Embase (“all years”) and CINAHL (1982 to June 2010) were searched. The final searches of the databases were carried out on June 30, 2010. See Table 2 for details of search strategy. All searches were restricted to studies of humans. “Falls” was included as a keyword in the MEDLINE and Cinahl searches in order to maximize the sensitivity of the search, albeit at the expense of specificity. Hand searching of the reference lists of relevant articles was also carried out.
Study selection
A single reviewer (C.S.) examined the titles of all retrieved articles and subsequently the abstracts of potentially relevant articles. In the next step, the full texts of all relevant articles were obtained. These were reviewed by both C.S. and P.L. Articles were excluded if they did not meet the criteria for selection of studies. See Figure 1 for more details of results of search strategy and study selection.
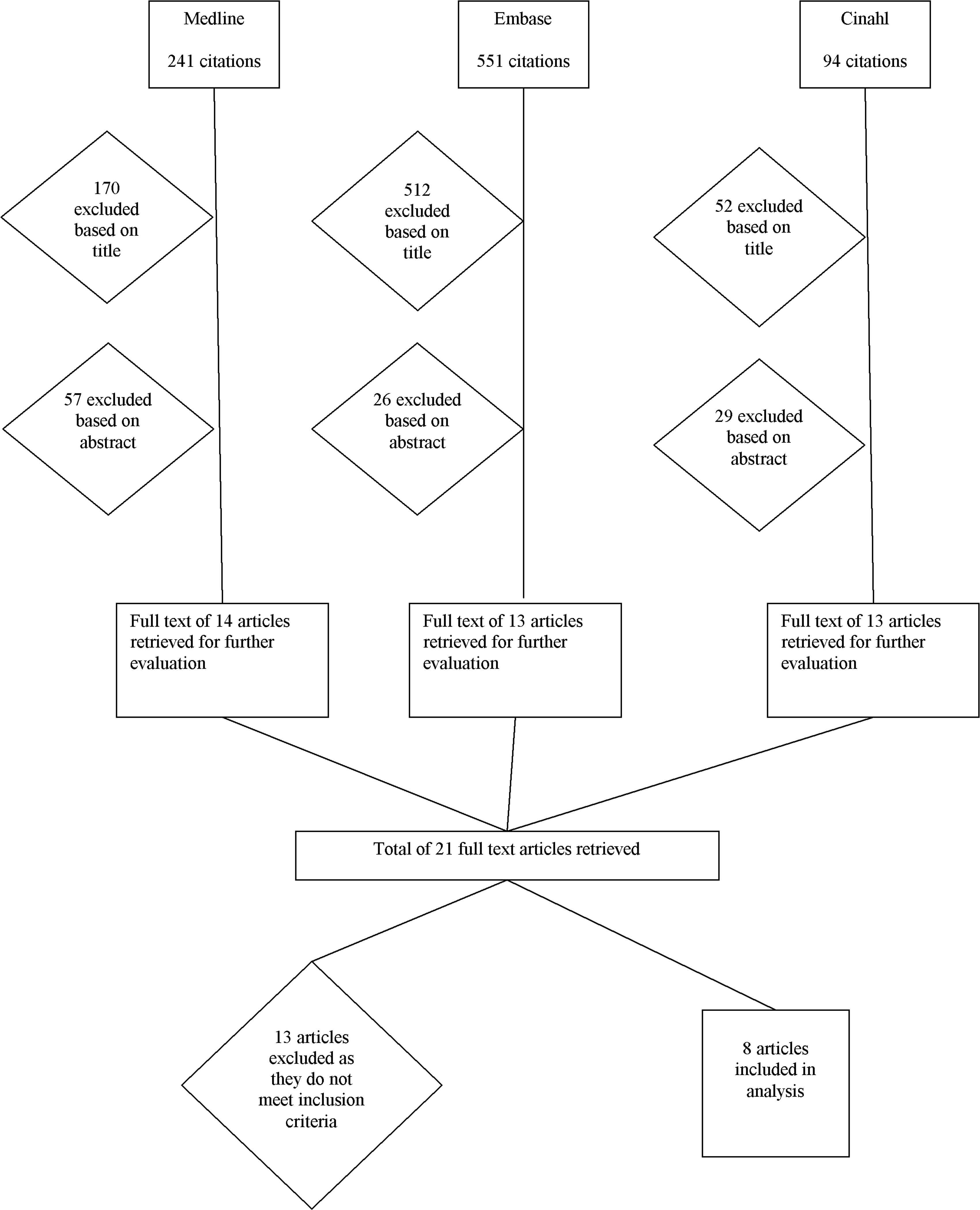
Results of search strategy and study selection.
Data extraction and quality assessment
Data were extracted from the reports of included studies on risk factors into a standardised table. Using the table, information from the studies was reported under the following headings: Publication details, Cohort details, Outcome measure used in analysis, and Risk factors identified. This was carried out by C.S. and verified by P.L. Further details pertaining to individual studies including those on variables measured in each study were included in a descriptive analysis.
The study design and the level of evidence of etiology that it can provide, as determined by the Australian National Health and Medical Research Council (NHMRC) was included in the data extraction table.15,16 An assessment of individual study quality was also conducted. The factors to be included in this assessment were selected based on their pertinence to the internal validity of studies that answer questions relating to risk factors and those that are most problematic in the area under scrutiny.
17
C.S. and P.L. independently assessed the quality of the included studies. The results were then compared and disagreements resolved by consensus. The following quality items were considered;
Has selection bias been minimized? Consideration was given to two particular sources of selection bias; nonrandom sampling bias and missing information bias. Nonrandom sampling can yield a nonrepresentative sample that generates parameter estimates that differ from the target population. Moderate to high levels of missing data can also introduce selection bias if participants with complete information are not representative of the total sample.
18
Has misclassification bias been minimized? Consideration was given to the validity and reliability of methods used to measure exposure and outcome variables, and the likelihood that misclassification may have resulted in an erroneous estimation of effect. Is the outcome measure valid? Consideration was given to whether the outcome measure and the corresponding method of analysis were appropriate. “Outcome measures” that occur prior to the measurement of the “exposure” or “risk factor” were not considered to be valid. Have adequate adjustments been made for strong confounders? The decision to regard a factor as a confounder should ideally be based on plausibility and prior evidence.
19
In the current context, knowledge of risk factors is limited. The options are, therefore, to adjust for confounding factors as identified in studies of older people, or to adjust for those factors shown in univariate analysis to have a substantial effect, regardless of p value, which may be large due to small sample size.
19
Data analysis
Data analysis was descriptive and includes analysis of the consequences of observed bias on the results obtained. Details of the studies of falls risk factors in hospital or hospice inpatients were analyzed separately from community-dwelling patients.
Description of studies
Seven studies that examined the risk factors for falls and one study of diagnostic accuracy of a screening tool for falls in patients with cancer were included, the first of which was published in 2002 and most recent in 2009. Of the studies to identify risk factors, four examined risk factors in hospital or hospice inpatients, and three studied outpatient attendees (Table 3). Studies of interventions to reduce falls risk in patients with cancer were identified but none met the inclusion criteria (Table 4).
NHMRC, Australian National Health and Medical Research Council; HR, hazard ratio; OR, odds ratio; BP, blood pressure; ECOG, Eastern Cooperative Oncology Group; COPD, chronic obstructive airways disease; ESAS, Edmonton Symptom Assessment Scale; IADL, instrumental activities of daily living scale; ADL, activities of daily living scale; GDS, geriatric depression scale; VES-13, vulnerable elders survey-13; ROC, receiver operating curve; TUAG timed up and go. √ = Yes, X = No).
Of the studies to identify risk factors for falls in patients with cancer in the inpatient setting, two were of prospective cohort design, one was a retrospective cohort study, and the other a case-control study.
Pearse et al. 9 studied the risk factors for falls in a prospective study of patients admitted to three palliative care IPUs within a cancer network in the United Kingdom. In addition to those variables detailed in Table 2, the following data were collected: gender, functional impairment, use of hearing aid, use of opioids, benzodiazepines, hypotensive agents, antimuscarinics and dopamine antagonists at time of admission, and the occurrence of a fall in the week preceding admission. Mean age was 67 years; 54% were female. Data pertaining to postural hypotension and impaired cognition were missing for 30% and 14%, respectively, of patients who did not fall. Statistical methods designed to control for the confounding effects of one or more than one variable were used; variables shown to be associated with falls in univariate analysis were entered into a logistic regression model. However, due to participants having variable lengths of follow-up, the logistic regression model, using “fall” or “no fall” as a binary outcome is not an appropriate choice; patients with longer admissions are “at risk” for longer. 31 Instead, survival analysis methods, such as the Cox proportional hazards model should have been used, using “time to fall” as the outcome measure.
O'Connell et al. 32 prospectively studied the risk factors for falls in consecutive admissions to oncology and palliative care wards in a private hospital. In addition to those variables shown to be associated with the occurrence of falls, as detailed in Table 2, the following data was collected: the occurrence of a fall in the preceding year, gender, blood pressure and hand grip, arm and leg muscle strength measured manually and scored from 1–3.
A total of 227 patients were recruited (mean age 67 ± 13.83 years). However, of the 34 patients who fell during the study, 18 fell prior to having the baseline research assessment. For these patients, data other than that routinely collected at admission (age, gender, cancer diagnosis, blood pressure on admission, and history of falls) was missing, thus making it likely that the estimate of effect of these variables was biased towards the null hypothesis. Conversely, nonvalidated tools were used to measure alertness and confusion and subjective methods used to assess muscle strength; any resulting misclassification bias involving these ordinal variables may have resulted in an away from the null bias, i.e., suggesting an association between the variable and falls where none exists. 18
In the study by Pautex et al., 33 the charts of all patients with advanced cancer hospitalised over a one year period were reviewed and the characteristics of those who fell during admission compared to those who did not. In addition to those variables shown to be associated with falls, as per Table 2, the following variables were examined; demographic details, Charlson Comorbidity Index, main medical diagnoses, Mini-Mental State Examination (MMSE), functional independence measure, incident comorbidities, hemoglobin concentration, administration of opioid, benzodiazepine, neuroleptic, antiepileptic, antidepressant, hypotensive, diuretic, respiratory system, corticosteroid and antibiotic medications, use of parenteral hydration or nutrition, and administration of palliative sedation. The occurrence of falls was determined using the institutional incident report forms. The mean age of participants was 71 ± 12.1 years; 59% were female. It was not apparent from the presentation of the results whether there were any missing data.
The criteria used to determine the occurrence of delirium or incident comorbidities during hospitalization were not specified, nor was it clear whether their occurrence preceded the fall in the patients who fell. Similarly it was not clear whether consideration had been given to the temporal relationship between medications used during admission and the timing of the fall in those who fell. If not, the direction of the observed association between falls and delirium and falls and the use of neuroleptic medications cannot be ascertained. Patients had differing lengths of follow-up corresponding to length of admission. As per the study by Pearse and colleagues, logistic regression, rather than survival analysis techniques, was inappropriately used to adjust for confounding.
Goodridge and Marr 34 conducted a retrospective analysis of falls that occurred in an IPU during 1999. The mean age of patients admitted was 70.9 years, 53.2% were male, and 0.3% had a noncancer diagnosis. Univariate analyses were conducted to investigate relationships between the occurrence of one or more falls during admission and gender, age, duration of stay, and diagnosis using data from all admissions. Male gender, increasing age, and longer stay were associated with falls. Cognition (measured using MMSE), symptom severity measured using the Edmonton Symptom Assessment System (ESAS) and medications on admission were compared between those who fell once and those who fell more than once during admission. There were significant levels of missing MMSE (37%) and ESAS (11%) data. While ESAS scores were observed to be higher in those who fell once than those who had repeated falls, age was inversely related to total ESAS scores and hence a potential confounder given the observed correlation between increasing age and falls.
Three studies examined factors associated with falls in patients with cancer attending outpatient clinics. In two of the three35,36 patients with cancer at any tumour stage were included, while in the study by Bylow et al., 37 patients with symptomatic metastatic disease were excluded. All three used convenience sampling and were therefore subject to nonrandom sampling bias. The studies were cross-sectional in design, collecting information from each subject at one point in time, but used a retrospective question, i.e., have you fallen during the past 3/12 months, to ascertain the “outcome.” As a result the outcome preceded the “exposure,” the study design therefore facilitating identification of the sequelae of falls rather than risk factors for falling. See Table 5 for details of incidence of falls reported in included studies.
Quality items reflecting consideration of important sources of bias in studies of diagnostic accuracy were used to assess the study by Overcash and Rivera, 17 whereby two instruments were administered to older persons with cancer, in order to establish their accuracy in predicting which patients had fallen. Critically, the utility of determining the accuracy of a test in predicting a past event is not clear. A useful lesson from this study is the susceptibility of retrospective reporting of falls to recall bias; 13 of the 20 patients reported having fallen within the preceding year, while 15 reported having fallen within 3 months.
Discussion
This literature search identified seven studies that aimed to investigate the risk factors for falls in patients with cancer. Upon critical appraisal all were found to have significant methodological limitations, precluding the generation of a new synthesis from this review, but highlighting important design and statistical issues pertinent to epidemiologic studies in this area and the need for further research. Limitations of this review include incomplete searching of the gray literature, limited hand searching for articles, and inadequate definition of cohorts in individual studies, particularly regarding stage of disease.
Evaluation of the cross-sectional studies of community dwelling persons highlights the inherent unsuitability of cross-sectional study design to answer this particular research question, due to the impossibility of determining whether observed impairments in functioning or physical or psychological health have predisposed to falling or resulted from it.
Going forward, researchers aiming to identify the risk factors for falling in this patient population should use validated tools to measure exposure variables, reliable methods to ascertain the occurrence of falls and attend to the temporal relationship between the two. Additional plausible exposure variables such as measures of sarcopenia, fluid deficit, and vitamin D deficiency should be included.
Studies of risk factors that do not control for strong confounders are of restricted value due to the potential for spurious results. 17 However, in areas where there is limited knowledge of risk factors and hence confounders, preliminary investigations that utilize univariate analyses can usefully highlight variables to be included and controlled for in analysis, in subsequent studies. From the studies in inpatient settings, the following variables were not exposed to significant misclassification bias and were found to be associated with falls in univariate analysis; age,9,32,34 low blood pressure, visual impairment, cognitive impairment, 9 performance status, fatigue, 32 and male gender, longer stay and low total ESAS score. 32 Establishing the relationship between medications and falls is particularly challenging due to the potential for confounding by indication, whereby the condition for which the medication is prescribed is itself associated with increased falls risk, e.g., neuroleptic medication and delirium. Alternatively, confounding by contraindication may result in erroneous observations as highlighted by Pearse et al. 9 ; in univariate analysis of their data, use of opioid medication was associated with lower risk of falling. They speculate that this may have resulted from clinicians preferentially using alternative analgesia in cognitively impaired patients for fear of exacerbating confusion. Agostini and Tinetti 38 caution that careful consideration should be given to baseline medical characteristics that may influence medication choice and indications for medications, which should be adjusted for in multivariate analyses.
Future research must use suitable statistical methods to adjust for confounding variables; in studies where duration of follow-up varies, survival analysis models using “time to fall” as the outcome measure are appropriate. Alternatively, models that facilitate analysis of recurrent falls and accommodate variable follow-up, such as negative binomial regression or the Andersen-Gill model may be used; in trials of falls prevention interventions, methods for analyzing recurrent events are preferable to time to first event analysis. 39 The effect of incident illnesses, whether or not risk factor profile differs between older and younger people with advanced cancer, and the physical and psychological sequelae of falls in this population are also worthy of investigation.
Ten studies of interventions to reduce falls risk in patients with cancer or cancer survivors were retrieved, but none met inclusion criteria. The described interventions included strategies to reduce falls rates in inpatient oncology settings by raising staff awareness of falls risk factors, attending to environmental hazards and procedural initiatives such as increased frequency of nurse rounds. The effectiveness of such initiatives, targeted at health care professionals, merits further careful evaluation.
In summary, findings from the small number of studies that used random-sampling techniques, suggest that patients with cancer have a high risk of falling. Further research is required to determine the principal risk factors for falls in patients with advanced cancer. This will facilitate identification of patients at risk, subsequent development of strategies to reduce risk and informed decision-making regarding use of any medications shown to increase falls risk. The challenge is to determine the interventions which reduce the risk of falling and augment rather than compromise quality of living for patients with advanced cancer.
Footnotes
Author Disclosure Statement
This research was supported by the Health Research Board and Irish Hospice Foundation through the Palliative Care Fellowship awarded to C.S. (HSR/2008/17). None of the authors have a relationship with any entities that have a financial interest in this topic.