
Abstract
Abstract
Background:
A large tertiary hospital in central Georgia has found a novel approach to hospital palliative care.
Approach:
It is unique in that the approach has a strong counseling base in providing the palliative service, rather than major reliance on advance practice nurses or palliative physicians. The Medical Center of Central Georgia employs master's prepared counselors who spend the hours needed to assist families in making difficult end-of-life decisions.
Model:
Using a family systems therapy approach, these counselors have developed the Transitions and Palliative Care Therapy Model, which has proved to be a successful means of providing the services. The model includes the “7 Core Components of Communication and Decision Making,” which gives the counselors actual interventions to use in working through these complex cases.
Outcomes:
The growth of the program over 7 years is staggering with the outcomes far exceeding even the predicted volume from the Center to Advance Palliative Care.
Conclusions:
The model has the counselor at the heart of the team, keeping the communication open and flowing. The Transitions and Palliative Care Therapy Model has become an accepted standard of practice at Medical Center of Central Georgia and continues to be a successful means of managing the most complex cases in the hospital.
Introduction
Most hospital-based palliative care programs have adopted models where the key members are either advance practice nurses or physicians.2–8 A multidisciplinary approach has been recommended with “a medical staff leader, a nursing leader, a medical social worker, a pain management specialist, a pastoral care representative and an administrator being the minimum team members.” 9 Early psychosocial interventions can be offered by palliative care counselors or pastoral care that can facilitate communication with nurses and physicians. 10 “The ultimate goal of palliative care is improving the overall quality of care for patients with serious illness and their families.” 11 How each hospital accomplishes this goal varies from one organization to another.
We report a 7-year experience of delivering competent palliative care to hospitalized patients through a patient-centered, interdisciplinary approach, relying on family systems therapy integration into standard medical practice. 12 This mode of delivering palliative services, called the Transitions and Palliative Care Therapy (TPCT) Model, has been field-tested with over 10,000 hospitalized patients since its inception in 2004. The TPCT Model was built on the foundation set forth in the National Consensus Project (NCP) 2004 Clinical Practice Guidelines for Quality Palliative Care and revised in 2009.13,14 It is unique in that the model has a strong counseling 10 base in providing the palliative service, rather than major reliance on advanced practice nurses or palliative physicians.2–8 The model consistently diminishes potential for conflict, communication deficits, time constraints, and knowledge gaps.
Approach
The Center for Palliative Care (CPC) is part of the Medical Center of Central Georgia (MCCG), a 603-bed nonprofit teaching hospital located in central Georgia. The CPC has three distinct components: the Palliative Consult Service; a 5-bed inpatient palliative care unit; and transitions counselors.
The Palliative Consult Service responds to a consult order written by an attending physician, with 90% of initial palliative consults being completed by midlevel providers. Full-time members of the Palliative Consult Service include a nurse practitioner and a clinical nurse specialist, both of whom are certified as advance practice hospice and palliative nurses. Part-time members include two physician assistants with specialization in geriatrics. The midlevels collaborate with two part-time hospice and palliative medicine certified physicians and consultative services such as chaplains, speech therapists, hospice nurses, and case managers. Palliative Consultants always work in tandem with the Transitions Counselors' evaluation of the family dynamics.
The second component is a 5-bed closed unit available if a palliative consult has been completed and the clinician determines a need for admission to the palliative unit. 15 The goal of care in the unit is acute pain management or symptom control, a more suitable environment for end-of-life care/inpatient hospice or a transition from curative to comfort based care. Palliative care standing orders are available for the nursing staff on this unit. Patients are referred by physicians from all over the hospital such as the intensive care units, emergency department, general medical floors, and various specialty areas. 16 Nurses and administrators on this unit are trained in palliative care and critical care. The unit specializes in quality end-of-life care.
The third key component of the CPC is Transitions, which consists of eight full-time master's prepared Transitions Counselors (from schools of Family Therapy and Counseling) who make initial contact with patients suffering from severe chronic disease or terminal illness. Referrals to the Transitions service can be initiated by anyone in the hospital. Most often referrals come from a nurse or physicians, but even a family member may ask for the service. Transitions counselors meet the psychosocial needs of patients and families within the hospital setting through medical family therapy. Throughout this article whenever “family” is mentioned, it includes the patient and family members, unless specifically indicated otherwise.
Transitions counselors are trained to provide critical services in a medical facility helping families navigate complex systems. Counselors attend weekly Interdisciplinary Palliative Rounds to increase their knowledge of medical issues related to the palliative patients. The counselors are integrated into the intensive care units (ICUs) and medical–surgical units through rounds where they receive pertinent information on specific disease processes and treatment options. The palliative medical director provides oversight to the Transitions counselors.
The palliative care team is thus composed of 8.0 FTE counselors, 2.5 FTE midlevel practitioners, and 0.5 FTE palliative physicians. The large majority of patient and family contacts, including family meetings, are initiated by counselors, allowing the midlevels and physicians to concentrate on biomedical issues and provide overall medical supervision.
MCCG supports the 2009 NCP recommendation for timing of palliative care to “begin at the time of diagnosis of a life-threatening or debilitating condition and continue through cure or until death and the family's bereavement period.” 13 This referral system provides interdisciplinary access sooner to more patients with life-limiting or severe chronic illnesses. 17 The focus of earlier intervention is on educating families about disease trajectory, coordinating multiple physician views, and collaborating with outpatient services. Collectively, this promotes continuity of care.
The 2009 NCP Clinical Practice Guidelines for Quality Palliative Care emphasize that all evaluations and interventions should be patient-centered, incorporating at all levels of the illness the central role of the family unit in decision making. 13 The Transitions counselors achieve this through a systems therapeutic approach in addressing the uniqueness of each case. Part of the master's training of these individuals focuses on the reality that when patients enter the hospital for care, they do not come alone. Most patients bring with them functional or dysfunctional family systems. Families are likely to be symptomatic when going through a transition, such as complex medical decision-making and facing the impending death of a loved one.
Model
Transitions counselors have developed the Transitions and Palliative Care Therapy Model (TPCT; Fig. 1), which focuses on “
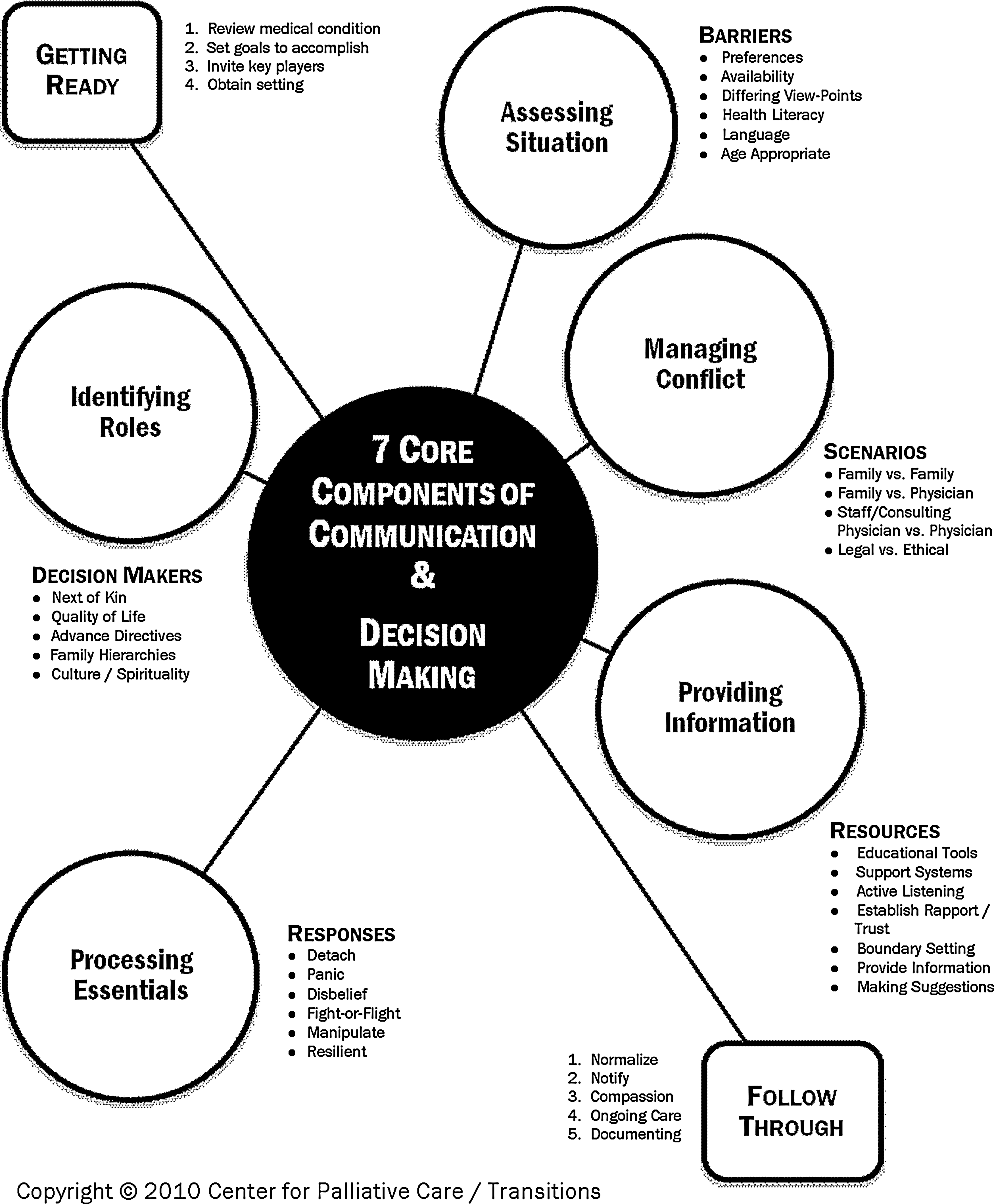
Transitions and palliative care therapy model.
Transitions counselors address each one of the complex cases, working through all of the interrelated subsystems. 18 These subsystems include the hospital system with its rules and regulations, the many different consulting physicians focusing on their specific areas of expertise and the family unit. Physicians also respond personally with their own emotions, values, beliefs and cultures. Families tend to respond best to a system that has clear boundaries, rules and messages, but in the complex health care system, this is difficult to control. Physicians and nurses often have neither the time nor training to navigate this complex emotional, cultural, and spiritual system. The TPCT model of patient-centered care enhances interactions among providers, departments, and health care settings.
Getting ready
Before meeting with a family, there is preparation needed in order to “Get Ready” for whatever the family may have on their agenda. The Transitions counselor reviews the medical records and speaks with the health care team members to determine whether there is a consensus by the medical professionals on the patient's overall condition. If there are discrepancies, the counselor will make verbal contact with physicians both consulting and especially the attending, to get clarification. Goals are set for the discussion before meeting with the family, but keeping in mind that the family may have their own goals. It is central to keep in mind that TPCT is a “communication” model. Keeping in touch with the attending and other members of the clinical team, is key to fostering transparency among the team and with the family. It is important for the clinical team to be on the same page when talking with family members. The counselor will invite key members of the health care team, family members, and family support systems to the meeting. The counselor's role is to coordinate, act as mediator, and keep the meeting running smoothly. By considering what information and decisions need to be made, the counselor can keep on track despite the families' attempts to deviate. This provides the clinical team the time to focus on providing critical information about the patient's medical condition. Once this information has been shared, the clinical team is able to exit the meeting and leave the counselor to assist the family in processing this information. Often times there are follow-up conferences with the attending physician. This insures communication of any family concerns with the attending. It also assures the counselor is in sync with the attending.
Assessing situation
The Transitions counselor begins additional interventions with his/her goals in mind but remains flexible to what the family may need. The counselor allows the family to tell the story of the illness 4 and their understanding of the previous discussions with physicians. Focus is on joining the family 18 and earning their trust by naming the emotions that they seem to be feeling (i.e., overwhelmed, angry, and frustrated). The counselor, keeping patient autonomy in mind, advocates for good communication about choices for medical care. If there seems to be any misunderstandings, the counselor will arrange additional meetings with the appropriate clinician. This leads to more informed decisions. It is important to recognize and address any barriers to communication (Table 1).
Identifying roles
Families are organized with hierarchies and subsystems18,19 that make each unique. When faced with complex decisions, families work around or through unresolved stressors that existed before the patient entered the hospital. These unresolved stressors, coupled with an unfamiliar environment and anticipatory grief, often result in chaos. Many times health care members find themselves caught in the middle of these unresolved issues, resulting in distress and burnout. Transitions counselors assess the family dynamics, hierarchies and subsystems, and how the patient's hospitalization affects this structure. New roles may have to be clarified and agreed upon in order to move forward with any decision making. Transitions counselors arrange family meetings to avoid coalitions and triangulations, 20 giving every family member a chance to speak up.
Through regular family meetings and ongoing documentation of family dynamics, Counselors facilitate effective decision making among family members (Table 2). Families are guided through the often confusing health care system and are proactively encouraged to request physician meetings or to list their questions in order to promote communication. Physicians specifically benefit because Transitions counselors are able to spend the minutes to hours required to identify the key decision makers, assess cultural or spiritual issues, establish rapport, and address baseline questions. Counselors identify family dysfunction and how it directly affects their ability to make decisions about patient goals-of-care. When the physician or nurse begins to discuss medical details, much of the conversation builds on the framework already developed by the Counselors.
Providing Information
One of the most important aspects of palliative care is assisting the family in making informed decisions, including pros and cons of treatment options and likely progression of the illness. Physicians explain complex medical conditions using terms that many families may not understand. The counselor spends the time with the family in order to identify the best ways to communicate with them, knowing there are many different ways that individuals retain information. Transitions counselors use appropriate resources to ensure the families have what is needed to make these informed decisions (Table 3).
Processing essentials
When the patient shows signs of terminal decline, symptoms of grief may inhibit the families' comprehension and decision-making abilities. The Transitions counselors have recognized several responses to grief that are common in these situations (Table 4). They gain the trust of the families by joining in their family system and assisting them in mentally and emotionally processing the information given by the medical team. Through this rapport-building, they often become a trusted precursor to the Palliative Consult Service. The hospital medical staff comes to rely on the counselors to know when it is the best time to share bad news or make decisions.
IDT, interdisciplinary team.
Managing conflict
The situations that are faced in palliative care can be very stressful on patients, families, healthcare staff, and clinicians. There can be conflict between the clinician and family, within the family, between healthcare staff and the clinician, and between clinicians themselves. The TPCT Model addresses these conflicts as one of the “7 Core Components of Communication and Decision Making” (Table 5). The Counselors have all received extensive training in managing conflict through their master's programs. Systems Theory is used on a daily basis to maneuver through all of the various conflicts that arise from such complex cases. It is important to remember that there are also legal and ethical factors (Table 6) when dealing with conflict. There is no one right answer to every case, but the counselor will assist the health care team in finding the middle ground to work toward a compromise. “Law provides guidance through various sources, but does not provide the answer.” 21
TPCT, Transitions and Palliative Care Therapy Model.
Follow through
After bad news is shared by clinicians, Transitions counselors assess whether the family has accepted the information and able to make decisions on appropriate goals-of-care. If the family is not able to accept the impending death, counselors move toward discussing long-term goals-of-care, which include discussions on quality of life. If the family does accept end-of-life care, counselors assess the family's feelings of guilt and reassure them by providing education on the signs and symptoms of nearing death. The goal of therapy at this stage is to normalize these feelings. 22
The Transitions counselors keep all other health care team members notified of any changes and introduce new team members in order to keep trust between family and staff. The plan of care is clearly documented to minimize confusion between care team members. Once the patient dies, the counselor will make a follow-up call to the family to initiate the CPC Bereavement Program.
Outcomes
Since the initiation of the program, it was evident that actual data tracking was important to consistently report to hospital administration the success of the palliative team and the TPCT Model. 23 CAPC has provided the means to estimate program volume that takes into account the hospital's average length of stay, frequency of deaths and patient mix. 24 The CPC has proven its success and sustainability with exceeding the CAPC estimated volume of 338 potential referrals by actually receiving 751 referrals in the first year of operation. The team uses a database that keeps actual outcomes of the program at their fingertips making it easy to report to administration on a regular basis (Fig. 2). Growth has continued due to the obvious needs of the patients at MCCG and the physicians' realization of the team's skills. 24 MCCG has many specialized physicians, being the second largest hospital in Georgia, that bring many complex cases needing the services of the palliative team.
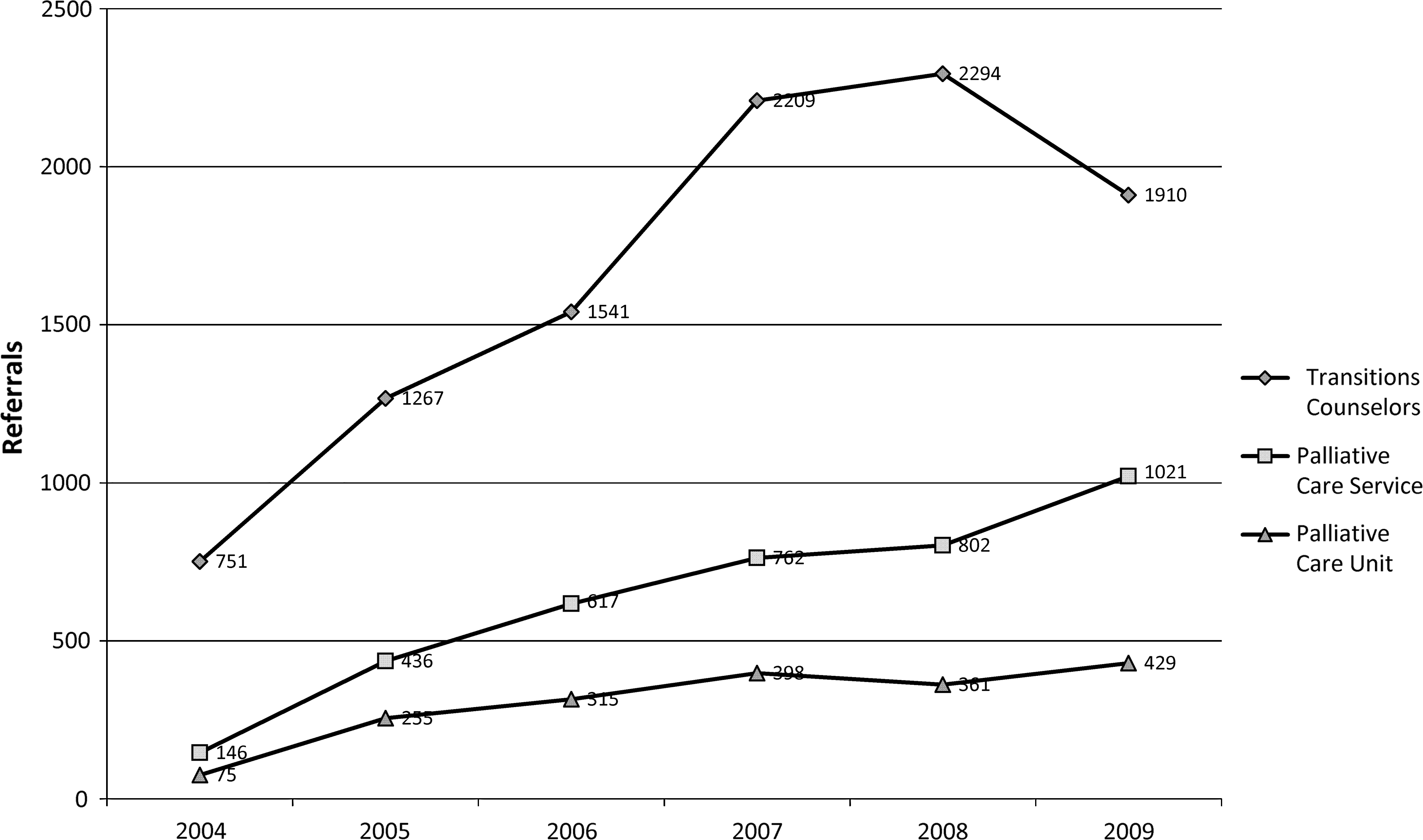
Palliative care growth, 2004–2009.
The TPCT model with the use of counselors has allowed early access to patients in need of services. The CPC department has 8.0 FTEs Transitions counselors, 2.5 FTEs midlevel providers, and 0.5 FTE palliative physicians. This staffing distribution is strikingly different from most published inpatient palliative models,2–8 which have a stronger focus on the physician/NP/PA team members. Despite the U.S. economic hardships in the last few years, the palliative team has continued to prove its value to the hospital organization.
Conclusion
The TPCT model has the counselor at the heart of the team, keeping the communication open and flowing. The specialized training that the counselors receive is based on a systemic approach where all parts of the interdisciplinary team and the patients' families and support systems are collaborating to make the difficult decisions involved at the end of life. This TPCT model appears to be a cost-effective way to provide palliative services, using counselors who are hired at a much lower cost than clinical staff. This model has attracted interest from other hospitals and is now being replicated at various sites. The Transitions and Palliative Care Model has become an accepted standard of practice at MCCG and continues to be a successful means of managing the most complex cases in the hospital.
We have presented a novel approach to having counselors in a strategic role in a hospital palliative care team. The purpose of this article has been to present our unique model. Our intention is to have an additional article to present the data that has resulted from this approach.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Additional Resources
Rolland JS: Families, Illness, & Disability. New York: Basic Books, 1994.
Nichols MP, Schwartz RC: Family Therapy: Concepts and Methods, 2nd ed. Boston: Allyn & Bacon, 1991.
McDaniel S, Hepworth J, and Doherty WJ: Medical Family Therapy: A Biopsychosocial Approach to Families with Health Problems. New York:
Basic Books, 1992, pp. 61–93.
Kübler-Ross E: On Death and Dying. New York: Scribner, 1969.