
Abstract
Abstract
Background:
Communication is an ongoing challenge for clinicians working with people facing life-threatening illnesses and end of life. Family conferences offer patient-focused, family-oriented care that brings together patients, family members, and health care providers.
Objective:
The aim of this study was to develop a research-based model for family conferences to help physicians and other health care providers conduct such conferences effectively and improve communication with patients and families.
Design:
We prospectively studied family conferences for patients facing life-threatening illness in two inpatient medical centers. We videotape and audiotape recorded real-life conferences and postconference interviews with participants.
Participants:
Twenty-four family conferences were included in the study. Participants consisted of 24 patients, 10 of whom took part in the family conferences, 49 family members, and 85 health care providers.
Approach:
A multidisciplinary team conducted a qualitative analysis of the videotaped and audiotaped materials using thematic analysis. The team used a multistage approach to independently and collectively analyze and integrate three data sources.
Main Results:
The resulting theoretical model for family conferences has 4 main components. These include the underlying structural context of conference organization and the key process components of negotiation and personal stance. Emotional engagement by health care providers, emotion work, appears central to the impact of these components on the successful outcome of the conference. In addition to the theoretical model, the authors found that family conference participants place specific value on the “simultaneous presence” of conference attendees that leads to being on the “same page.”
Conclusions:
Physicians and other health care professionals can use the model as a guide for conducting family conferences and strengthening communication with patients, families and colleagues.
Introduction
Family conferences, also called family meetings, offer an opportunity for patient-focused, family-oriented care that brings together patients, family members, and health care providers. They are valuable clinical interventions desired by both professionals and patients in the settings of life-threatening illness and end-of-life care, and they positively impact the care experience of those involved, as demonstrated by the randomized controlled trial conducted in the intensive care (ICU) setting.25–30 Research on palliative care family conferences in the ICU has provided a mix of setting-specific and setting-transferable information.31–34 The current study, conducted solely on medical wards, is unique in applying audio and visual methods to build a model based on direct observation and participants' discussion of their perspectives.
The aim of this study was to examine family conferences in the clinical setting to inductively develop a research-based theoretical model for family conferences to help health care providers plan and lead such conferences effectively. The study focused on elements of the family conference process and participants' priorities. The study did not aim to investigate conference topics, participants' characteristics, or quantifiable outcomes. Rather, participant-generated data and direct observation were used to identify what made conferences helpful and successful.
One practical challenge is the lack of definition of “family conference” as it applies to the inpatient medical setting. Literature suggests that such conferences are one-time meetings attended by the patient (when possible), family members, and health care providers to discuss the patient's illness, treatment and care; conferences are not family therapy.28,35–40 Although they are one-time meetings focused on a specific topic, several conferences may take place during the course of a patient's illness. 41 Family conferences have a range of functions and are valuable for facilitating communication, enhancing family inclusion, promoting interdisciplinary coordination, exchanging and sharing information and negotiating decisions.19,38,42–45 They are opportunities for first-hand communication among the people most involved in patients' lives and apply across the trajectory of palliative care, from time of diagnosis through end of life and bereavement. Conferences may address any topic and are regularly used to discuss diagnosis, prognosis, treatment options, care and resuscitation preferences, and end-of-life care decisions.46,47
Methods
The research team was led by a clinician–researcher with no clinical relationship to the study settings. We collaborated with medical ward and palliative care teams at two medical centers in Southern California to prospectively identify inpatient family conferences for seriously ill patients with an estimated life expectancy of 6 months or less. The purposive sampling did not include eligibility criteria regarding the patient's diagnosis or the conference topic because these were not focal to the study. Family conferences were defined for the study as preplanned meetings that include at least three people. Preplanning, even by a few hours, was a requirement in order to distinguish conferences from coincidental or informal contact with the family. Patients and families were invited by the hospital-based health care providers to be in this qualitative study. Those who agreed to be contacted by the research team were reached by telephone or in person for study participation. Patients or their representatives had to give permission for inclusion of the conference in the study prior to other family conference participants being approached. Written consent for participation in the study by all conference attendees was obtained prior to videotaping or audiotaping of the family conference.
Family conferences were videotaped and audiotaped on location at the hospitals, in the rooms usually used for such meetings. Videotaping enabled examination of social interaction and organization within conferences. 48 Face-to-face semistructured interviews conducted by the research team following the conference invited participants to reflect on and discuss positive and negative aspects of the conference as well as offer recommendations for conference improvement. Patients and family members were interviewed separately from staff, although interview questions were similar. Interviews were conducted and audiotaped in a quiet, private space. Audio from the family conferences and postconference interviews was professionally transcribed and anonymized for qualitative data analysis. Institutional Review Board (IRB) approval was obtained from all institutions involved in the research.
Data analysis
Data included videotapes and written transcripts of the family conferences, and written transcripts of postconference interviews. Utilization of these three distinct but overlapping data sources was chosen to triangulate the data and strengthen the research design.49,50 Atlas.ti computer software, designed for managing qualitative videotape and audiotape materials, facilitated data analysis. 51 A multidisciplinary team of researchers from anthropology, social work, sociology, and medicine, conducted the qualitative analysis. Professionals with clinical and non-clinical backgrounds were involved.
A modified grounded theory approach was used to analyze the data. 52 The multistage iterative analysis process began early in data collection, informing the data collection process, and concluded after data gathering completion. Data analysis team members independently conducted line-by-line analysis of the written transcripts, initially using in vivo codes based on the interview questions and then applying open coding.52,53 Analysis of the conference transcripts and videos involved open coding exclusively.
Themes and subthemes were identified, subjected to constant comparison methods and iteratively reconfigured throughout analysis. 54 To facilitate and document the coding process, control for research bias, and increase reliability within the coding team, we used standard techniques to develop a codebook.52,55–57 Data analysis team members coded data separately and met regularly to develop and refine the codebook and the theoretical model. The distinct analyses of the conference transcripts, conference videos, and postconference interviews were integrated to achieve the final model.
Results
Conferences and participants
Twenty-four family conferences were studied from July 2005 to March 2006. Eighteen of the conferences were videotaped and audiotaped, 5 were audiotaped only, and 1 included only postconference interviews. Postconference interviews were conducted for 21 of the 24 conferences. Family conferences were for 24 patients aged 56–90 years (mean 74.3 years), of whom 87.5% were male. Seventy-five percent of the patients had a cancer diagnosis.
Patients participated in 42% of the family conferences. The conferences had a mean of 2 family members (range, 1–6) and 4 health care professionals (range, 1–11) with a total of 49 family members and 85 professionals participating in the study. However, the majority of postconference interview participants were family members. Health care professionals in the conferences included physicians, nurses, social workers, and case managers; the majority of professionals interviewed postconference were physicians.
Family conference model
We integrated analysis of the conference and postconference data to develop a theoretical model for family conferences (Fig. 1). The data suggest four major components that influence the conference: conference organization, negotiation, personal stance, and emotion work.
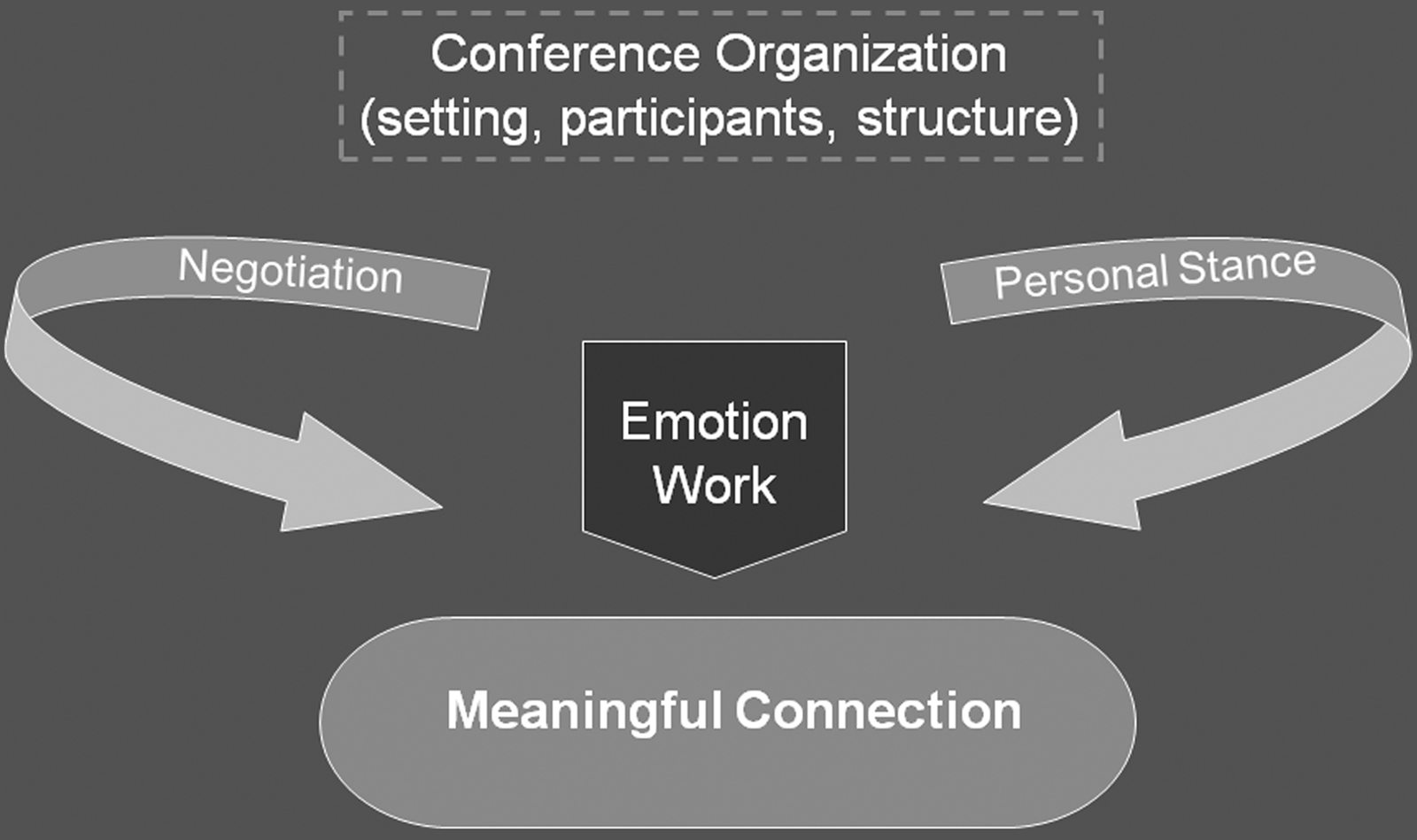
Theoretical model for family conferences.
Conference organization is the underlying base of the model. It is the background to what takes place in the meeting but is not the most critical part of the model. Conference organization includes the setting (Fig. 2A), participants (Fig. 2B), and structure (Fig. 2C). The setting includes elements such as room size, seating, and comfort. Physical landscape choices consider room size in proportion to participant numbers, sufficiency and configuration of seating, and promotion of participants' comfort. Providers standing over family participants may create power dynamics that interfere with the conference process, while rooms with comfortable chairs and pleasant décor provide a supportive setting.

Elements of conference organization.
The participants component of conference organization refers to who is included in the meeting (Fig. 2). All people who are relevant to the meeting should be there to allow for a “simultaneous presence.” For professionals, this may mean inviting consultants or members of the team who know the patient/family well. For family participants, patients should usually determine who is invited to attend. One of the strongest concepts to emerge from the data—from patients, families, and health care providers—was the importance of people being on the “same page” as a result of being present in the same place and at the same time to experience the exchange. Specifically, participants indicated that telling someone about what happened in the meeting was not sufficient and did not fulfill the valued state of being on the “same page.”
The final organizational component is the conference structure which refers to the phases of the meeting (Fig. 2). It guides how to procedurally conduct a conference but is not linear or prescriptive. Structural elements are part of the background organization rather than its central components. Conference goals and participants will influence which structural elements are included and in what order. The following examples demonstrate the structural elements:
Example 1 (Agenda Setting)
Doctor: I wanted us to sit down to talk a little bit about what happened that brought us to the place that … where we are now, sitting and having this discussion. But also about where we go from here.
Example 2 (Diagnosis/prognosis)
Doctor: You know listening to how you were talking about how that affected you and looking at you and I've always said I'll let you know. And I think we're coming to the point of the balance where the treatment's doing more harm than good.
Patient: Yeah.
Doctor: And that's the impression I'm getting and that you might actually do better if we stop treating the cancer and just let you be.
Patient: And I counted on you for that. You told me that you would …
Doctor: I would tell you, yeah.
As visible in Figure 1, negotiation is one of the key process components of an effective family conference. In these meetings, negotiation refers to the exchange process for reaching a decision and building consensus. Negotiation may occur between any combination of participants and commonly around topics such as perspectives on the patient's situation, care goals, and discharge plans. The following is an example of negotiation:
Example
Doctor 1: Okay. Do you ever talk to S?
Doctor 2: Not very often. I don't know her well, but there are a couple of other pulmonologists that I work really closely with. I can call her if you like …
Doctor 1: Yeah.
Doctor 2: … and get her opinion. And if she feels … You know, if she says, yes, it's going to prolong the dying process …
Doctor 1: Yeah.
Doctor 2: … we'll definitely …
Doctor 1: We'll have to go a different route …
Doctor 2: Absolutely.
Doctor 1: … go a different route. Okay.
Doctor 2: If she feels that it's going to enhance her breathing, as we seem to, then of course we would keep it.
Doctor 1: Okay. That's all I want, yeah. I feel comfortable with it.
Negotiation in the family conference is an important process component of understanding and decision making.
Personal stance, the second key process component, refers to behaviors and personal presentation that health care providers display during the conference. Stance focuses on the attitude and mode of delivery that are conveyed. Active listening behaviors such as appropriate eye contact, head nodding, and attentive body language are positive exemplars of personal stance. Behaviors and attitudes that convey empathy and respect enhance personal stance.
The family conference model suggests that the contribution of negotiation and personal stance is mediated by the key component of emotion work. Emotion work refers to health care providers' emotional engagement with themselves, the participants and the content of the family conference. It demonstrates providers' willingness to venture into the emotional realm of the patient/family experience. Actions of this emotional labor include helping patients and family members to manage uncertainty, asking about emotions, empathically acknowledging the difficulty of illness and end of life, or engaging in self-awareness about one's own emotions. It invites the emotional aspects of care that may be painful but essential, reflecting genuine interpersonal engagement.
Conducting family conferences that include emotion work does not require health care providers to be experts in psychosocial care or mental health, but inclusion of team members with such expertise, such as social workers, psychologists, and pastoral care providers, is extremely valuable to the conference. 58 Engaging in emotion work reflects the distressing emotions encountered in serious illness but also the joys and humor that patients and families experience. The following are examples of emotion work in the conference:
Example 1
Doctor: I know this is hard to hear, but—I'm concerned that, that there may need to be someone really there for you most of the time.
Example 2
Family member: Well, she has malignant tumors that cannot be cured and it looks like the treatment isn't … is maybe not worth doing because of the pain she goes through for the treatment. And you're suggesting that she will have like six weeks to three months to live, and perhaps just to keep her comfortable would be the way to go from now till she dies.
Doctor: That's a very clear statement of what took us awhile to get to that point … that you've handed it over really clearly. [Doctor turns to the patient] How does it make you feel to hear somebody else say that?
Patient: Like it's somebody else they're talking about.
Emotion work during the family conference appears to function as a crucial gatekeeper to achieving the desired outcome for the meeting.
We have named the outcome of the family conference as meaningful connection. The name reflects the centrality of the relational processes in achieving success in these meetings. Since family conferences serve a broad range of functions, the ideal outcome enables this range to be achieved at the highest level of quality. Achieving a meaningful connection among family conference participants reflects a successful process of communication intended to enhance the quality of the patient/family experience.
Discussion
Communicating with families can be an intimidating prospect, especially for professionals with minimal training in working with families. Family conferences are a valuable tool for communicating with patients and families facing life-threatening illnesses and end of life. This study explored what makes family conferences helpful and successful based on direct observation of naturally occurring conferences, as well as the perspectives of patients, family members, and professionals. Our family conference model provides a theoretical framework to clinicians for conducting family conferences, combining information about structural components for conference planning and process components for allowing the optimal conference experience.
The unique use of videotaping enabled us to study real family conference interactions, in conjunction with firsthand feedback from the participants. 59 The rigorous qualitative analysis of multiple data sources by a multidisciplinary research team led to a cogent theoretical model for family conferences. The model reflects the organizational and structural components—the “who, what, where” aspects of conference planning—but illuminates the centrality of the relational processes in these meetings.
The opportunity that family conferences offer for bringing people to the “same page” regarding the situation and care of a patient is invaluable. The term “same page” was used by family members and professionals alike, both emphasizing its critical importance. The distinction of people being present at the conference to experience the “same page” communication was noted as essential and incomparable to people simply hearing about the family conference discussion.
Perhaps the most challenging element of the theoretical model to put into practice is emotion work. Medical education has traditionally socialized physicians towards limited emotional engagement with patients and families, creating a tension between demonstrating compassion and protecting oneself from the emotional strains of caring. 60 However, responding to emotions is one of the core functions within patient–clinician communication that overlap to affect health outcomes, 61 and our respondents were clear that it was crucial to the successful conduct of a family conference. The importance of emotional engagement for constructive conference outcomes has been noted in guidelines, based on literature review and expert opinion, developed for family meetings in palliative care. 62 A randomized controlled trial of ICU patients' family members' bereavement demonstrated the benefit of a model that acknowledges family members' emotions. 30 Our study provides audiovisually based empirical evidence that reinforces the need for palliative care providers to engage with families' and professionals' emotional elements of the family conference. Furthermore, our theoretical model places emotion work centrally in relation to other aspects of the conferencing process. Without this engagement, communication with patients and families is compromised.
Our methods have both strengths and limitations. The richness of the videotape data enables examination of both verbal and nonverbal data. 63 Triangulating the data of the conference videos, the conference audios, and the interviews enabled us to develop a rigorous model reflecting key elements of the family conference. The model is strengthened by having all participant groups represented: patients, family members and health care providers from multiple disciplines. This richness is counterbalanced by an intensity of analysis that limited the number of interviews. Family conferences were studied in only two medical centers in one city, limiting geographic and cultural diversity. Studying more conferences across more settings would enable exploration of patterns relating to demographic diversity and interdisciplinary collaboration.
Further research on family conferences in the setting of palliative and end of life care needs to systematically explore demographic variations in who receives family conferences, and the frequency and timing of conferences along the trajectory of illness. Process evaluation is needed to further understand what drives conference success, especially relating to emotion work. Finally, research needs to explore the impact of family conferences on communication, continuity of care, and the quality of the patient/family experience of care.
Footnotes
Acknowledgments
This research was conducted under a grant from the UniHealth Foundation in Los Angeles, California. We appreciate the foundation's support and interest in this work. Thank you to the medical and palliative care teams at the participating medical centers for their crucial collaboration, to Marc Roseboro for his sensitive and skillful videotaping, and to Joya F. Golden for her thoughtful administrative assistance. Most of all, we thank the family conference participants—patients, family members, and staff—who graciously shared their experiences with us and made the research possible.
Work related to this research was presented at the conferences of the American Academy of Hospice and Palliative Medicine & Hospice and Palliative Nurses Association in February 2007, the American Psychosocial Oncology Society in March 2007, the European Association for Palliative Care in June 2007, and the International Psycho-Oncology Society in September 2007.
Author Disclosure Statement
No competing financial interests exist.