
Abstract
Abstract
Background:
After 20 years of debate regarding the appropriateness of family-witnessed resuscitations (FWR), little substantive data exist to suggest a benefit or harm to the family member.
Objective:
To compare bereavement-related depression and post-traumatic stress disorder (PTSD) symptoms among cardiopulmonary resuscitation (CPR) patients' family members who remain in the waiting room of an urban emergency department (ED) with those who are invited to witness CPR.
Methods:
A prospective comparison study was conducted at two large, urban, Midwestern teaching hospitals. Adult family members of nontraumatic CPR ≥18 years of age patients were eligible. In the intervention hospital, emergency physicians were trained and encouraged to invite family members to witness CPR (FWR). At the control hospital, family remained in the ED waiting room (Non-FWR). Family members from each hospital were interviewed 30 and 60 days post-event regarding bereavement-related depression and PTSD symptoms. Relevant demographic information was also collected. Comparisons between FWR and Non-FWR were conducted using independent samples t tests and χ2 where appropriate.
Results:
Sixty-five family members (24 FWR and 41 Non-FWR) were included. There were no differences between groups in relationship to the patient (35% spouse/significant other), mean age (overall, 56 years), or race (75% African American). Patients in each group did not differ in need for assistance in any activities of daily living (overall, 44% needed assistance) prior to cardiac arrest. However, more FWR were female (83% versus 59%), and had higher levels of overall social support available. There were no differences between FWR and Non-FWR on overall PTSD scores (11.7 versus 11.4; mean difference = 0.3 [95 confidence interval (CI): −5.5; 6.1]) or depression scores (16.0 versus 20.6; mean difference = −4.5 [95CI: −12.0; 3.0]).
Conclusion:
Bereavement related depression and PTSD symptoms are commonly seen in family members of cardiac arrest victims, however, the magnitude of the effect is not impacted by witnessing or not-witnessing CPR in the ED.
Introduction
Although there have been a number of publications that suggest that family members are amenable to this practice and would do it again in a similar situation,8–12 it remains a widely debated issue among ED personnel.13–17 Foremost among the concerns are the potential for increased litigation, and for family members to obstruct the resuscitation attempt. Additionally, there is an underlying concern regarding lay-person exposure to the process of CPR, which is an inherently traumatic event. These concerns are highlighted by reports that suggest that witnessing CPR in the pre-hospital setting is associated with significant increases in symptoms of post-traumatic stress disorder (PTSD), 18 and that the presence of an overtly grieving family member may delay the initiation of key resuscitation procedures. 19
Much of this uncertainty arises from a critical gap in knowledge regarding the potential consequences of family presence during the process of ED resuscitation. Evidence suggests that this may be particularly true in urban locales. 20 Therefore, the purpose of this study was to compare markers of adverse bereavement outcomes among family members who remain in the waiting room with those who are invited to witness active CPR in an urban ED setting.
Methods
Design and setting
This was a prospective, quasi-experimental, comparison group study conducted in two large, urban, Midwestern academic EDs. Each hospital is located in Detroit, MI, where out-of-hospital cardiac arrest is almost uniformly fatal, 21 and each is affiliated with the Department of Emergency Medicine at Wayne State University. Combined, these hospitals provide care for ≥180,000 patients each year, of which approximately 360 receive CPR for nontraumatic causes. The patient population is primarily African American, and most patients are un- or underinsured. This study was approved by the Wayne State University Institutional Review Board.
Subjects
Participants in this study were English-speaking, adult (≥18 years) family members or significant others of adult (≥18 years) patients who received CPR, which was defined as active chest compressions. Eligibility required presence in the ED while the medical (nontraumatic) resuscitation was in progress and permission from the attending physician in charge of the resuscitation.
Study protocol
This study took place between November 1, 2007 and October 31, 2009. All adult family members present in the ED waiting room of either study hospital during the course of a loved one's resuscitation attempt were identified by a trained research assistant. In the control arm, following conclusion of a failed resuscitation attempt, permission was sought from the family spokesperson (designated as such by family members or, if no one else was present, by the research assistant) to allow subsequent contact by study personnel. In the intervention arm, while CPR was being conducted, the family spokesperson was invited to witness the resuscitation attempt with an escort. Family members willing to provide follow-up information were contacted via telephone 30 and 60 days after the ED encounter. The first interview (30 days post-event) obtained demographic data, as well as information related to factors that may contribute to poor bereavement outcomes, such as whether or not the participant witnessed CPR in the pre-hospital setting.
Training of researchers
In-service training sessions regarding FWR were provided to all emergency medicine physicians (resident and faculty) at the intervention hospital by an attending physician with several years experience conducting FWR in EDs. In addition, a nurse practitioner was trained as a family member escort with specific instructions to:
•
•
•
•
•
Additionally, as part of a collaborative educational project, second- and third-year emergency medicine residents at each hospital concurrently participated in a simulated resuscitation attempt (using a high-fidelity human patient simulator), which included a standardized family witness (played by a trained actor). A complete description of this experience has been described elsewhere. 19
Outcome measures
We operationally defined evidence of adverse bereavement as symptoms of depression and PTSD. We used the following respective measures: the Center for Epidemiological Studies–Depression (CES-D) Scale, and the PTSD Symptom Scale-Self Report (PSS-SR). Both instruments are well-accepted measures with desirable reliability and validity characteristics. Important to the context of this setting, the CES-D has been validated in a nationally representative African American population, 22 and the PSS-SR has been used in African American cohorts, though no data regarding its psychometric properties have specifically been described in this population.23,24 Although we report the mean for each outcome measure as well as the percentage of participants falling within each diagnostic category for each scale, these data were not intended to enable diagnosis of psychological illness, and stand to serve merely as general makers of poor bereavement outcome.
Statistical methods and sample size
After review of the historical CPR rates and a pilot study to ascertain the prevalence of family member presence in the ED waiting room during active CPR at each hospital, we derived an intended sample size for this study based on feasibility of 60 patients, with 30 coming from each of the hospitals. We provide descriptive statistics of all measurements and perform independent samples t tests, or nonparametric analogs, to compare the mean depression scores and the mean PTSD scores between groups, and report results using mean differences and associated 95% CI. To aid in the interpretation of depression and PTSD symptom scores, we categorized respective participant outcomes using associated guidelines for diagnosis of each disorder. For the depression scale, the categories were “no/low,” “mild to moderate,” and “possible major depression.” For the PTSD scale, participants were categorized as to whether or not they had symptoms (yes/no) in each of the instrument's subscales: “re-experiencing,” “avoidance,” and “increased arousal.” If the participant experienced symptoms in each subscale, they were categorized as “possible PTSD.” We compared these categorical data using χ2, and to control for the fact that the study groups were substantively different on variables potentially related to the outcomes, we conducted multivariable hierarchical multiple regression models for each outcome (depression and PTSD symptoms).
Results
Overall, there were 65 participants in this study: 24 witnesses to a resuscitation, and 41 nonwitnesses. All eligible participants who were invited to be involved in the study, whether as a witness or nonwitness, agreed to participate. The imbalance in sample size was due to differential inclusion criteria: control participants were identified following the death of their family member, whereas intervention participants were identified during the resuscitation attempt. Thus, although resuscitations at the intervention hospital were common, early arrival of family members during the resuscitation attempt (or early enough to warrant an invitation to witness the event) was rare.
No participant in either group admitted to accessing any hospital-based bereavement support service, or requested information regarding such services. One participant at the intervention hospital wished not to respond to the bereavement outcomes portion of the interview due to emotional difficulty. Therefore, although this participant's scale information is not accessible, we have chosen to include this participant in all categorical measures of poor bereavement outcomes in the FWR group. As shown in Table 1, most of the participants were African American, female, a close relative of the patient, and had substantive levels of social support. Importantly, many of the participants (38.5%) witnessed CPR in the pre-hospital setting and, 8 (12.3%) individuals actually performed bystander CPR prior to ED arrival. Resuscitation outcomes were identical (all 65 CPR recipients expired prior to hospital discharge), and, as shown in Table 2, patients' need for assistance with activities of daily living prior to cardiac arrest was similar between groups.
The Caregiver Strain Index is computed by summing the number of stressors related to caring for the patient.
Measures of social support is the mean rating on a scale of 1 to 5, with 5 indicating the most social support.
Indicates a significant (p < 0.05) difference between groups.
One participant did not complete this portion of the interview.
ADL, activities of daily living.
Participants demonstrated an overall high level of depression and PTSD symptoms during bereavement (Tables 3 and 4), but these outcomes did not differ significantly between the FWR and Non-FWR groups at 30 or 60 days. The only evidence suggestive of a difference in poor bereavement outcomes was observed in the “increased arousal” subscale of the PSS-SR at 60 days (mean difference 2.63 [95% CI: 0.36; 4.90]).
Note: One FWR participant wished not to respond to the psychological questionnaires due to emotional difficulty, and is therefore categorized as experiencing all PTSD category symptoms as well as possible major depression; however, this is not represented in the mean ratings.
Note: One FWR participant wished not to respond to the psychological questionnaires due to emotional difficulty, and is therefore categorized as experiencing all PTSD category symptoms as well as possible major depression; however, this is not represented in the mean ratings.
As shown in Figure 1, we also assessed whether participants' symptom scores increased or decreased between the 30 and 60 day interviews, comparing the progression of bereavement outcomes for each group. The median reduction in CES-D scores was significantly greater for participants in the FWR group (median reduction: 7.0 versus 2.0, respectively; p = 0.013), but were similar for PSS-SR scores (median reductions: 5.0 versus 3.0, respectively; p = 0.200).
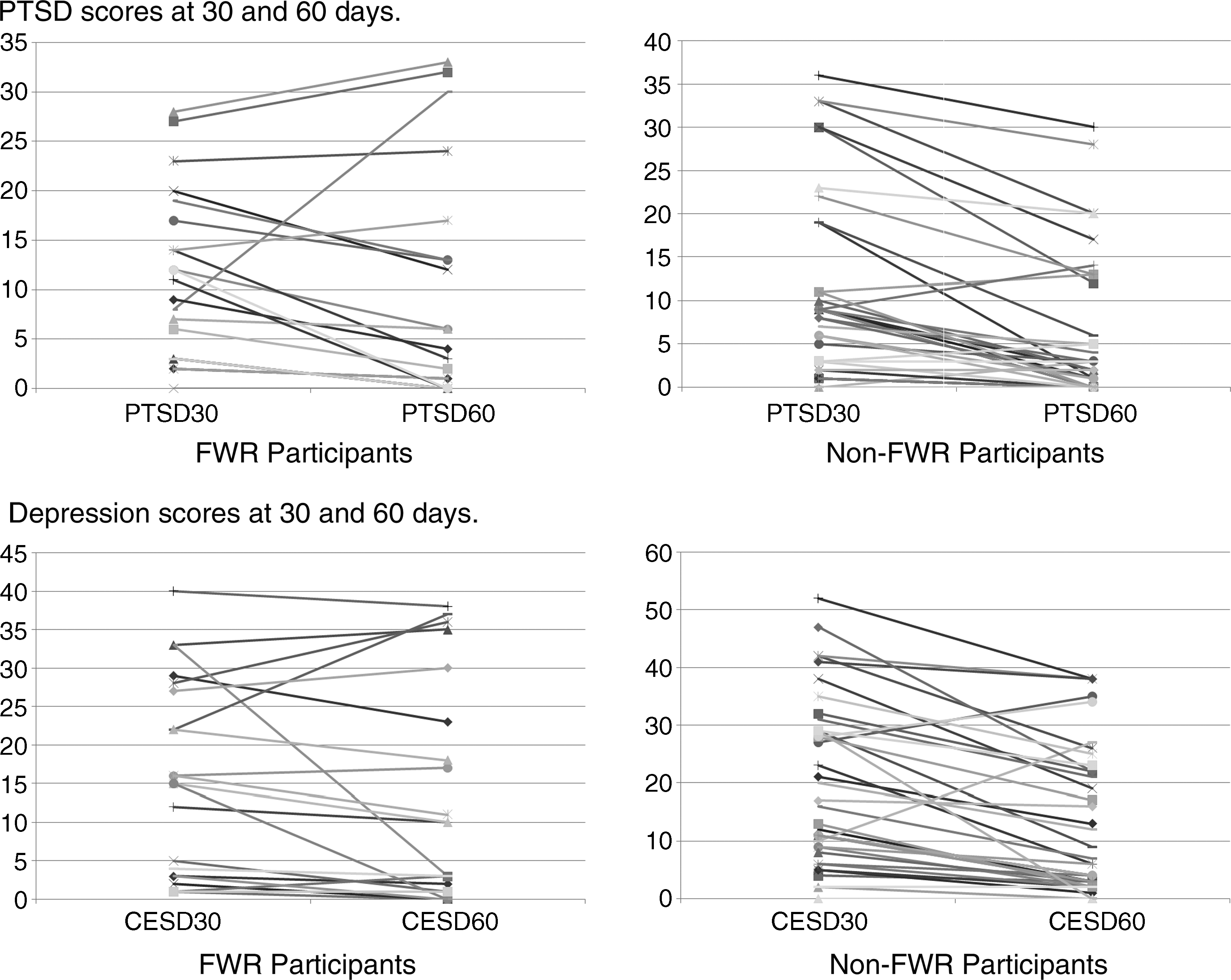
Participant symptom scores.
To assess the impact of witnessing CPR, regardless of location, we realigned groups post hoc into those who witnessed CPR either pre-hospital or in the ED (n = 36) and those who did not (n = 29). Results for 30-day CES-D scores were similar whether or not participants witnessed any CPR event: 19.4 (±14.1) for witnesses versus 18.7 (±14.5) for nonwitnesses (mean difference = 0.69 [95 CI: = 6.8 to 8.2]), and there was no difference between CPR witnesses and nonwitnesses in terms of CES-D score change between 30 and 60 days (5.0 [ ± 10.0] versus 5.9 [ ± 7.0]; mean difference = 0.9 [95% CI: −5.7 to 3.9]). PTSD scores trended toward an increase in the witness versus nonwitness groups (13.7 [ ± 11.3] versus 9.2 [ ± 10.3]) but the mean difference (4.5 [95% CI: −10.1 to 10.1]) was not statistically significant. There was also no difference between CPR witnesses and nonwitnesses in terms of the change between 30 and 60 day PTSD scores: 3.8 (±7.3) versus 4.3 (±5.4); mean difference = −0.5 (95% CI: −4.1 to 3.0).
In the hierarchal multivariable regression models, we included the participant's gender and score on the social support scale, as well as the patient's need for assistance on any activity of daily living (yes|no). Controlling for these variables did not alter the interpretation of the effect, or lack thereof, of being a witness to the resuscitation.
Discussion
In this report, we provide results for the largest and most comprehensive study of the impact of FWR on witnesses' bereavement outcomes to date, and present, for the first time, data derived from an urban, predominantly African American population. Overall, we have no evidence to suggest that bereavement outcomes at 30 and 60 days are substantively different in family members who witness resuscitations in the ED versus those who remain in the waiting room. However, our results provide provocative implications regarding the persistence of adverse bereavement over the course of 60 days with demonstration of lasting depression symptoms among family members who witnessed the resuscitation attempt. What exactly this means in the context of end-of-life care in the ED, however, is unclear. Interestingly, our findings were noted despite the fact that nearly 45% of our participants were with the patient at the time of his or her collapse and most witnessed CPR in the pre-hospital setting prior to ED arrival. While serving as a potential confounder for our results, this calls into question the common practice of “sheltering” family members during the resuscitation of loved ones.
Our follow-up period of 30 to 60 days was chosen for three reasons. First, this time period is the earliest point at which capture of symptoms associated with PTSD can be achieved. Second, because grief is a dynamic process that fluctuates considerably over time (rather than a static trait), symptoms that are still present after 30 days of bereavement are likely to be clinically significant. Third, not all patients will manifest consequences in the early post-event period and inclusion of follow-up past 30 days was needed to detect late development of symptoms.
Initial positive reports associated with FWR prompted researchers in the United Kingdom to conduct a randomized trial comparing outcomes of family members who witnessed the resuscitation of a loved one with those who did not. 25 In this study, pediatric and adult patients requiring CPR for medical or traumatic reasons were randomized to either a control arm (no family witness) or a group designated for chaperoned FWR. Although the study design intended to interview 64 family members after 1 and 6 months, the study was terminated after 25 patients were enrolled (13 randomized to the intervention arm) because the investigators feared that the clinical team was so convinced of the benefit of FWR that it would be no longer willing to randomize family members to the control arm. Objectively, however (and consistent with our results), these investigators found no evidence to suggest that the practice was harmful or helpful. These results, coupled with ours, lead us to conclude that if there is an interest in having family members witness CPR at an institution where sufficient resources exist (i.e., a dedicated chaperone), and the process has been prepared for and planned well, FWR can be performed.
There are several limitations to our study. First, the extent of the exposure of FWR is variable and may differ in both time and intensity, making the generalizability of this intervention tenuous. Secondly, and most importantly, this was not a randomized study, thus there are important differences between our witness and nonwitness groups that undoubtedly interact with our outcome variables. Although our sample size does not permit for an extensive multivariable analysis, we conducted several exploratory analyses to identify alternative interpretations of the effect of FWR. Regardless of our approach (i.e., comparing those who witnessed CPR anywhere, or performed CPR) we found similar, no-effect results.
The principal cause of the selection bias is based in who the physicians and study staff asked to participate, particularly in the witness group. However, this same selection process would be likely in actual practice. As demonstrated by the unequal recruitment of intervention and control cases, our experience identified that many times the family member did not arrive to the ED in time to be invited to witness the resuscitation attempt. This may be a significant issue because family members accompanying the patient in transport, and thus eligible to be present in the ED during a short resuscitation attempt, may be more likely to be the patient's primary caregiver or loved one. This could result in an imbalance in emotional closeness (rather than relationship) between witnesses and nonwitnesses. However, this study design was chosen with full recognition of these limitations, and was determined to be more appropriate than a randomized trial in this particular setting. During our preliminary work preparing for this project, we conducted a survey of the ED personnel at each of these hospitals and identified that there was strong support and strong opposition to the practice of FWR, 20 which raised our concerns regarding conducting a randomized study. In this environment, there was perceived to be too strong of a risk that participants would not receive the treatment that they were randomly assigned to, thus creating an imbalance that would be insufficiently handled by the intention-to-treat principle. Ideally, a larger sample size would be useful to statistically control for important confounding variables; however, for the scope of this project, inclusion of a more expansive participant pool was not feasible. Given the preliminary evidence and limitations of this study, future multisite trials are needed to more adequately address comparable treatment groups, of large size, in order to adequately control for factors that may be related to the outcome, such as gender and social support available to family member witnesses, as well as patient-level characteristics such as quality of life and medical condition prior to the arrest.
Conclusion
The results of this study conducted in a large urban area with a predominantly African American population suggest that bereavement-related depression and PTSD symptoms are common sequelae in family members of deceased, adult, nontraumatic cardiac arrest victims. However, the magnitude of the effect is not substantively impacted by witnessing or not witnessing CPR in the ED.
Footnotes
Acknowledgments
This project was supported by a grant from the Blue Cross Blue Shield of Michigan Foundation.
Author Disclosure Statement
No competing financial interests exist.