
Abstract
Abstract
Purpose:
To examine the reported rates and predictive factors for sleep disturbance in patients with bone metastases.
Methods:
Patients with symptomatic bone metastases treated with palliative radiotherapy (RT) were eligible. At initial consultation, demographic information, baseline Brief Pain Inventory (BPI) questionnaire, and analgesic consumption were recorded. The BPI functional interference sleep item was categorized into none (0), mild (1–3), moderate (4–6), and severe (7–10). Follow-up BPI was collected in person or via telephone post-RT at week 4, 8, and 12. Subgroup analysis for BPI between responders and nonresponders was performed. Ordinal logistic regression analysis was used to search for the relationship between sleep disturbance and other covariates.
Results:
Four hundred patients were enrolled between May 2003 and June 2007. Two hundred thirty-five males (59%) were accrued. The median age was 68 years old (range, 30–91). Within the study population, primary cancer sites included breast (25%), lung (25%), prostate (24%), bladder (4%), pancreas/gastric (3%), and other primaries (18%). In the BPI functional interference items, the mean baseline score for sleep disturbance was 4.8. When categorized in terms of severity, 99 (25%) patients had moderate sleep disturbance and 144 (36%) patients had severe sleep disturbance, respectively. There was an improvement in sleep scores for both responders and nonresponders at week 4 and 8, but scores worsened for nonresponders at week 12.
Conclusion:
Age, Karnofsky Performance Scale (KPS), pain score, and lung primary were the significant variables associated with sleep disturbance. The scores for sleep disturbance improved significantly post-RT in responders at week 4 and 12.
Introduction
Sleep disturbance is associated with a number of negative consequences that, when combined, affect the health-related quality of life (QOL) in an individual. 6 A disruption in the regular sleep schedule can interfere with the restorative function of sleep, thereby drastically decreasing the QOL. 7 There has been evidence to suggest that poor sleep can profoundly affect cognitive, psychological, and physical function. 8 A report by Mystakidou et al. 9 showed that sleep disturbance can be a significant risk factor for depression and anxiety in patients with cancer. This study goes on to reveal that sleep disturbance can even be correlated with an increased desire for hastened death.
Despite the high prevalence and significant risk factors associated with sleep disturbance, health care professionals tend to underdiagnose and undertreat the problem. 4 One of the main goals of palliative care is to maintain or improve the QOL of patients; as such, it is necessary to assess and address sleep problems within this patient population. There is also value in being able to predict sleep difficulties within patient populations, so as to be better prepared to manage their care. The purpose of this study was to examine the self-reported rates and predictive factors for sleep disturbance in patients with bone metastases attending an outpatient radiotherapy clinic, using the Brief Pain Inventory (BPI) and baseline demographic information, respectively. Subgroup analysis was also performed to gauge differences in severity of sleep disturbance between partial/complete responders to treatment compared to nonresponders.
Methods
The Rapid Response Radiotherapy Program (RRRP) at the Sunnybrook Odette Cancer Center is an outpatient clinic that provides timely access to palliative radiation for patients with advanced cancer. Most patients are simulated and treated on the day of their initial consultation to help provide quick symptom relief and hopefully improve their quality of life. A retrospective analysis of patients with cancer referred to the RRRP for palliative radiotherapy for symptomatic bone metastases between May 2003 and June 2007 was conducted. Eligible patients included those treated with radiotherapy for their symptomatic bone metastases, and were at least 18 years of age. Ethics approval to conduct the research was obtained from the Sunnybrook Health Sciences Centre Ethics Review Board. At initial consultation, demographic information, including age and primary cancer site, was recorded along with analgesic consumption. Patient performance status was evaluated using the Karnofsky Performance Scale (KPS). Additionally, patients were asked to complete a baseline short-form BPI questionnaire.
The BPI is a self-assessment tool that has been validated internationally in patients with cancer.10–13 The short-form survey contains 10 scaled questions, 3 of which assess pain intensity and 7 measure functional interference. The scales are anchored between a value of 0 (no pain/interference) to 10 (maximum pain/interference). Among the functional interference items is one that evaluates the impact of pain on sleep.
The BPI functional interference sleep item cutpoints were extrapolated from those validated for the Edmonton Symptom Assessment Scale 14 ; sleep interference was categorized into none (0), mild (1–3), moderate (4–6) and severe (7–10). Follow-up BPIs were completed either in person or via telephone by a research assistant at 4, 8, and 12 weeks post-RT. Additional subgroup analysis for BPI between nonresponders and responders was performed to serve as a method of assessing variations in sleep disturbance severity. Nonresponders were patients in whom there was progressive disease (PD) or stable disease (SD). Responders were patients who showed either a complete (CR) or partial response (PR) to radiation treatment (Table 1). 15
Note: OMED = oral morphine equivalent dose in the last 24 hours.
Descriptive statistics and frequency distributions were generated for the patients' demographic and disease-related characteristics. Ordinal logistic regression analysis was used to search for the relationship between sleep disturbance and other covariates (i.e., age, KPS, gender, primary cancer site, pain site, pain scores). Odds ratios (OR) and 95% confidence intervals (CI) were calculated in the cumulative logit model for each covariate. The probabilities modeled were cumulated over the following BPI order: 3 = severe; 2 = moderate; 1 = mild; and 0 = none. One-way analysis of variance (ANOVA) was applied to compare the BPI sleep item in responders and nonresponders at the follow-up week 4, 8, and 12. A two-sided p value of <0.05 was considered statistically significant. All calculations were conducted by Statistical Analysis Software (SAS version 9.2 for Windows, SAS, Cary, NC).
Results
A total of 400 patients completed the BPI questionnaire between May 2003 and June 2007. The patient population comprised 235 males (59%), and the median age was 68 years old (range, 30–91). The most common primary sites of cancer were breast (25%), lung (25%), and prostate (24%). Less common primaries were bladder (4%), pancreas/gastric (3%), and other cancer sites (18%). A total of 243 patients received single-dose radiation treatment (800 cGy/1 fraction; 61%) as opposed to multiple dose regimen (typically consisting of 2000 cGy/5 fractions or 3000 cGy/10 fractions). Table 2 summarizes patient demographics of the study population, while Table 3 shows the distribution of some of the baseline variables across the severity increments of sleep disturbance.
SD, standard deviation; KPS, Karnofsky Performance Scale.
Five patients did not complete the BPI functional interference sleep item.
Fifteen patients were not assigned KPS scores.
SD, standard deviation; KPS, Karnofsky Performance Scale, BPI, Brief Pain Inventory.
With regards to the BPI functional interference item, the mean baseline score for sleep disturbance was 4.8 and the median score was 5. Roughly one-fifth (22%) of patients had no sleeping problem, while 17% of patients had mild sleep interference. The majority of patients at baseline had either moderate or severe sleep disturbances; with 25% and 37% of patients registering those sleep scores, respectively (Table 4). Five patients did not complete the BPI functional interference sleep item.
The ordinal logistic regression analysis created a prediction model for sleep disturbances, and the following factors were shown to be statistically significant predictors (Table 5): age (OR = 0.98; 95% CI = 0.96–0.99; p = 0.0001), KPS (OR = 0.98; 95% CI = 0.96–0.99; p = 0.0015), worst pain score (OR = 1.34; 95% CI = 1.24–1.46; p < 0.0001), and lung as the primary cancer site (OR = 1.76; 95% CI = 1.16–2.69; p = 0.0085). Younger patients were more likely to be afflicted with severe sleep disturbances; those who reported severe sleep problems were, on average, 62 years old in contrast with those with moderate (67 years), mild (68 years), and no (68 years) sleep problems.
Where p < 0.05 is considered statistically significant.
KPS, Karnofsky Performance Scale.
Additionally, severe sleep disturbances were more frequently reported in patients with a poorer KPS score (average KPS score was 67 for those with severe sleep disturbances, 71 for those with moderate, 73 for those with mild, and 72 for those with none). A higher worst pain score (representing more severe pain) as measured with the BPI also correlated with more profound sleep disturbances (Fig. 1). Finally, in patients with primary lung cancer, there were 31% with severe, 27% with moderate, 21% with mild sleep disturbances, and only 15% who reported no sleep difficulties.
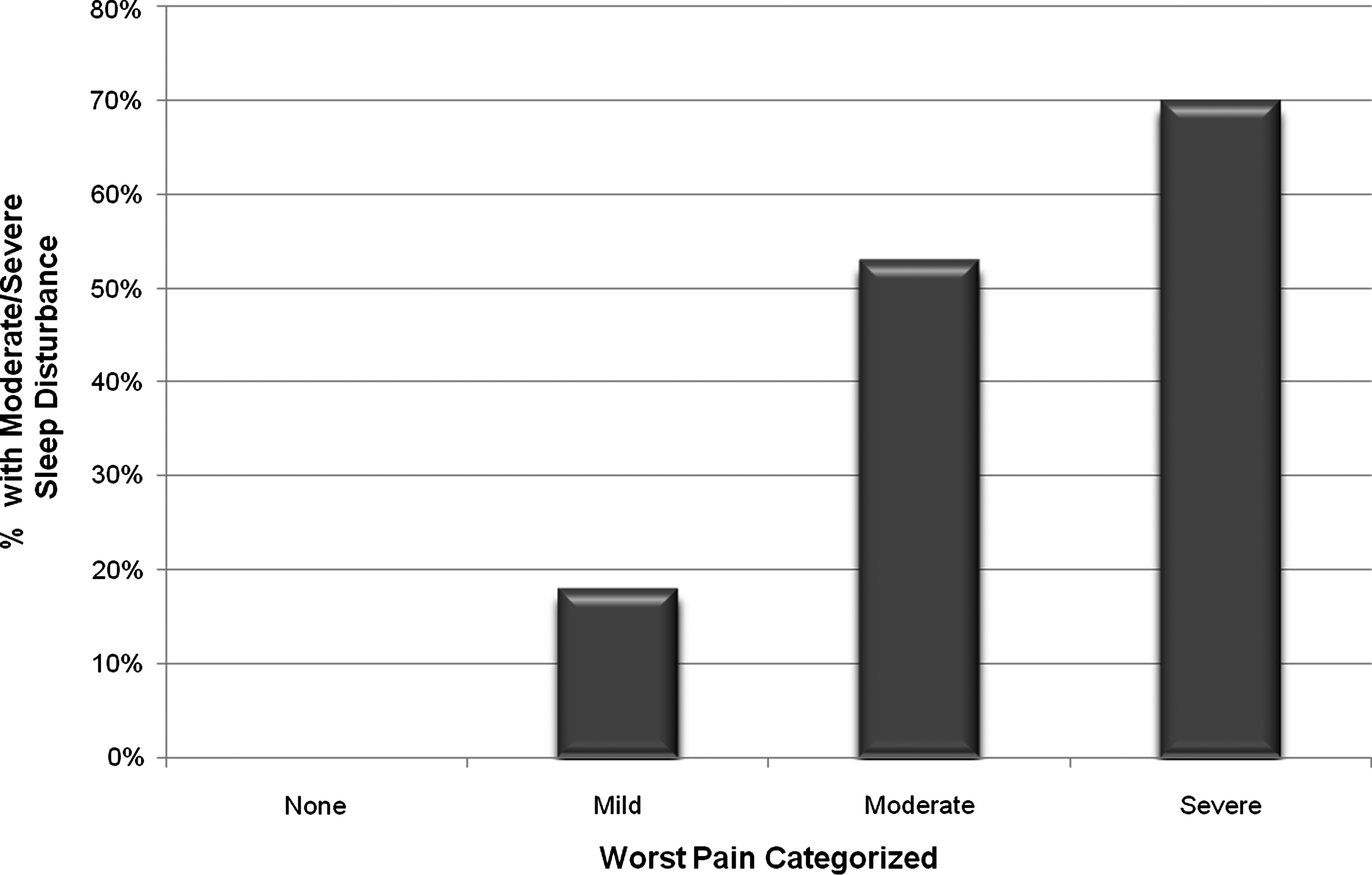
Correlation of sleep with pain at baseline. p value <0.0001.
The BPI sleep item was also compared at follow-up in weeks 4, 8, and 12 between nonresponders and responders to radiotherapy treatment (Table 6). Among the 400 patients at baseline there were 275 patients with week 4 follow-up, 217 patients with week 8 follow-up and 188 patients with week 12 follow-up. The overall response rate by monthly follow-up was as follows: at week 4, 58%; at week 8, 59%; and at week 12, 66%, respectively. Follow-up mean sleep item scores for nonresponders were 3.44, 2.29, and 2.77 at weeks 4, 8, and 12 respectively; mean sleep item scores for responders were 1.98, 1.63, and 1.40. The results were statistically significant for weeks 4 and 12 (Fig. 2; p = 0.0004 and 0.003, respectively). It was evident that there was an improvement in sleep scores for both responders and nonresponders at week 4 and 8, but scores worsened for nonresponders at week 12.
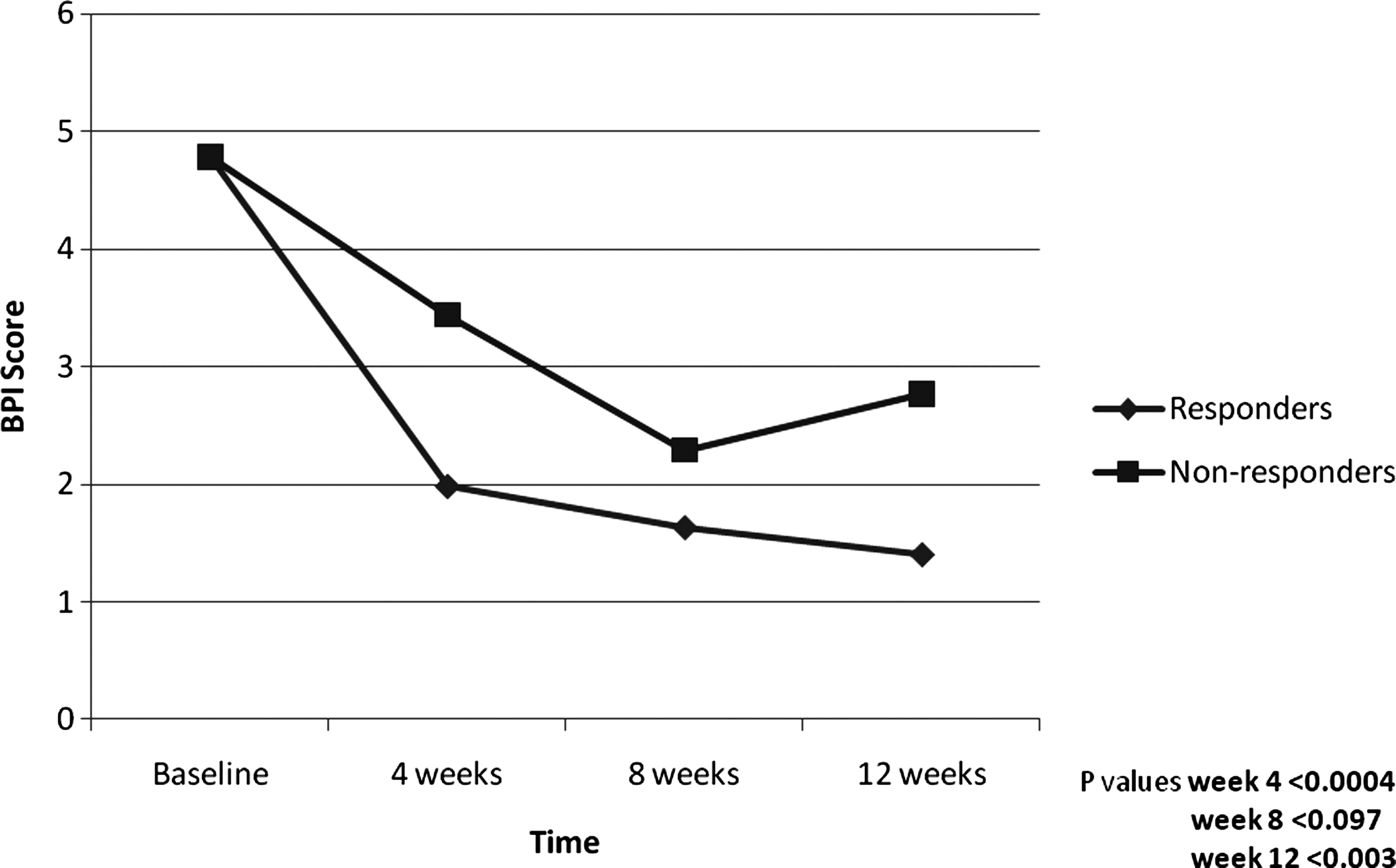
Difference in Brief Pain Inventory (BPI) severity between responders and nonresponders for sleep posttreatment.
CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; CI, confidence interval.
Discussion
The results from our study showed a statistically significant improvement in sleep at weeks 4 and 12 in the responder population. One would expect to see this result, as the improvement of pain should improve quality of life and therefore have the potential to impact on sleep. One would also expect this result to be seen at 8 weeks of follow-up, however, although an improvement was seen, it was not statistically significant. The results also indicated improvement in sleep for the nonresponders, although not statistically significant. These results could be due to a variety of reasons such as changes in pain medication or concurrent therapies; however, due to the retrospective nature of this study, this information was not captured.
At initial consultation, approximately 78% of the patient population reported at least a mild sleep disturbance. Our analysis showed that more severe sleep disturbances were more likely to occur if the patient was younger, or rated a lower KPS score. Patients who had primary lung cancer were also more likely to suffer from severe sleep disturbances. Furthermore, higher pain scores correlated with more serious sleep disturbances. Other factors such as gender and site of pain were not observed to be significant predictors of sleep disturbances.
The proportion of patients with sleep disturbances within our study population was somewhat higher than what has been reported in other accounts in the literature. A review article by Kvale and Shuster 16 reports the prevalence of insomnia among patients with cancer to be between 19%–63%. In another review by Sateia et al., 1 prevalence of sleep disturbance in patients with advanced cancer is identified as between 10%–74%. This discrepancy is likely due to the varying end points used to define sleep problems in the literature. For example, in one study, 30% of the study population had sleep difficulties whereby they received less than 5 hours of sleep. 17 Yet patients receiving 8 or more hours of sleep have been shown to still experience poor and fragmented sleep. 5 Therefore, the definition and assessment of sleep disturbances can vary widely and cause its prevalence to fluctuate between studies. Perhaps a better tool can be created in order to standardize the assessment of good quality sleep, due to the subjective nature of this construct.
Within this study, the patients' age was seen to affect the prevalence and quality of sleep disturbances, while their gender was not significantly correlated. Patients who were younger reported more severe sleep disturbances when compared with those who were older. There has been some disagreement within the literature as to whether younger age is associated with poorer sleep,3,18 or if there is no correlation between the two.7,17 Furthermore, within the general population, older age is actually a predictor for more frequent sleep disturbances. 19 However, younger age can be associated with more severe symptom burden, 3 which can contribute to the frequency and severity of sleep disturbances. 1 This current study revealed no correlation between patient gender and their susceptibility to sleep disturbances, which is comparable to other studies.3,7 However, in the general population females tend to be at a greater risk for developing insomnia. 19 Conversely, a study by Mercadente et al. 17 found that among patients with advanced cancer, males were more likely to have difficulty sleeping. It would be wise to pursue further research on gender and the prevalence of sleep disturbances in cancer populations to account for this discrepancy.
Mercadente et al. 17 also discovered that patients with lower KPS scores were more likely to be drowsy during the day, which is in accordance with the observation from this study where patients with lower scores tended to suffer from more severe sleep deficits. However, the distinction between correlation and causation should be noted, as it has been demonstrated that poor sleep may adversely affect performance status in patients. 20
Lung as a primary cancer site was found to be a significant predictor of sleep disturbances. Palesh et al. 3 also found that in their study population patients with lung cancer reported the highest prevalence of insomnia symptoms. This trend was also noted in a report by Davidson et al., 21 who found that patients with lung cancer enrolled in their study had high levels of all sleep-related problems. They attributed this to the shorter timeline upon which patients with lung cancer had received their diagnosis, as well as the higher likelihood for patients with lung cancer to possess comorbidities such as chronic obstructive pulmonary disease. Also, as noted in a review by Hajjar, 4 respiratory distress can contribute to the sleep disorders experienced by patients.
In this analysis, more acute pain was correlated with a greater tendency for severe sleep disturbances. This is in agreement with other studies,4,7,21–23 which have also demonstrated that pain can influence the quality of sleep. Managing patient symptoms and prescribing medication for the pain can help deal with the sleep disturbance.4,23
Other studies have shown additional factors to be correlated to higher reported rates of sleep disturbance. Psychological distress, in the form of depression and hopelessness, has been correlated with more significant sleep deficits, as has the use of stronger opiods.22,24 As previously mentioned, symptom burden can also be correlated with sleep disturbances, as symptoms of advanced disease such as respiratory and gastrointestinal dysfunctions and genitourinary symptoms can contribute to sleep disturbances. 25
Despite the frequency of sleep disturbances within the cancer population, the problem tends to be underreported 4 and one study noted that only about 16% of the patient population made physicians aware of their sleep difficulties. 26 Ultimately, it is important for clinicians to be trained in screening for sleep difficulties, given the profound effect that they may have on a patient's quality of life. 6 This study works to confirm this belief, identifying important factors that may contribute to the likelihood that a patient will suffer from sleep disturbance; however, it is equally important to recognize other factors from literature that have been shown to increase the likelihood of pathologic sleep, including psychological distress and considerable symptom burden.
This study was limited in its retrospective nature. Another limitation exists due to the lack of documentation regarding concurrent therapies such as dexamethasone at initial consultation. In addition, the BPI is not a tool that is used specifically for assessing sleep dysfunction; it is often used as a screening tool. Future studies that are prospective in nature using QOL tools such as the EORTC QLQ-C30 would be beneficial in furthering knowledge regarding sleep impairment and quality of life.
Footnotes
Acknowledgments
We thank the Michael and Karyn Goldstein Cancer Research Fund and Stacy Yuen.
Author Disclosure Statement
No competing financial interests exist.