
Abstract
Abstract
Background:
Preserving dignity can be considered as a goal of palliative care. To provide dignity-conserving care, it is relevant to identify the factors that influence a patient's self-perceived dignity. This study aims to develop an instrument to measure factors affecting self-perceived dignity that has good content validity and is appropriate for use in practice.
Methods:
Data were collected in the Advance Directives Cohort Study. In 2008, the cohort received a questionnaire with 31 items that might influence one's self-perceived dignity. For a subsample of people with poor health (n = 292), we analyzed which items could be removed because of the mean scores for presence of the item and its influence on dignity.
Results:
The 31 items fell into four domains: evaluation of self in relation to others, functional status, mental state, and care and situational aspects. Mean scores for presence and influence on dignity showed large differences and were not correlated. Six items were scarcely present and did not substantially affect self-perceived dignity. Because three of these were expected to influence dignity in other settings, only three items could be removed and two items could be combined into one. After calculating correlations between conceptually similar items, one extra item could be removed.
Conclusion:
Reducing the instrument to 26 items and dichotomizing the answer option for presence increases its feasibility for use in practice. The instrument offers an important step to better understanding the phenomenon of self-perceived dignity by gaining information directly from patients.
Introduction
Despite the widespread use of the term “dignity,” there are only a few studies in which factors that support or undermine self-perceived dignity were the central focus. Recently, Periyakoil et al. created a Dignity Card-Sort Tool to assess which factors influence erosion or preservation of dignity at life's end (17;18). In a qualitative study, Chochinov et al. examined how patients with advanced terminal cancer understand and define the term. This resulted in the development of an empirical model of dignity in the terminally ill (19). Based on this model, the Patient Dignity Inventory (PDI) was developed—a measurement instrument consisting of 25 symptoms or experiences that could be used by clinicians to detect end-of-life dignity-related distress (20;21). The validity of this list was established in a study where patients in a palliative care program (predominantly cancer patients) were asked to what extent the item had been a problem or concern within the previous few days.
To examine the concept of dignity, and the relevance and comprehensiveness of the PDI in a different population, a cohort of Dutch people with one or more advance directives (ADs) received a questionnaire in spring 2007 (22;23). One-half of the cohort received a questionnaire with items from the prototype PDI (with 22 items). The other half received open-ended questions, asking respondents how they would define dignity and what issues they thought would influence their sense of dignity during the last phase of life. The answers given to the open-ended questions were largely corresponding to the prototype PDI items, indicating that the prototype PDI has fairly good content validity. However, it became apparent that items related to care and ability to communicate were lacking in the prototype PDI. Furthermore, some items were too abstract for respondents to understand. For example, the prototype PDI items “Not being able to independently manage bodily functions” and “Not being able to carry out tasks of daily living” were not always thought to include “going to the toilet without help” or “being able to wash yourself” (22). These findings prompted us to develop a new measurement instrument, which is based on the construct of dignity found in the answers on the open-ended questions. An additional reason for developing a new instrument was the recognition that the weight given to factors influencing self-perceived dignity differs between individuals and cannot directly be derived from the knowledge whether or not an aspect is present. Therefore, the new instrument distinguishes between (a) to what extent an item is present and, if so, (b) to what extent this influences one's sense of dignity.
For practical use in end-of-life care, the instrument not only has to be comprehensive, but must also take as little effort as possible for the patient to fill it in.
Consequently, the purpose of the present study is to develop an instrument to measure factors that affect self-perceived dignity, with good content validity and feasible for use in practice. In this study, we focus on possibilities for reducing the number of items listed and on the assumed distinction between the concepts of presence and influence on dignity, with regard to self-perceived dignity.
Methods
Design and study population
Data for this study were collected in the Advance Directives Cohort Study, a major ongoing longitudinal study on end-of-life issues (23). Since October 2005, a cohort of people with one or more of the four most frequently used ADs in the Netherlands receive a written questionnaire every 18 months.
Three of these most frequently used ADs are formulated by the “Right to die-NL” (NVVE in Dutch): the advance euthanasia directive, refusal of treatment document, and appointment of a health care representative. The fourth (standard) AD is the “wish to live statement” (in which the patient states that s/he wants adequate care directed at quality of life and is explicitly against euthanasia), provided by the Dutch Patient Association (NPV in Dutch). This association is based on Christian values. The cohort is a sample of randomly selected members of both associations.
The present study is based on data collected in autumn 2008. In this third cycle of data collection, a total of 4,399 members of the NVVE and 1,050 members of the NPV completed the questionnaire. Because dignity is considered as a goal in end-of-life care that may be threatened by severe illness, we selected a sample of 292 people to evaluate the instrument: 235 members of the NVVE and 57 members of the NPV. These people were all those within the larger sample of 5,449 participants who stated that they had an illness and also indicated being severely impaired in at least one dimension of the EQ-5D (mobility, self-care, usual activities, pain/discomfort, or anxiety/depression) and had filled in the dignity questionnaire.
The measurement instrument
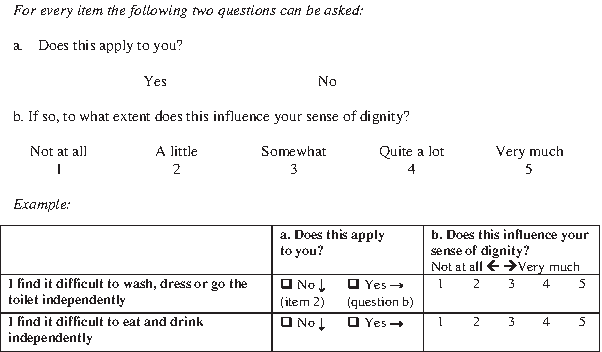
A random half of the cohort received open-ended questions about personal dignity in the second cycle of data collection (spring 2007). Their answers have been analyzed, resulting in the development of content labels. Based on these content labels, we formulated items to cover the content (22). To this end, we used or adapted formulations that arose in the answers to the open qualitative questions, but also included new ones by combining answers, to create items that were more broadly applicable and understandable. For instance, the content labels “not receiving enough care from people around me,” “not receiving enough attention and understanding,” and “affectionate, warm, loving care” were combined in the item “I receive too little attention and care from the people around me.” This process resulted in an instrument that consisted of 31 symptoms or experiences that might exert influence on dignity. Respondents were asked to indicate (a) to what extent the item was present and, if so, (b) to what extent their sense of dignity was influenced by the item (Fig. 1). Both questions were measured by using a uniform five-point scale. The second question was not asked if the item was not present. In addition, we asked respondents to rate their sense of dignity on a 10-point scale (1 = sense of dignity completely lost, 10 = sense of dignity completely intact).

Questions about personal dignity.
Theoretical framework
The 31 items can be considered as causal indicators, because the occurrence of these symptoms or experiences can cause a change in self-perceived dignity. Even a single symptom or experience may suffice to cause impairment of self-perceived dignity, although a low sense of dignity need not necessarily imply that someone suffers from all the symptoms listed (24;25). Because of this, it is not meaningful to calculate a sum or total score of all the items. Instead, each item must be considered separately. Because dignity is formed by the items, and not the other way around (i.e., the items are reflections of dignity), traditional methods for reducing the number of items, such as factor analysis and Cronbach's alpha, cannot be used. These traditional methods can only be applied when items are expected to correlate with each other (24–26). Instead, in models with causal indicators, valid grounds for omitting an item might be that (a) it occurs too infrequently to be worth reporting, or (b) it is very highly correlated with another item on the same questionnaire, so there is redundancy of information (25).
Analysis
First, we classified the 31 items in different domains, and ranked the mean scores for presence and influence on dignity per item. We analyzed the answers given by members of the NVVE and the NPV separately, because there are marked differences in opinions about end-of-life issues between these associations (23).
Secondly, to examine the extent to which the conceptual difference between (a) the presence of aspects and (b) their influence on personal dignity exists in actual practice, we assessed whether high-presence items were also highly influential on personal dignity. In addition, we calculated the correlation between the extent of being (a) present and (b) influential to dignity for each item, using the Pearson's correlation coefficient. We also calculated the overall correlation between the percentages of the items being present and their mean scores for influence on dignity.
Thirdly, we examined whether items could be removed from the list. We decided that an item might be omitted when it fulfilled both of the following criteria: (a) its mean score for presence was lower than 2.0 and (b) its mean score for influence on dignity was lower than the mean score of the item ranked 16th. This must apply for the answers from members of both associations.
To assess redundancy of information, we assessed whether items that seemed conceptually similar correlated highly on influence on dignity, using Pearson's correlation coefficients. An item was omitted if it correlated more than 0.7 with another item in both associations.
Results
Sample characteristics
Table 1 shows the characteristics of 292 respondents who suffered from a disease and were severely impaired on at least one of the dimensions of the EQ-5D. The majority of respondents in both groups were female and lived at home. The most frequently reported disease was rheumatoid arthritis, followed by heart disease. Furthermore, members of the NVVE rated their self-perceived dignity on average as 7.1 (on a scale from 1 to 10), while the mean score for members of the NPV was 7.6.
Poor health: having cancer and/or other illness and severely impaired in mobility, self-care, usual activities, pain/discomfort or anxiety/depression.
For 7 respondents from the NVVE and for 4 respondents of the NPV the residence is unknown due to missing observations.
For 9 respondents from the NVVE it is unknown, due to missing observations, whether or not someone's beliefs or religion is appreciated as important in one's life.
Many respondents had several diseases. The most prevalent diseases are listed in the table, but many others were mentioned (e.g. osteoporosis, spinal cord lesis, Chron's disease, migraine, Lyme disease, Chronic Fatigue Syndrome and PTSS).
For 8 respondents from the NVVE and for 9 respondents of the NPV the overall score for self-perceived dignity is unknown due to missing observations.
Significant difference between groups (p < 0.05).
Presence and influence on dignity
In Tables 2 and 3, the items are ranked according to the mean scores given for influence on dignity. We distinguished a framework of four domains: (I) evaluation of self in relation to others (8 aspects), (II) functional status (10 aspects), (III) mental state (5 aspects), and (IV) care and situational aspects (8 aspects). Table 2 shows that the mean scores for the presence of factors ranged from 3.5 (“not able to do domestic tasks”) to 1.3 (“struggle with beliefs or religion”) for members of the NVVE and were highest in the domain “functional status.” Similarly, for members of the NPV, the highest mean scores for presence were found in the domain “functional status” and ranged from 3.6 (“not able to do domestic tasks”) to 1.2 (“too little privacy”) (Table 3). In both groups, mean scores for presence were lowest in the domain “care and situational aspects,” In contrast, the highest mean scores for influence on dignity were found in the domain “evaluation of self in relation to others,” while the lowest mean scores for this concept were given for items in the domain “functional status.” These mean scores ranged from 3.5 (“not made a meaning or lasting contribution”) to 2.2 (“impaired hearing”) for members of the NVVE (Table 2) and from 2.9 (“lost control over my life”) to 1.5 (“impaired hearing”) for members of the NPV (Table 3). For all but one item, members of the NVVE reported items to be more influential to dignity compared to members of the NPV.
Poor health: having cancer and/or other illness and severely impaired in mobility, self-care, usual activities, pain/discomfort or anxiety/depression.
Presence: between 10 and 21 missing observations per item.
Influence on dignity: between 0 and 15 missing observations per item.
The overall correlation coefficient between the percentage to which items are present and the mean scores for influence on dignity is −.08.
For this item (a) the mean score for presence is lower than 2.0 and (b) the mean score for influence on dignity is lower than the mean score of the item ranked 16th.
Poor health: having cancer and/or other illness and severely impaired in mobility, self-care, usual activities, pain/discomfort or anxiety/depression.
Presence: between 0 and 8 missing observations per item.
Influence on dignity: between 0 and 5 missing observations per item.
The overall correlation coefficient between the percentage to which items are present and the mean scores for influence on dignity is .04.
For this item (a) the mean score for presence is lower than 2.0 and (b) the mean score for influence on dignity is lower than the mean score of the item ranked 16th.
There were no items for which the correlation between the extent of being (a) present and (b) influential to dignity was more than 0.7 in both the NVVE and NPV samples. Moreover, there was no overall correlation between the percentages of items being present and the mean scores for being influential to dignity (r = -.08 for members of the NVVE and r = .04 for members of the NPV).
Item reduction
Ten items in the group of the NVVE (Table 2) and 11 items in the group of the NPV (Table 3) occurred infrequently and barely exerted influence on dignity. These items met the formulated criteria to remove an item from the list. Of these, only six items met the criteria in both the NVVE and NPV sample. These items were: “not able to speak clearly or understandably,” “impaired hearing,” “feeling anxious,” “too little privacy,” “struggle with beliefs or religion,” and “not living in a peaceful or safe place.” We decided to remove these items unless there was a theoretical reason to keep them in the instrument.
Three of these items could actually be removed from the list: “struggle with beliefs or religion,” “feeling anxious,” and “not living in a peaceful or safe place.”
As far as the item “too little privacy” is concerned, earlier research has shown this factor to be influential in personal dignity (19,27,28). However, this can be expected to apply primarily to patients who live in care homes, nursing homes, or hospices. In our study, most people live at home, where their privacy is probably not hampered. As we want the instrument to be useful also for people who stay in an institution, we decided not to remove this item from the list.
The items “impaired hearing” and “not able to speak clearly or understandably” were added to the instrument as a result of the findings in the study with the prototype PDI (spring 2007), in which it appeared that items about “the ability to communicate” were lacking in the prototype. However, in this new measurement round of the cohort (autumn 2008), these items were barely present and scarcely exerted influence on dignity (Tables 2 and 3). Because this was quite different from what we had expected (based on the results of spring 2007), we would like to give these items another chance for inclusion by combining and reformulating them into “My impaired hearing or speech hampers me in the communication with others.”
The item “impaired sight” was ranked above average on presence, while its influence on dignity was small (Tables 2 and 3). This could mean that people with slightly impaired sight easily resolve this with glasses or lenses, which apparently has no influence on dignity. From now on, to include only those respondents who have a genuine problem with impaired sight, this item could be reformulated as “Even wearing glasses or lenses, I am not able to see very well.”
By calculating correlations between items that seemed conceptually similar, we were able to remove one more item from the instrument: “not receiving all care I need.” This item correlated significantly high with “receiving too little attention and care from people around me” in both the NVVE (r = .73) and NPV sample (r = .99). We chose to remove the first item, “not receiving all care I need,” because it is less specific than the other.
After making these changes, the new measurement instrument consists of 26 items, categorized as follows: (I) evaluation of self in relation to others (8 aspects), (II) functional status (9 aspects), (III) mental state (4 aspects), and (IV) care and situational aspects (5 aspects). The revised instrument can be found in the Appendix.
Discussion
Few many studies focus on factors affecting self-perceived dignity. We evaluated a measurement instrument consisting of 31 factors that asked about the extent of (a) being present and, if so, (b) exerting influence on dignity. Because the mean scores and ranking orders for these two concepts showed large differences and no overall correlation was found, a distinction can be made between these two concepts with regard to self-perceived dignity in practice. Based on the mean scores for presence and influence on dignity and on the inter-item correlations, four items could be removed from the instrument and two items could be combined into one item. This relatively small reduction in the number of items listed shows the variety in aspects that patients ascribe to their sense of dignity, which was also reported by Chochinov et al. (19).
Study population
The instrument was addressed to a cohort of Dutch people with one or more ADs. This study population is not representative of the Dutch population, since only 7% of the Dutch adult population possesses an AD (29,30). However, because concerns about loss of dignity are an important reason to draw up an AD, many participants in this cohort have probably thought about dignity and end-of-life-issues before the issues arise and are likely to have more exceptional views on these issues than the general public. The NVVE and NPV represent the most extreme opposite perspectives on euthanasia and physician-assisted suicide in the Dutch population and, therefore, probably cover the whole range of existing ideas on these issues. In a model with causal indicators, it is important to cover all aspects considered as being influential to dignity to ensure a good content validity. Choosing this study sample makes it likely that all relevant aspects for dignity have been covered.
Most of these people in this study were not yet in their last phase of life. By selecting ill and severely impaired people, we tried to create a sample in which personal dignity might be threatened. Nevertheless, only 10% of this sample population lived in care homes or nursing homes. Some aspects probably become more important for personal dignity for those who live permanently in an institution. This may explain the low mean scores found for the presence of items in the domain “care and situational aspects.” Taking into consideration that we selected the study sample by using the EQ-5D questions, of which three questions measure functional aspects, the high mean scores for presence in the domain “functional status” are not surprising.
The development of the instrument
The reason for developing a new instrument was the recognition that the prototype PDI had some imperfections. At that time, the revised version of the PDI did not yet exist. In this revised version, items about care were added and items were made more concrete. Apparently, Chochinov et al. had similar ideas about the shortcomings of the prototype PDI. However, while the revised PDI consists of only one question about the extent to which an aspect has been a problem or concern, we consider it important that the instrument distinguishes between presence of an item and its influence on dignity. Nevertheless, calculations showed weak relationships between the extent to which an item (a) occurs and (b) affects dignity. Because the focus of the instrument is self-perceived dignity, it is important to know whether an item is present but not essential to know to what extent an item is present. Hence, to shorten the list even more, the question for presence can be revised as a “yes or no” item (Fig. 2).
Revised questions about personal dignity.
Representation of the model of dignity in the terminally ill
The themes of the model of dignity in the terminally ill (19), “illness-related concerns,” “social dignity inventory,” and “dignity conserving repertoire,” are represented well in our instrument. The items in domains II, “Functional status” and III, “Mental state,” largely correspond to the themes and sub-themes of the category “Illness-related concerns” in the model. The domains I, “Evaluation of self in relation to others,” and IV, “Care and situational aspects” mainly contain elements of the categories “Dignity-conserving repertoire” and “Social dignity inventory” in the model.
In the dignity model, the “dignity-conserving repertoire” forms a buffer between “illness-related concerns” and “social dignity inventory” on the one hand and “dignity” on the other hand (19). A limitation of the measurement instrument is that it cannot reflect the inter-relatedness among the three categories in the dignity model; the instrument can only measure the influence on dignity for each item separately. To understand the relationship between several items with regard to self-perceived dignity, in-depth interviews are more suitable.
Conclusion
To provide dignity-conserving care, it can be useful for caregivers to identify which factors affect a patient's self-perceived dignity. Reducing the number of items listed and dichotomizing the answer options for the question about presence increased the feasibility of the instrument for use in practice. This quantitative instrument to measure factors influencing personal dignity can give insight into the factors that constitute dignity and could help improve dignity-conserving care and research on end-of-life care. For it to be useful in end-of-life care, more research regarding this instrument in different settings of this field is required.
Footnotes
Acknowledgments
This work was supported by funding from the Pieter van Foreeststichting, NVVE, and NPV. The authors gratefully acknowledge the assistance of Pam Kaspers and Matthijs van Wijmen in piloting development of the instrument, and Faith Maddever in translating the original Dutch questionnaire into English for international publication.
Author Disclosure Statement
No competing financial interests exist.
Appendix. The Complete (Revised) Instrument
The term dignity is often used when speaking about the final phase of life. We would like to find out as much as possible about what influences a person's sense of dignity.
If an item does not apply to you, please continue to the next item on the list. However, if an item does apply to you we would like you to answer question b.