
Abstract
Abstract
Purpose:
To describe health care utilization (HCU) at the end of life in cancer patients. These data are relevant to plan palliative care services, and to develop training programs for involved health care professionals.
Methods:
The Dutch Bone Metastasis Study (DBMS) was a nationwide study proving equal effectiveness of single fraction palliative radiotherapy compared with multiple fractions for painful bone metastases in 1157 patients. The 860 (74%) patients who died during follow-up were included in the current analysis. The main outcome was the frequency of hospital-based (outpatient contact or admission) and/or general practitioner (GP) contact during the last 12 weeks of life. Changes in HCU towards death were related to data on quality of life and pain intensity using a multilevel regression model.
Results:
Hospital-based HCU was reported in 1801 (63%) returned questionnaires, whereas GP contact was stated in 1246 (43%). In 573 (20%) questionnaires, both types of HCU were reported. In multilevel regression analyses, the frequency of outpatient contacts remained constant during the weeks towards death, whereas the frequency of GP contacts increased. Lower valuation of quality of life was related to both GP- and hospital-based HCU.
Conclusions:
There was a high consumption of hospital-based HCU in the last 12 weeks of life of cancer patients with bone metastases. Hospital-based HCU did not decrease during the weeks towards death, despite an increase in GP contacts. Future planning of palliative care and training programs should encompass close collaboration between medical specialists and GPs to optimize end-of-life care.
Introduction
Although much is known about preferences, data on actual health care utilization (HCU) in the last weeks of life are scarce. 9 These data are needed for accurate planning of palliative care facilities, and development of training programs tailored to the health care professionals involved.
The Dutch Bone Metastases Study (DBMS) was a prospective randomized landmark trial, proving equal effectiveness of single fraction palliative radiotherapy compared with multiple fractions for painful bone metastases in 1157 patients.10–13 During frequent follow-up, besides pain intensity, HCU and quality-of-life items were measured. Eight hundred and sixty (74%) patients died during the study period. Therefore, data from the DBMS provide a unique opportunity to analyze HCU at the end of life in cancer patients in relation to self-reported pain and quality of life.
This study aimed to describe HCU during the last weeks of life in patients with painful bone metastases. The hypothesis was that hospital-based health care workers cared for patients requiring complicated care (reflected by higher pain levels and lower quality of life) compared with the patients cared for by general gractitioners (GPs).
Methods
Patients
The current analysis included all patients who died during the follow-up of the DBMS. A detailed description of the in- and exclusion criteria, as well as the baseline and follow-up measurements in the DBMS have been published previously.10–12 Between March 1996 and September 1998, 1157 Dutch patients with painful bone metastases from solid tumors were randomized between a single fraction of 8 Gy versus six fractions of 4 Gy. In December 1998 the follow-up ended, data on survival of all randomized patients was updated, and the trial was closed. 11
Questionnaires
After baseline measurements, weekly questionnaires were sent to the patients during the first 12 weeks after randomization. Thereafter, monthly questionnaires were sent for a maximal period of 2 years or until death or end of study follow-up. Each questionnaire covered the preceding week and consisted of questions concerning HCU, quality of life, and pain intensity.
As end-of-life care was the interest of the current analysis, only the questionnaires returned in the last 12 weeks of life were included.
Health care utilization
The questions on HCU covered GP contact (Have you visited your GP this week?), outpatient visits (Have you visited your treating physician in the hospital this week?), and hospital admissions (Have you been admitted to the hospital this week?). The answer options were “yes” or no.” Patients could indicate more than one type of HCU in each questionnaire. Outpatient and inpatient hospital care was provided by the same health care professionals. Therefore, hospital-based HCU was defined as an outpatient contact and/or a hospital admission. No data on medical or psychological reasons for a health care contact or the actual place of death were collected in the DBMS.
Quality of life
The questions regarding quality of life were derived from the Dutch version of the Rotterdam Symptom Checklist (RSCL; see Appendix). 14 The RSCL consists of three subscales (physical symptom distress, psychological distress, activity impairment level) and an overall valuation of quality of life. The physical and psychological distress was measured using a four-point Likert-type scale, ranging from “not at all” (=1) to “very much” (=4). For the activity impairment level subscale, responses ranged from being “unable” (=1) to perform the stated activity to doing so “without help” (=4). The overall valuation of quality of life was measured on a seven-point Likert-type scale, ranging from feeling “excellent” (=1) to “extremely poor” (=7).
The RSCL scores were calculated per questionnaire according to the RSCL guidelines. 14 Per questionnaire, the sum-score of each RSCL subscale was calculated. Only when more than 50% of the items of a subscale were answered, was a standardized score calculated. 14 Standardization transformed the sum-score to a 100-point scale, by expressing the sum-score as the percentage of the maximal possible sum-score. In calculating the maximal possible sum-score, the missing items were taken into account. Conform RSCL guidelines and for consistency with the physical and psychological distress level subscales (in which a low score corresponds with low distress) the activity impairment level subscale and overall valuation of quality-of-life score were reversed. 14 On the reversed subscales a low score represents a low impairment of activity and a low overall valuation of quality of life, respectively.
These standardized and subsequently reversed scores were used to describe quality of life and will be further referred to as “RSCL scores.”
Pain intensity
In each questionnaire, the pain intensity was reported using an 11-point numeric rating scale ranging from 0 (=no pain) to 10 (=worst imaginable pain). Patients also noted their pain medication intake in the preceding week.
To take into account analgesic usage, inadequately treated pain was defined as having a pain intensity of at least 5, without opioid usage. 15
Statistical analysis
In all patients who died during the DBMS follow-up period, baseline characteristics were tested between those who answered HCU questions (“yes” or “no”) and those who did not (no answer at all). The tested baseline characteristics were: age, sex, urbanity (defined as≥1000 surrounding addresses/km2), primary tumor, number of bone metastases, time period from diagnosis of the primary tumor to randomization, randomization arm, Karnofsky performance status at randomization, systemic treatment at randomization and time period from randomization to radiotherapy, and survival after radiotherapy. Mann-Whitney tests were used to compare quantitative and ordered data; χ2 tests were used to compare proportions.
To study the relation of HCU to quality of life and pain intensity during the weeks before death, as well as to possible clinical relevant baseline characteristics (age, sex, primary tumor, and urbanity) multilevel logistic regression models were used. Missing questionnaires were assumed to be distributed at random, as this model adjusted for possible confounding factors. Patients were on the highest level, and repeated measures on the lowest level. Several response measures were analyzed, namely sex, primary tumor, urbanity, and inadequately treated pain. For each binary outcome measures the probability of getting a certain health care contact was modelled. Different determinants were included, namely age, pain intensity, and RSCL scores.
P values are based on two-sided tests, and considered significant if p<0.05. In the multilevel analysis, odds ratios (OR) were considered significant if the 95% confidence interval (CI) did not include 1.00. The statistical analysis was performed using SPSS version 16.0 for Windows (SPSS Inc., Chicago, IL), whereas the multilevel analysis was performed using MLwiN2.02 (Centre for Multilevel Modeling, University of Bristol, Bristol, United Kingdom).
Results
Patients and questionnaires
During the follow-up time of the DBMS 860 patients died (74%). In the last 12 weeks of life, the patients who died during follow-up time of the DBMS received 5189 questionnaires (Fig. 1). Six hundred and sixty one (77%) patients returned questionnaires in the last 12 weeks before death, and 627 (73%) answered HCU questions. A total of 3277 (63%) questionnaires were returned. In 2865 questionnaires (55 %) HCU questions were answered.
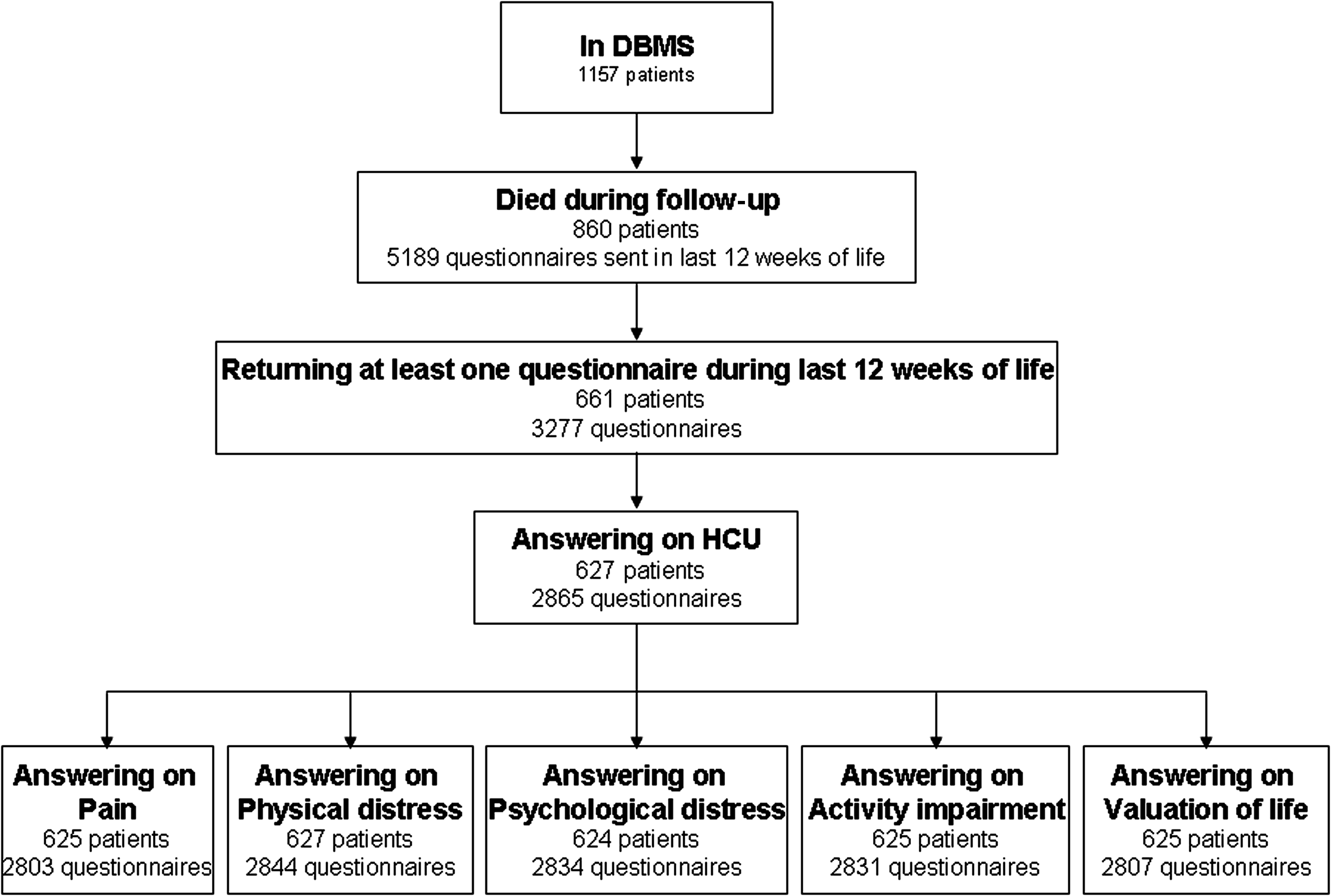
Consort diagram of patients and questionnaires included in current analysis.
Table 1 lists the baseline characteristics of all deceased patients in the study. Patients who did not answer HCU questions were mostly women, patients with breast cancer, and patients with a longer interval from diagnosis of the primary tumor to randomization into the DBMS.
Health care utilization
In any of the 12 weeks before death, a hospital-based HCU (either an outpatient contact or an admission) was reported in 1801 questionnaires (63%), and a GP contact in 1246 questionnaires (43%). In 573 questionnaires (20%), both a GP contact and a hospital-based HCU contact were reported. Fig. 2 depicts the HCU as reported in the questionnaires.

Health care utilization (HCU) reported in questionnaires. The circles indicate the number of questionnaires answering questions on HCU. The overlapping areas indicate the questionnaires stating more than one health care contact.
The reported health care contacts per week before death are shown in Fig. 3. Of the 627 patients answering the HCU questions, 396 (63%) reported during the last 12 weeks of life a GP contact as well as a hospital-based health care contact.

Health care utilization per week before death.
The mean pain intensity and the RSCL subscale scores of the questionnaires regarding specific HCU are presented in Table 2. In questionnaires that answered HCU questions with “no”, the pain scores were similar, but the overall quality of life was higher, compared with questionnaires that stated one or more health care contacts. Factors related to HCU in multilevel regression analysis are presented in Table 3. Reporting no HCU was related to a higher overall valuation of quality of life.
N: number of questionnaires. Pain intensity: measures with 11-point numeric rating scale (0=no pain, 10=unbearable pain). Inadequately treated pain: percentage of questionnaires reporting pain intensity of at least 5, without opioid usage. RSCL: Rotterdam Symptom Checklist; 100 points subscales. For physical symptom distress, note that a higher score=more distress. For psychological distress, note that a higher score=more distress. For activity impairment, note that a higher score=more impairment. For overall valuation of quality of life, note that a higher score=a higher valuation of overall quality of life.
Nonurban:<1000 surrounding addresses/km2. Urban:≥1000 surrounding addresses/km2. Pain intensity: measures with 11-point numeric rating scale (NRS; 0=no pain, 10=unbearable pain). Inadequately treated pain: percentage of questionnaires reporting pain intensity of at least 5, without opioid usage. RSCL: Rotterdam Symptom Checklist; 100-point subscales. For physical symptom distress, note that a higher score=more distress. For psychological distress, note that a higher score=more distress. For activity impairment, note that a higher score=more impairment. For overall valuation of quality of life, note that a higher score=a higher valuation of overall quality of life. OR, 95% CI: odds ratio with 95% confidence interval. Bold Italic: confidence interval not including 1.000.
Having reported a GP's contact was independently related to living in a nonurban area, being of higher age, being closer to death, having more physical symptom distress, and having a lower overall valuation of quality of life. It was also related to having adequately treated pain.An outpatient contact was independently related to younger patients, lower activity impairment level, and a lower overall valuation of quality of life. The frequency of outpatient contacts did not change significantly during the weeks before death.
Admission to a hospital was independently related to patients reporting more physical symptoms and a higher activity impairment level. When we analyzed the effect of different primary tumors, patients with lung cancer were less likely to be admitted to a hospital than patients with breast cancer, prostate cancer, or other types of cancer.
Fig. 4 present the chance for a specific type of health care contact towards death for each tumor group, based on the multilevel regression model. Although towards death the frequency of GP contacts increased and the frequency of no HCU decreased, the frequency of outpatient contacts remained stable.
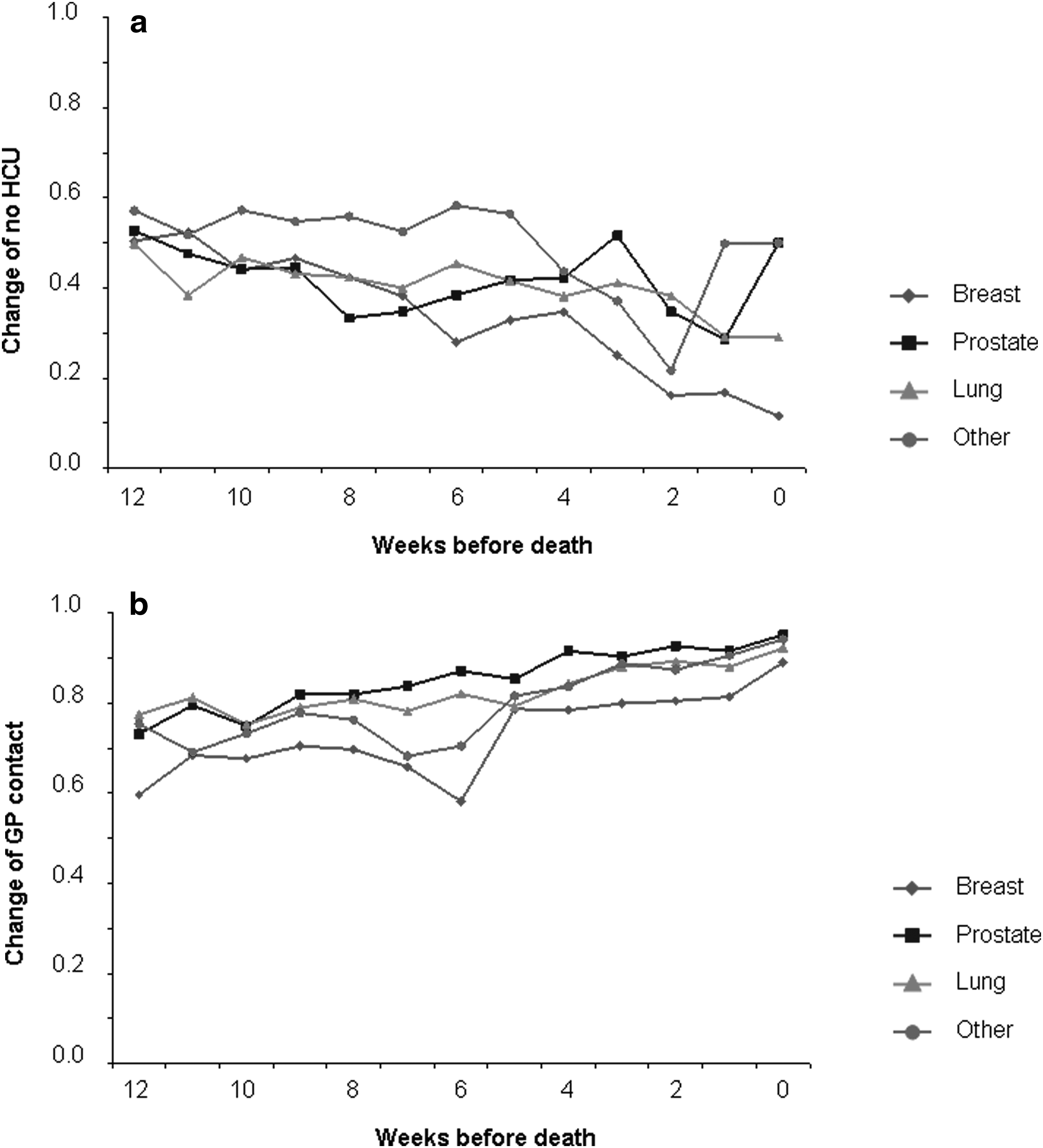
Chance for specific health care utilization (HCU) as modelled by the multilevel regression analysis.
Discussion
The current descriptive analysis provides evidence that hospital-based health care was frequently used during the last 12 weeks of life in patients with painful bone metastasis: 63% of the returned questionnaires stated a hospital-based health care contact. This is in contrast with the preference to be cared for at home. Although patients may require specialized care, travelling to a hospital is often burdensome. In the majority of cases the care needed may also be provided by specialized palliative home teams. This highlights the urgency of adequate training programs for involved health care professionals and for accurate planning of care. This may enable patients to be cared for and die at home and to avoid inappropriate hospital visits.16,17
Baseline characteristics
Patients who answered HCU questions appeared to have a more limited survival after radiotherapy compared with patients not answering these questions. This patient selection is likely to be a consequence of the original study design: Duringthe first 12 weeks after randomization into the DBMS the questionnaires were sent weekly; thereafter they were sent at a monthly interval. Therefore, patients who died within 12 weeks after randomization (n=274, 32%) received more questionnaires during their last 12 weeks of life, compared with patients who died later during follow-up.
The difference in survival after radiotherapy was related to the difference in primary tumor, time from diagnosis to randomization, sex, and systemic treatment at randomization. This is due to the characteristics of the several tumor types, as well as their treatment options. Lung cancer patients, often male patients, were more likely to have a shorter survival compared with breast cancer patients. Furthermore, at the time of the DBMS, palliative systemic therapy for lung cancer was less often used. 18 This is also likely to be the explanation for the significant OR for admission to the hospital for this tumor type (OR: 0,37; 95% CI: 0.15–0.90). As lung cancer patients composed 33% of the study population, hospital admission rate found in the DBMS may underestimate hospital admissions for today's care.
Health care utilization
Towards death the percentage of GP contacts increased. In previous studies, GP involvement was found to improve palliative home care and to be related to more home deaths.19,20 Therefore, the high percentages of GP contacts near death seem in line with known patients' and caregivers' preferences.1–5 Unfortunately, in our analysis, the type of HCU during the weeks before death could not be related to the place of death, as this was not registered in the DBMS database. During the study years, specialized end-of-life home nursing care was generally available in The Netherlands.
In 20% of the questionnaires, hospital-based HCU was reported together with a GP contact. As the questionnaires covered a time frame of one week, this percentage is a lower estimate. Using the broader time frame of all 12 weeks studied, the percentage increased to 63%. Even this percentage is likely to be an underestimation, as not all 12 weeks before death were covered with questionnaires: only during the first 12 weeks after randomization were the questionnaires sent in a weekly interval and thus covered all possible visits.
Remarkably, the increasing percentage of GP contacts towards death was not accompanied by a decrease in hospital-based contacts. In a meta-analysis it was shown that improvements in patient care can be expected from interactive communication between primary care health care workers and specialists. 21 Therefore, one would expect that close collaboration between GPs and medical specialists will reduce the need for outpatient contacts. This concept is one of the central ideas in the gatekeeper position of the GP in the Dutch health care system, which resembles the function of the personal physician in the Patient Centred Medical Home project in the United States.22–24 In our analysis, GP contacts did not reduce hospital-based HCU during the last weeks of life. One reason might be that outpatient visits have their own value for patients. Although information regarding the medical or psychological reasons for HCU was not registered in the DBMS, we suggest that aspects of hope and reassurance can be important reasons for outpatient visits. Furthermore, patients may visit the GP for other reasons than the visits to the outpatient clinic. For instance, the GP is likely to be contacted more often for psychosocial support, whereas hospital-based health care is more likely to be used for somatic reasons. However, evidence to underpin these suggestions is lacking in the literature, although first attempts have been made.25,26
Data regarding the specific reasons for visiting a GP oroutpatient clinic or for admission are necessary. Firstly, these will show whether the several health care services are used for the reasons for which they are meant. Secondly, combined with information regarding the place of HCU, these data are essential to develop effective training programs. For maximum patient benefit, proper knowledge of all aspects of palliative care such as the range of (non)pharmaceutical treatment options, medical intervention strategies, and comprehensive care facilities is needed by all involved health care workers.
Pain and quality of life
In the multilevel analysis, pain intensity was not related to any type of HCU. Apparently, an increase in pain intensity did not independently increase the probability to visit a GP and/or the hospital during the last weeks of life. Contrary to this, a lower valuation of quality of life was related to more GP and/or hospital contacts. Although these findings did not support our initial hypotheses, they underline the importance of focussing on overall quality of life instead of separate physical symptoms such as pain, when studying or planning health care utilization.27,28
Study limitations
The presented study was a further descriptive analysis of the prospectively randomized DBMS. As selection bias may have occurred, given significance levels are estimates and should be interpreted with caution.
Fifty-five percent of the questionnaires sent during the last 12 weeks of life answered questions on HCU and were included in this analysis. Considering the closeness to death of the responders, this is a reasonable response rate.
It was assumed that the missing questionnaires were missing at random, given the characteristics included in the multilevel logistic regression model. Because these characteristics are also related to drop-out, we think that this is a reasonable assumption.
Since the DBMS ended in 1998, palliative care for patients with painful bone metastases has changed. Patients with a disseminated cancer live longer as a result of improved systemic therapies. In addition, the focus is more on active symptom control. These changes can have contrary effects on hospital-based HCU. On the one hand, systemic treatment for disseminated lung cancer has been developed, which is likely to increase hospital-based HCU. 18 On the other hand, in The Netherlands, since 1998 palliative care is promoted by a governmental stimulation program, focusing on palliative care provided by primary care workers.6,29 Unfortunately, no direct data regarding the effect of these changes on place of end-of-life care are available at the moment. As a surrogate parameter, a recent study showed that the percentage of cancer deaths occurring in Dutch hospitals slightly increased from 28% in 1996 to 31% in 2003 and 2006.30–32 Together with the increasing incidence of cancer during that period, 33 this indicates the relevance of the current analysis for today's care.
Conclusions
There was a high consumption of hospital-based HCU in the last 12 weeks of life by cancer patients with bone metastases treated within the DBMS. This type of HCU did not decrease during the weeks towards death, despite an increase in GP contacts. In multivariate analysis, lower overall valuation of quality of life was related to both GP and hospital-based HCU. This emphasizes the importance of integrated palliative care, in which medical specialists as well as GPs have close collaboration and both have knowledge regarding palliative care issues and treatment possibilities. Training programs focusing hereupon need to be developed. In the future, specialized care can then be provided at home or in the hospice so that the preference of patients to stay and die at home or in a home-like setting can be granted.
Footnotes
Acknowledgments
J. J. Meeuse received financial support from the Comprehensive Cancer Centre North-Netherlands. None of the other authors received any financial funding for this study.
Author Disclosure Statement
No competing financial interests exist.
Appendix. Rotterdam Symptom Checklist
Would you please check whether you answered all questions?
Thank you for your help.