
Abstract
Abstract
Objective:
Qualitative research is becoming more common in pediatric palliative care and end-of-life care. The present article systematically reviews and summarizes qualitative and survey-based research on pediatric palliative and end-of-life care pertaining to the needs of patients and their families.
Method:
Twenty-one qualitative and survey-based studies published between 2000 and 2010 that met the selection criteria were retrieved from MEDLINE, PsycINFO, and CINAHL. All studies reported on the needs of patients and families receiving pediatric palliative and end-of-life care—from either the patient's, parent's, sibling's, or health care provider's perspective. Findings from these studies were aggregated using a metasummary technique.
Results:
Findings were extracted and grouped into the following 10 thematic domains pertaining to patient and family needs: interactions with staff, health care delivery and accessibility, information needs, bereavement needs, psychosocial needs, spiritual needs, pain and symptom management, cultural needs, sibling's needs, and decision making.
Conclusions:
The results of this metasummary highlight the needs of patients and families to be taken into consideration in the creation of high-quality pediatric palliative and end-of-life care services and guidelines.
Introduction
There are numerous studies and recommendations for palliative care for adults that have led to an increase in services and improved care for adult patients. In contrast, only in the last decade has there been a rise in research in pediatric palliative care (PPC) and pediatric end-of-life care (PEOLC). While the provision of PPC services has been found to ease children's suffering and provide an improved end-of-life care environment for children, 4 more research in the area is imperative, as adult literature in palliative and end-of-life care cannot easily be applied to children.5,6 Moreover, the research to date suggests that U.S. and Canadian health care systems do not adequately meet the needs of children with life-threatening and life-limiting illnesses or those of their families.7–11 In order to address this deficiency, several North American organizing bodies have provided guidelines for health care providers (HCPs) and hospitals to improve the situation of patients and families receiving PPC or PEOLC.2,3,12,13
Currently, much of the research on PEOLC and PPC is qualitative in nature. Quantitative studies give a very valuable but often partial description of complex processes such as parental bereavement; whereas qualitative studies offer a complementary in-depth exploration of human experience.14,15 Recently there has been a push to synthesize qualitative research so that it may be used for evidence-based practice. When qualitative studies in a particular topic area are taken together—through systematic techniques such as metasummary—the collected findings allow for an accurate representation of the universal concepts relevant to the topic.16,17–19 In the present article, qualitative and survey-based research from the perspectives of families, patients, and HCPs on the needs of patients and families receiving PPC or PEOLC is subjected to a metasummary with a view to inform guidelines and to ensure that they are up to date.
Methods
Metasummary methodology
Metasummary is a type of systematic review where qualitative and descriptive quantitative findings are collected from topical or thematic surveys of the data through a review of the relevant literature.17,20 Sometimes used as a precursor to metasynthesis, this method involves extracting findings from various studies, then grouping these findings and abstracting common findings based on topical and thematic similarities.16,20–23 In qualitative metasummary all findings are given equal relevance regardless of specific qualitative methodology and without prior evaluation of methodological quality. In qualitative research the method stated is often found to be neither an indicator of the method actually used nor does it influence the findings.18,19 Therefore, we extracted findings from articles that were relevant to our research question and objective and did not analyze the exact methodology used other than assuring that it is qualitative, survey-based, and amendable to the techniques of metasummary (i.e., topical or thematic summaries of the data). The following two calculations were then performed to give an indication of the occurrence of particular findings and impact of particular articles (see Figure 1).17,23,24 The proportional frequency of the finding (PFF) indicates the number of times a finding is reported across all included articles; the proportional intensity of the article (PIA) calculates the total number of findings extracted from a given article.17,23,24 Readers familiar with metasummary and metasynthesis techniques may be accustomed to seeing the terms frequency effect size and intensity effect size used to denote PFF and PIA, respectively.17,23,24 To avoid confusion, however—especially among those for whom the term ‘effect size’ has a particular and uninfringeable meaning—we have herein opted to employ the terms PFF and PIA for descriptive clarity.
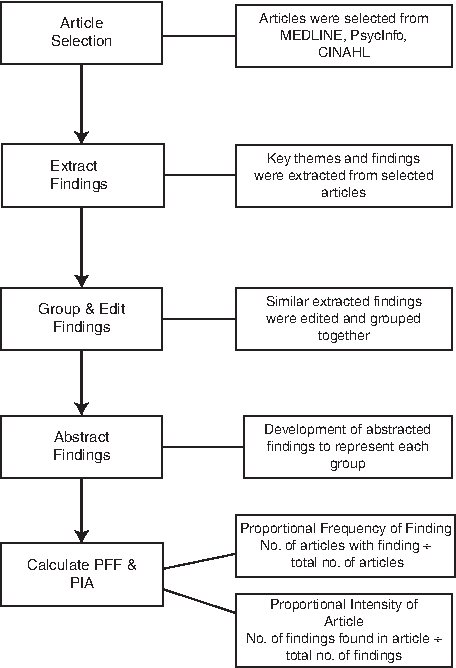
Metasummary procedure. PFF, Proportional frequency of finding; PIA, proportional intensity of article.
Article retrieval
We conducted a comprehensive literature review using MEDLINE, PsycInfo, and CINAHL databases. Keywords used for database searching fell into three linked categories: (1) child*, pediatric, paediatric, or adol*; (2) end-of-life, terminal*, or palliative; and (3) hosp*, service, program, need, or perspective (*denotes truncation). To confirm that the retrieved sample comprehensively represented the existing publications on the topic, we scrutinized bibliographies from the included articles and related clinical recommendations and literature reviews. The search was last updated in January 2011.
Inclusion and exclusion criteria
In order to be included in our review, articles had to (1) focus on perspectives of either parents, patients, or HCPs in Canada or the United States on aspects of PPC and PEOLC; (2) empirically examine these perspectives using thematic surveys, surveys with open-ended question, and/or qualitative methods; (3) be published in an English peer-reviewed journal; and (4) be published between 2000 and 2010. We chose a 10-year time frame to highlight the increases in both qualitative health research and PPC services at this time and to provide a current and up-to-date review. We included studies conducted in either Canada or the United States in order to collect findings that would be specifically relevant to patients, families, and HCPs in Canada and the United States, as these two countries serve similar populations and are at similar stages of development of PPC programs.7,25,26 The aim of the current review is to give a snapshot of PPC services in Canada and the United States; therefore, research conducted in the United Kingdom, Australia, and other jurisdictions was not included, even though there is much research in PPC coming from these areas. Twenty-one articles met these criteria and were included in the review.
Procedure
Two authors (MS and TL) assessed the studies to determine if they were relevant to the review and recorded the research question or statement of purpose, research method, sample size, and participant characteristics (see Table 1). The articles were then metasummarized using techniques described by Sandelowski and Barroso (see Figure 1).16,17,19,23 Findings were considered any integrated conclusions and discoveries offered by researchers regarding the experiences they were studying.20,23 The research team (MS, TL, and MA) met on a regular basis to discuss how the findings would be grouped and to develop the abstracted findings to represent each group. Discrepancies between authors were discussed and resolved through consensus on the most accurate way of representing the finding. These findings were then grouped into thematic domains. For the calculation of PFF and PIA each report was treated as one unit of analysis and each finding was weighted equally.16,23,24 The PIA was calculated by dividing the number of findings extracted from one particular article by the total number of findings extracted in our review (see Table 2). The PFF was calculated by dividing the number of articles or studies with the particular finding by the total number of studies in our review (see Table 2).
Age of child at the time of death.
Age of child participant.
Age at time of diagnosis.
CPCCRN, Collaborative Pediatric Critical Care Research Network; PICU, pediatric intensive care unit.
PFF, Proportional frequency of finding.
PIA, Proportional intensity of article.
Results
Health care delivery and accessibility
Needs related to health care delivery and accessibility were cited in 13 of the 21 studies reviewed (see Table 2). Continuity, consistency, and coordination of care were reported in 11 of the studies and were the focus of the Heller and Solomon 2007 article. This form of care has been reported as serving to build relationships, promote caring, and encourage sharing of expertise and information about the child between HCPs. 27 HCPs have reported the need for patients to receive care outside the hospital.28,29 Home visits by HCPs and the ability to transition in and out of hospital are considered essential to high-quality pediatric palliative and end-of-life care.28,30 HCPs have also highlighted the importance of giving the child the choice of where to die. 28 However, parents have reported that community-based hospice programs are poorly prepared to serve pediatric patients. 30 Although descriptive research conducted with parents has reported that the number of deaths in the intensive care unit has decreased and hospice care discussions have increased and are occurring earlier, 31 parents have also reported several important obstacles to home death.30,32 Parents and HCPs have emphasized the need for services and competent pediatric trained HCPs to be available and accessible to families and patients from the time of diagnosis up until and including the bereavement period.28,33,35 In addition, parents have reported the occurrence of negative events and preventable oversights that may be addressed by staff that are more competent in PPC and PEOLC.30,32
Interactions with staff
Needs related to interactions with staff were highlighted in 13 of the studies reviewed and was the main focus of the Hsaio, Evans, and Zeltzer 2007 study (see Table 2). Interactions with staff were reported as problematic in 3 of the studies30,34,35 and needs in this area were mentioned in all 13. Parents, patients, and staff have all mentioned the importance for continual and ongoing relationships between staff and families and all want to be involved in discussions about the child's care.28,30,33–41 Furthermore, families have reported wanting a familiar person to deliver difficult news in a sensitive and caring manner.30,34,39 The manner in which staff communicate was divided into two groups: (1) parents want honest and straightforward communication30,33–35,39,40 and (2) parents want staff to show sensitivity, empathy, and competency when they communicate with them.27,28,33–35,38,40,41
Information needs
Information needs were mentioned in 9 out of the 21 articles reviewed (see Table 2). Five of the studies reported the simple need for more information.29,34–36,40 Parents and HCPs have noted that parents need to be prepared for what to expect from their child's illness and potential treatments.29,34 However, parents have reported feeling as if information was withheld from them and that they did not get updated as frequently as they wanted about their child's condition.35,40 Additionally, parents reported that the information given to them was often contradictory or confusing,34,35,40 especially for non-English-speaking families. 28
Bereavement needs
Bereavement needs were reported in 9 out of the 21 studies reviewed and were the main focus of the Macdonald et al. (2005) and D'Agostino et al. (2008) studies (see Table 2). Six of the studies reviewed reported parents wanting care to extend from the time of diagnosis through to the bereavement period.27,30,35,40,43 Families also mentioned developing a strong bond with the treating hospital and feeling abandoned if this bond was broken.40,41 Parents reported wanting mementos such as a handprint or a hospital bracelet;35,40 and they reported wanting staff involved in the child's care to follow up with them after the child's death with acts such as sending cards, attending memorial services, and telephone calls.35,40,43 However, parents have also reported that returning to the treating hospital can be emotionally challenging. 40 Parents have reported needing help to prepare for their child's death and to prepare for what to expect at the time of death, including funeral arrangements and bereavement counseling services.29,35,40,43 Moreover, parents want bereavement services to be available immediately after their child's death (or even before) and they want these services to be both flexible and consistent. 43 In line with the psychosocial needs, parents also desire contact with other families that have lost a child. 43
Psychosocial needs
Psychosocial needs were reported in nine of the studies reviewed and were the main focus of the Jones (2006) study (see Table 2). The psychosocial needs of patients and families have importance in their own right but also affect other needs. For example, the need for patient dignity and respect is reported in several studies as a patient need but is also cited as playing a crucial role in communication needs. 34 Parents and HCPs have reported that patients and families need emotional support,28,29,34,41,43 which includes services such as counseling29,41,43 or play therapy.28,29 Socially, patients, parents, and HCPs have reported that patients need access to peers and other children going through similar experiences.28,29,44 In addition, patients and HCPs have reported that patients need some semblance of a ‘normal’ life with developmentally appropriate activities.28,29,44 HCPs and parents have reported that parents need access to other families in similar situations.28,29 This finding is similar to the parent networking finding in the bereavement domain; however, this finding relates more to social support while the child is still alive, whereas the other finding relates to social support after the child has died (for example, through bereaved parents support groups). Lastly, along with needing social support from peers, families need unrestricted access to their child and vice versa,28,41 especially as the child approaches the end of life. 36
Spiritual needs
Spirituality was touched upon in eight of the studies and is the main focus of the Meert et al. (2005) and Robinson et al. (2006) studies (see Table 2). Some of the reported spiritual needs were more religious in nature, such as the need for prayer;41,45 whereas others are not necessarily associated with religion, such as the need for hope and for the child to be remembered after death. Parents have highlighted their striving to maintain hope while accepting their child's prognosis. 32 Bereaved parents have mentioned the transcendental quality of the parent-child relationship and the need to maintain a bond with their child throughout illness and after the child's death.28,36,40,41,45 Some of these parents have also mentioned their search to find meaning from their child's death by looking for the good their child has brought to others and finding reasons to go on living.33,41 To address some of these issues, parents have mentioned wanting guidance in line with their values28,41,45 and access to spiritual counselors or clergy.29,36,41,45
Pain and symptom management
Six of the reviewed studies mentioned the need to relieve pain and symptoms of patients (see Table 2). Two other articles related to pain and symptoms of PPC patients46,47 were identified, but the results in these articles were more inventories of pain and symptoms experienced by patients and did not frame the findings in terms of what is needed or lacking in pain and symptom management. In the included articles, when physicians were questioned about the needs of their patients, they reported that pain and symptoms need to be assessed consistently and managed effectively. 28 However, research involving parents and HCPs has shown discrepancies between the high degrees of pain reported by parents and HCPs' perceptions that pain was well managed.30,31 A crucial aspect of pain and symptom management is the need for the patient to be comforted and soothed.28,30 Despite the fact that alleviation of pain was reported by parents as very important, parents have also reported that they do not want alleviation of pain to impair consciousness or impact their ability to communicate with their child. 40 Interestingly, a study by Wolfe and colleagues (2008, not included) that compared a baseline cohort (1990–1997) to a follow-up cohort (1997–2004) found that parents reported their child to be suffering from pain and dyspnea less in the follow-up cohort. 31
Cultural needs
Cultural needs were reported in six of the studies reviewed (see Table 2). These findings were taken both from research conducted with parents of various languages and cultures30,36,37,48 (Mexican American, Chinese American, and Spanish-speaking families) discussing their needs and from research conducted with HCPs on their views of high-quality PPC and PEOLC.28,49 Families and HCPs have reported the importance of providing care and information that is culturally sensitive28,30,37,48,49 and fair. 48 Furthermore, parents who do not speak English face communication issues that may impede their child's treatment and their comprehension of what is happening to their child,30,36,37 which could be addressed by providing translators 28 and ensuring that non-English-speaking families know there are interpreters available. 37
Decision making
Decision-making needs were mentioned in six of the studies reviewed (see Table 2). We identified—and excluded—several studies with findings related to decision making but which were often in terms of factors involved in decision making (e.g., progression of the child's illness) rather than parent's and patient's needs when making decisions.50,51 In the included studies, parents and HCPs have reported the importance of treating patients and families with respect and allowing them to have a say in treatment decisions.28,29,41 Furthermore, families and patients need adequate information to support their decision making, including assessment of the goals of care.28,29,33,37
Siblings' needs
Five of the reviewed articles mentioned siblings' needs (see Table 2). HCPs have reported that care needs to be more family oriented28,30,49 and should involve siblings. 49 Families have reported that the impact on siblings is often underrecognized; 38 they do not receive the care they need 28 and parents lack information on how to support them.36,37 To address this need, parents and HCPs want more support and counseling29,30,36,44 and services for siblings.29,30,44
Discussion and Implications
This metasummary provides a comprehensive and global view of the needs of patients and families receiving PPC or PEOLC in Canada and the United States through the perspectives of patients, families, and HCPs. Through the collection and analysis of the qualitative and survey findings in the area, we have found that patient and family needs can be categorized around 10 general need domains: health care delivery and accessibility, interactions between staff and families, information needs, bereavement needs, psychosocial needs, spirituality needs, pain and symptom management, cultural needs, decision making, and needs of siblings. The PIA gives an indication as to how many findings one article contributed to the metasummary. The highest PIAs were found for the articles by Donnelly et al. (2005), Jones (2006), and Meert et al. (2005), respectively. These articles contributed the most findings to the metasummary, because these articles examined broadly the needs of patients and/or families receiving pediatric palliative or end-of-life care. Articles that had a lower PIA focused on specific aspects of care or needs such as cultural needs, bereavement care, etc. The high PFF of the health care delivery and accessibility needs and interactions with staff needs shows that these domains are touched on in many of the articles and are frequently mentioned as problematic by families and HCPs. Lower PFFs were found for sibling, decision making, pain and symptom management, and cultural needs. However, a low PFF does not indicate that there is less need in the area, but rather that these domains are less represented in the qualitative and survey-based research. In fact, all 10 domains are important in consideration of policies to address patient and family needs. Moreover, the domains and categories we have discovered are also in agreement with current guidelines in PPC and PEOLC, which emphasize the need for continuity and integration of care; 13 developmentally appropriate care; respect for patients and families; 2 care from diagnosis through to bereavement;2,13 attention to symptom and pain control; and the emotional, psychological, and spiritual needs of patients. 3 However, we have found that (1) many parents are still reporting these aspects of care as lacking or problematic and (2) there are more specific needs being reported by patients and families that should be addressed in guideline and policy creation.
Although every attempt was made to review the literature systematically and comprehensively, there remain several limitations to this metasummary. Firstly, this review was restricted to published literature and did not include theses or dissertations. Secondly, although several of the studies examined pediatric palliative care services or the care of seriously ill and dying children more generally,28,30,34–38,48,49 some of the studies were specific to children who died of cancer29,39,43,46 in the intensive care unit33,40–42,45 and in hospice.44,47 We did not compare findings across hospital units or type of illness, in that findings from intensive care, oncology, palliative care services, and hospices were grouped together, so that needs unique to these types of care were not highlighted specifically. Nonetheless, overall, the findings from the more specific studies agreed with the findings from the broader studies on general PPC services. Lastly, although this article highlights the general needs of PPC patients and families, there are important details in relation to specific illnesses and conditions beyond the scope of this metasummary that should be considered in guideline and policy creation.
This being said, this metasummary has several notable strengths. This metasummary provides a concise and comprehensive review of recent literature in PPC and PEOLC. By coalescing various studies taken from the perspectives of patients, families, and HCPs, we have gained insight into the needs of patients and families receiving PPC and PEOLC in Canada and the United States. Furthermore, by focusing on research conducted in these regions in the last decade we have produced a current snapshot of the most relevant and important needs in this field. Novel techniques such as metasummary provide a means to link qualitative research findings to evidence-based practice. By systematically summarizing qualitative research on these needs, we hope to aid clinicians in providing care that is most helpful to patients and their families and in assessing the extent to which additional services or resources may be needed to further develop their respective institutions to meet the needs of their clientele. This metasummary is part of a larger review of the needs in PPC and PEOLC of patients, families, and HCPs that we hope will further elaborate and guide clinical practice and research in PPC and PEOLC.
Our review highlights the most frequently reported needs (such as health care delivery and accessibility) as well as needs that are less frequently mentioned but equally important for clinicians and policy makers to address (such as sibling needs). However, there is a dearth of research on whether current services actually meet these needs, apart from a few studies on implementation of various PPC services45,50,51 or preliminary evaluations of implemented programs and services (such as the Davies et al. 2005 and Macdonald et al. 2005 articles reviewed herein). Therefore, there is still a great deal of research to be done to discover (1) how best to meet the needs of patients and families, (2) how to implement PPC services and PEOLC practices, and (3) if the implemented services and practices are able to meet the needs of patients and families.
Footnotes
Author Disclosure Statement
No competing financial interests exist.