
Abstract
Abstract
For difficult to treat neuropathic pain from cancer, adjuvant analgesics are often used with opioids. We present the case of a 5-year-old girl who was diagnosed with meningitis caused by malignant T-cell lymphoma. She had severe neuropathic pain not relieved by increasing doses of a fentanyl infusion. Intravenous administration of ketamine and lidocaine in combination with fentanyl provided excellent analgesia without significant side effects. Ketamine and lidocaine can be safely infused together with concomitant opioids for the treatment of refractory neuropathic pain caused by cancer.
Introduction
Case Report
A 5-year-old girl who had continuous cough and dyspnea underwent computed tomography that revealed a large tumor in the mediastinum. Examination of a biopsy specimen revealed the presence of lymphoblastic T-cell lymphoma. Malignant cells had metastasized to her bone marrow, and the lymphoma was judged to be a stage III tumor. She was administered chemotherapy comprising prednisolone, cyclophosphamide, daunorubicin, and
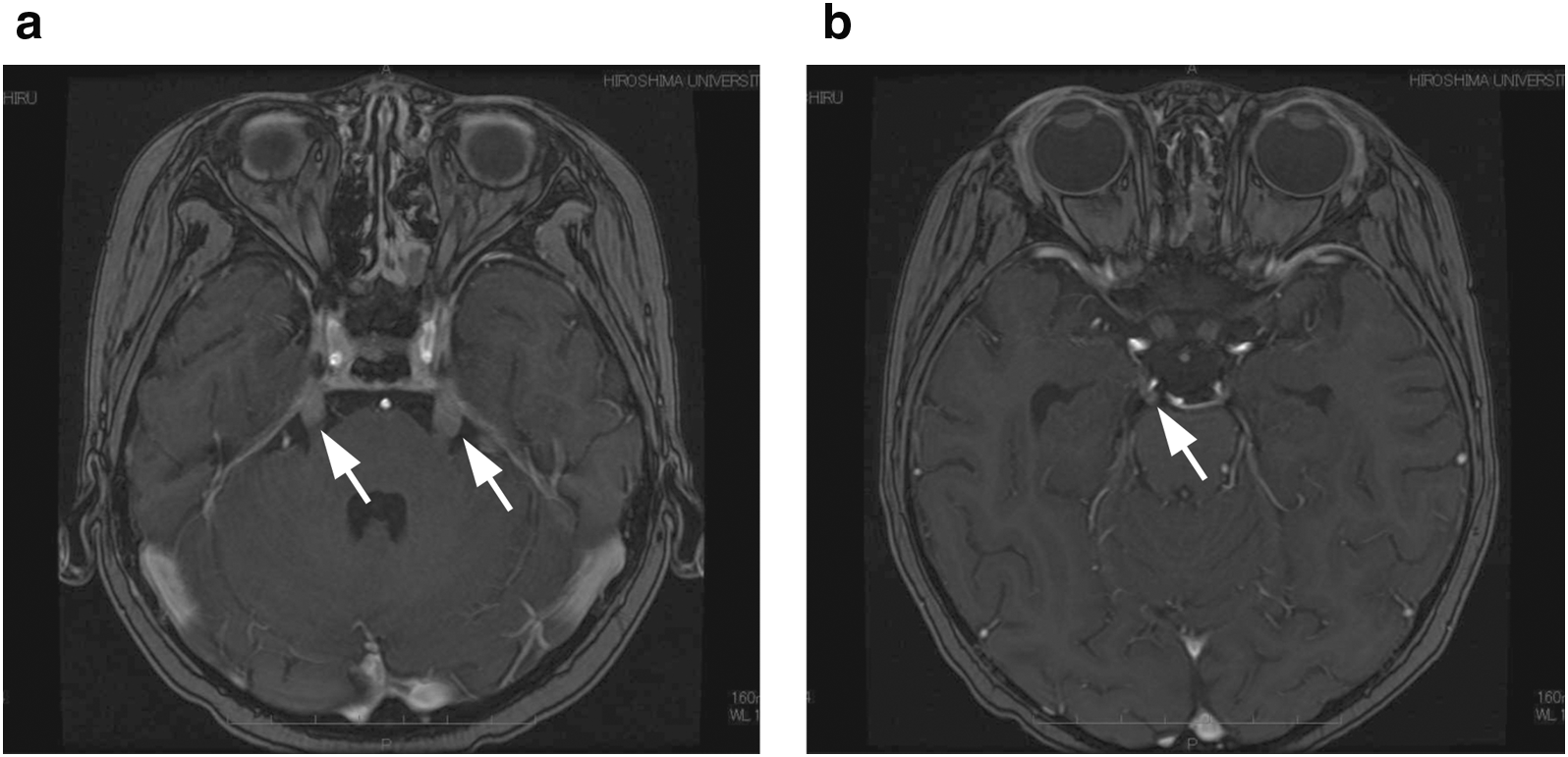
Enhanced MRI at the time of cancer-related meningitis. Contrast effect and swelling are seen at the right and left trigeminal
Subsequently, we co-administrated fentanyl with a continuous intravenous infusion of lidocaine (9.3–14 μg/kg/min) starting 62 days after transplantation because it was not possible to control the trigeminal neuralgia with the former. Cranial radiotherapy (3 Gy×9) was initiated on day 64 after transplantation. Following radiotherapy, the patient's facial pain and the visual disorder in the right eye improved transiently, but then recurred soon after. In addition, she developed new neck and right shoulder pain, likely due to leptomeningeal carcinomatosis. The cerebrospinal fluid cell count increased, and the level of LDH increased in the blood sample. Spinal cord irradiation (3 Gy×10) was initiated on day 82 after transplantation. Following radiation, the severe sharp pain of her neck and right shoulder did not change in severity. Because it was difficult for her to swallow oral medications, we could not prescribe gabapentin or other oral adjuvants for neuropathic pain. On day 89 after transplantation, we decided to initiate a continuous intravenous infusion of ketamine (0.12 mg/kg/h) in addition to the fentanyl and lidocaine infusion that the patient was currently receiving, in the hopes of improving analgesia for severe prosopalgia and neuropathic pain associated with leptomeningeal disease. Her severe pain was markedly relieved after the administration of ketamine, and she was able to lead a normal life of approximately 2 weeks with her family. She became unconscious on day 107 after transplantation and died on day 109. Figure 2 shows the summary of the clinical course.
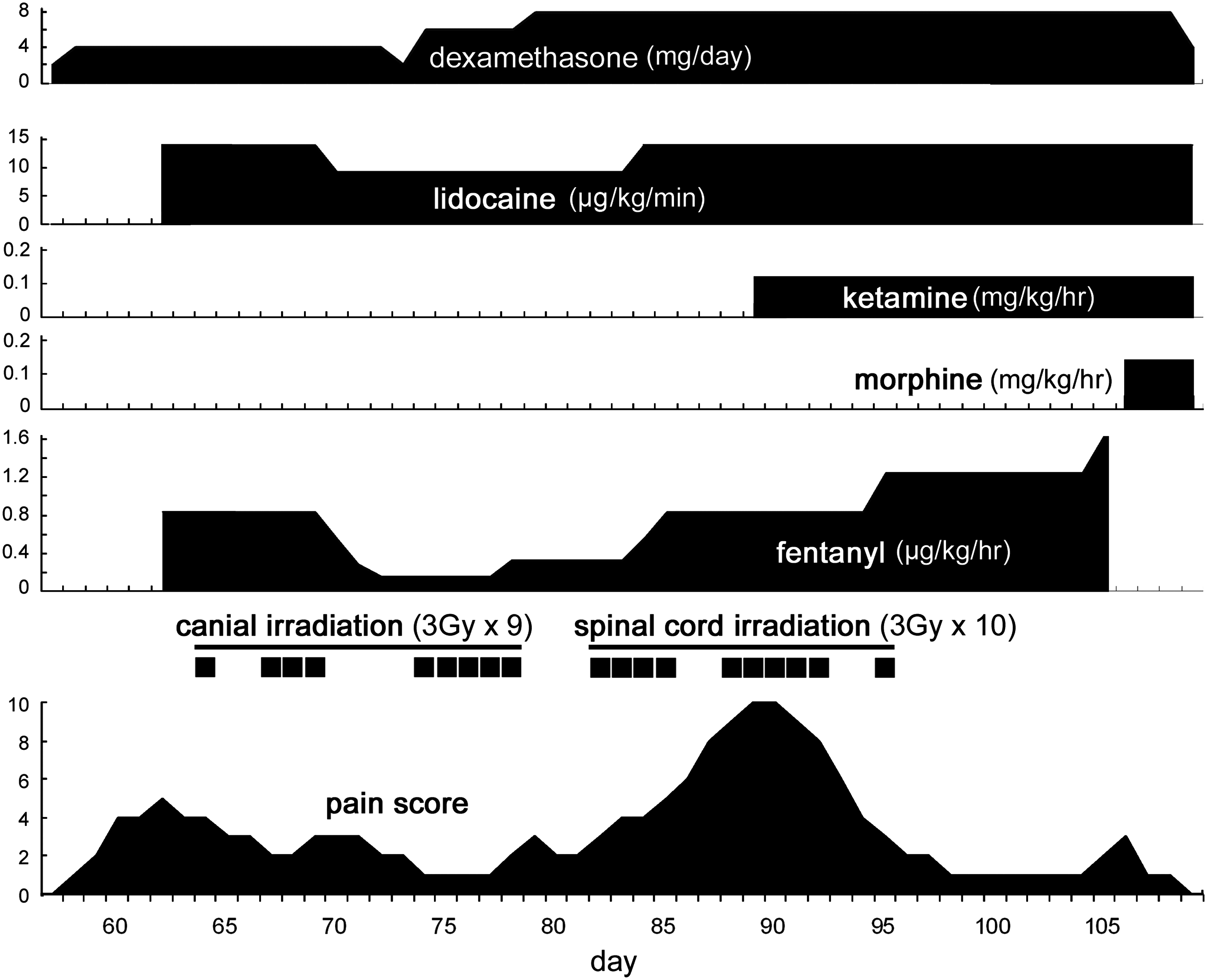
The summarization of the clinical course. Pain control was difficult by the administration of only opioids. A combination of lidocaine and ketamine was effective in controlling neuropathic cancer pain.
Discussion
We report the administration of continuous intravenous infusion of ketamine and lidocaine together with a fentanyl infusion for a case of severe neuropathic cancer pain. Almost all patients who have cancer pain are administered opioids such as morphine and fentanyl. Although opioids are first-line therapy for neuropathic pain in patients with advanced cancer, they are sometimes ineffective. Ketamine or lidocaine may be useful adjuvants in such cases.
Ketamine is a nonopioid anesthetic agent and N-methyl-Daspartate (NMDA) antagonist, and it is usually used for short diagnostic or surgical procedures. 13 The activation of NMDA receptors, which are the sites of action of the excitatory neurotransmitter glutamate in the spinal dorsal horn, is involved in central sensitization.14–17 Ketamine exerts its analgesic effect via attenuation of central sensitization.15–17 In addition, ketamine potentially attenuates the acquired opioid tolerance via NMDA antagonism.16–18 In our case, ketamine may have exerted an analgesic effect by attenuating central sensitization and opioid tolerance.
There is significant experience using ketamine in pediatrics and adolescents for perioperative pain management16,19 and for procedural pain.20–23 In addition, ketamine has been used for cancer-related pain given as an infusion.5,24–27 Infusion rates ranging from 0.084 to 0.6 mg/kg/h have been reported. 16 Another study, using subanesthetic doses of ketamine for pain relief in children and adolescents reports a dose range from 0.1 to 1 mg/kg/hour. 5 In our present case, a dose of 0.12 mg/kg/h of ketamine was effective.
Peripheral and central sensitizations contribute to the pathogenesis of neuropathic pain. Peripheral sensitization is induced by the aberrant expression and activation of sodium channels on damaged primary afferent neurons and adjacent neurons.28,29 Lidocaine is thought to exert an analgesic effect by blocking these sodium channels at low concentrations; thus, normal neurotransmission is not disrupted.28–31 The analgesic mechanism of lidocaine in relieving the central neuropathic pain in our case is unclear; however, some studies have shown the efficacy of lidocaine.12,30,32,33 In the present case, lidocaine may have exerted a central analgesic effect via the same mechanism as that of the peripheral analgesic effect.
The dosing of intravenous lidocaine for pain has not been well established in pediatrics. One study has reported that a lidocaine infusion of 35 to 63 μg/kg/min was successful in treating refractory pain in a pediatric patient. 12 Though it is not a report about children, the authors reported that the average lidocaine infusion rate was 1.5 to 5 mg/kg/h34–36 The lidocaine dose is possible to convert to 25 to 83 μg/kg/min. Our patient was administered a dose of 9 to 14 μg/kg/min of lidocaine. The lidocaine dosage used in this case was lower than previous reports; however, in combination with intravenous ketamine it seemed to be effective.
Conclusion
Although opioid therapy is considered to be first-line therapy for neuropathic pain associated with advanced cancer, many patients will not obtain relief. Often it is necessary to use different classes of pharmacological agents to treat refractory pain. The combination of ketamine, lidocaine, and fentanyl was safe and efficacious in this pediatric patient. Clinicians should use all available pharmacological and nonpharmacological approaches available and as appropriate. Our study suggests that there may be a role for combining adjuvant analgesics in a step-wise fashion to achieve good analgesia. However, more research is necessary to determine the efficacy of this approach versus rotation of adjuvant analgesics and/or opioids in the treatment of refractory neuropathic pain related to cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.