
Abstract
Abstract
Background:
Pain is one the most common symptoms experienced by palliative care patients. The treatment of pain involves the use of strong opioids such as hydromorphone, morphine, methadone, fentanyl, oxycodone, oxymorphone, or levorphanol for moderate to severe pain. Hydromorphone is metabolized by the liver to hydromorphone-3-glucuronide (H3G), a compound that can potentially cause neuroexcitatory phenomena with accumulation. Pharmacokinetic studies have shown that H3G levels in patients with renal insufficiency are 4 times as high as those with normal renal function; however, reports have been conflicting as to whether or not it is safe to use hydromorphone in renal insufficiency.
Methods:
In this study we sought to determine the prevalence of neuroexcitation in patients with renal insufficiency who were given hydromorphone, as measured by the glomerular filtration rate (GFR), and to investigate factors associated with increased risk of neuroexcitation in this patient group. For the 12- month period from June 2007 through June 2008, charts of inpatient hospice patients that showed a glomerular filtration rate of <60 (mL/min/1.73 m2) and hydromorphone administration for pain control via continuous infusion were reviewed for the occurrence of neuroexcitatory effects, including tremor, myoclonus, agitation, cognitive dysfunction, and seizures.
Results:
Overall prevalence of neuroexcitatory effects were: tremor 11 (20%), myoclonus 11 (20%), agitation 26 (48%), and cognitive dysfunction 21 (39%). No seizures were observed. No neuroexcitatory effects were observed for the lowest quartile of dose or duration of hydromorphone. There was a strong and graded increase in neuroexcitatory effects with increasing quartile of dose or duration of hydromorphone for agitation (dose, p<0.0001; duration, p<0.0001) and cognitive dysfunction (dose, p<0.0002; duration, p<0.002). Consistent but weaker trends were observed for tremor and myoclonus.
Conclusion:
Parenteral hydromorphone has few neuroexcitatory symptoms until H3G accumulates past a neurotoxic threshold, such as might occur with increasing dose or duration, which, when exceeded, causes neuroexcitatory symptoms to manifest.
Introduction
Babul et al. 4 hypothesized that H3G, based on its structural similarity to morphine-3-glucuronide and enhanced water solubility, could be expected to accumulate in patients with chronic kidney disease(CKD) and, in one patient with CKD, demonstrated H3G levels 4 times as high as in patients with normal renal function. Of note, this patient did not exhibit any neuroexcitatory symptoms. Contrary to the experience of Babul and colleagues, multiple case reports have hypothesized that H3G accumulation in patients with renal insufficiency may have contributed to the neuroexcitation and cognitive impairment that was observed.5–9 Another study, by Lee and coworkers, 10 did not suggest problems with neurotoxicity when using hydromorphone in patients with CKD. In that study, oral, sustained- release hydromorphone was used in the setting of CKD for opioid rotation, with improvement of opioid-related adverse effects. Subjects were described as having end-stage renal disease, but inconsistency between blood urea nitrogen and creatinine levels raise questions concerning the patients' renal function. Another shortcoming of that study was use of creatinine as a marker for renal function, which is considered a poor marker for such function, especially in patients with reduced muscle mass, often seen in cachectic patients. A recent study by Davison and Mayo 11 on patients on dialysis who received chronic hydromorphone therapy found substantial accumulation of H3G on nondialysis days. There was an association between H3G accumulation and decreased time to maximal analgesia on nondialysis days suggesting an algesic effect of H3G accumulation. Generally, no untoward toxicity occurred, except the authors suggested that increased levels of H3G were associated with increased sensations, described as lancinating and tingling with elevated pain scores before dialysis. The authors suggested that hydromorphone was safe to use during dialysis, but that it might be problematic in those who are not having H3G removed.
One retrospective study reported that neuroexcitatory symptoms, such as myoclonus, agitation, and seizures, were independently associated with the dose of hydromorphone and the number of days on treatment. 12 The authors concluded that hospice patients receiving continuous infusion of hydromorphone for more than 15 days and with doses larger than 20 mg/hour may be at an increased risk for these neuroexcitatory symptoms because of their natural decline in renal function.
Because hydromorphone is an effective and useful analgesic for moderate to severe pain, there is a need to further consider the association between use of hydromorphone and the occurrence of neuroexcitatory effects. Determining the conditions under which neuroexcitation might occur in patients given hydromorphone is important, as neuroexcitation can worsen symptoms and adversely affect quality of life. The primary aim of this study was to observe if hydromorphone dose and/or duration was associated with neuroexcitatory effects in patients with CKD renal insufficiency as estimated by glomerular filtration rate (GFR), a far more accurate measure of renal function.
Methods
Study design and setting
A retrospective analysis was conducted of patients with renal dysfunction who received continuous infusion hydromorphone. Charts of patients who were treated either at one of Hospice of the Valley's inpatient palliative care units or at home during a 12-month period from June 2007 through June 2008 were evaluated. Charts were reviewed at all 4 of Hospice of the Valley's offices, which together serve all of Maricopa County, Arizona.
Study subjects
Inclusion criteria were age of at least 18 years, abnormal renal function as defined by GFR, and receipt of continuous parenteral infusion of hydromorphone. Charts of patients who fulfilled these criteria were reviewed and medical and nursing records were studied. Records prior to hospice admission were reviewed to obtain baseline laboratory data; relevant demographic and clinical data including age, sex, race/ethnicity, and weight were also recorded. GFR was calculated for patients via the Cockcroft-Gault equation. 13 Those patients with stage 3 to stage 5 kidney disease (GFR below 60) were considered to have CKD 13 and were included in the study. Patients below this cutoff are classified by the National Kidney Foundation as having at least moderate kidney disease with a loss of at least half of their nephrons. 13 Neuroexcitatory effects were recorded individually and included tremor, myoclonus, agitation, cognitive dysfunction, and seizures. Hospice diagnosis, maximum continuous dose of hydromorphone, duration of use, and method of administration to each patient were recorded.
Data collection and analysis
This study was approved by the Institutional Review Board at Arizona State University and was also approved by the leadership at Hospice of the Valley. Data were collected from charts by one investigator (G.P.)); for the purpose of this research, individual patients were assigned a code that was not related in any way to any of their personal information. The primary outcome measure was whether the patient with CKD had neuroexcitatory effects from hydromorphone. These neuroexcitatory effects included tremor, myoclonus, agitation, cognitive dysfunction, and seizures. Myoclonus was documented as present if twitching, jerking, or myoclonic movements were reported.
The distribution of values for demographic and clinical characteristics of patients was examined. To achieve normality, values of creatinine were transformed to logarithms before analysis. Demographic and clinical characteristics were compared between patients with and without neuroexcitatory effects and between those above and below the median for selected variables using the χ2 test, Fisher's exact test, or independent samples t tests, as appropriate. Trends for neuroexcitatory effects across quartiles of predictor variables were assessed by using the Fisher's exact test. Logistic regression was used to evaluate the association between dose and duration of hydromorphone neuroexcitatory effects independent of each other and of other potential confounding variables. All data analyses were performed with SAS version 9.0 (SAS Institute Inc., Carey, NC). A p value<0.05 was considered significant.
Results
Fifty-four patient charts were identified as meeting the inclusion criteria during the 12-month period of June 2007 through June 2008. Table 1 presents characteristics of the study population. The average age of the study population was 68.5 years, the sample was evenly split by gender (males: 48%), and most of the patients were Caucasian. Among this sample, 11 patients (20%) experienced tremor, 11 patients (20%) experienced myoclonus, 26 patients (48%) experienced agitation, and 21 patients (39%) experienced cognitive dysfunction. No patients experienced a seizure.
C, Caucasian; AA, African America; O, Other; GFR, glomerular filtration rate; HM, hydromorphone; IV, intravenous; SQ, subcutaneous.
Table 2 compares demographic and clinical characteristics of patients who experienced individual neuroexcitatory effects with those who did not experience such effects. These data suggest that neuroexcitatory effects with the exception of “cognitive dysfunction” did not increase with worsening renal function. The data show that dose and duration of hydromorphone were greater for those who experienced neuroexcitatory effects including cognitive dysfunction (Table 2).
GFR, glomerular filtration rate; HM, hydromorphone.
Table 3 presents characteristics and incidence of neuroexcitatory effects in patients stratified at the median for factors with potential to influence risk of neuroexcitatory effects, including dose and duration of hydromorphone, weight, GFR, and creatinine. As shown, prevalence of neuroexcitatory symptoms was higher for those receiving doses of hydromorphone above the median or for longer than the median duration. To further explore the relationship between dose and duration of hydromorphone and neuroexcitatory effects, we considered the prevalence of such effects across increasing quartiles of dose and duration of hydromorphone (Figs. 1 and 2). As shown, neuroexcitatory effects were absent in those patients who received doses of hydromorphone in the lowest quartile (Fig. 1) or were in the lowest quartile for duration of hydromorphone (Fig. 2).
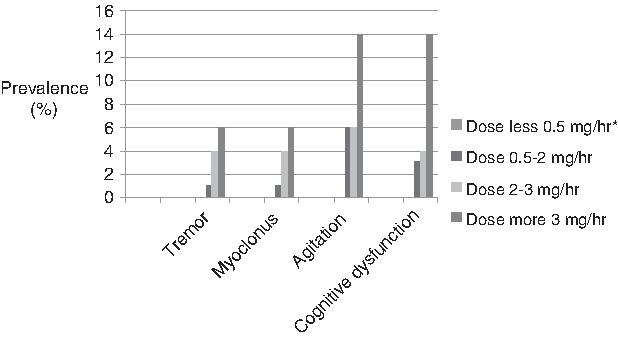
Incidence of neuroexcitatory effects according to increasing dose of hydromorphone. P values for trends across quartiles of dose: agitation: <0.0001; cognitive dysfunction: <0.0002. *There were no symptoms for patients receiving doses of <0.5 mg/hour.

Incidence of neuroexcitatory effects according to increasing duration of hydromorphone. P values for trends across quartiles of duration: agitation: <0.0001; cognitive dysfunction: <0.002. *There were no symptoms for patients with duration of treatment <2 days.
GFR, glomerular filtration rate.
Table 2 indicates that compared with duration of hydromorphone of 3 days or more, those who received infusion for less than 3 days were older (mean 74.7 versus 64.3 years, p<0.05) and had a different distribution of gender (63% versus 27% male, p=0.01). Because of those differences, it is possible that the relationship between dose and neuroexcitatory effects may be confounded by GFR, whereas the relationship between duration of hydromorphone and neuroexcitatory effects may be confounded by age and gender. Patients who received infusion for less than 3 days also had lower GFR (mean 37.8 versus 44.1, p=0.079) and lower dose (mean 1.7 versuss 9.8 mg/hour, p<0.04) compared with patients with duration of 3 days or more.
Compared with duration of hydromorphone of 3 days or more, those who received infusion for less than 3 days were older (mean 74.7 versuss 64.3 years, p<0.05) and had a different distribution of gender (63% versus 27% male, p=0.01). Patients who received infusion for less than 3 days also had lower GFR (mean 37.8 versus 44.1, p=0.079) and lower dose (mean 1.7 versus 9.8 mg/hour, p<0.04) compared with patients with duration of 3 days or more. To consider the relationship between duration of hydromorphone and neuroexcitatory effects independent of dose and these possible confounding variables, we performed logistic regression adjusting for potential confounders. After adjustment for GFR, gender, age, and dose, duration of hydromorphone (p<0.03) remained significantly associated with cognitive dysfunction and agitation (p<0.01). However, in these models, dose was no longer significantly associated with neuroexcitatory effects.
Discussion
Although this study was retrospective, we were able to show that adverse symptoms tend to occur with greater frequency in patients with renal insufficiency getting longer infusions and higher doses of hydromorphone. Importantly, no neuroexcitatory symptoms were observed for the lowest quartiles for dose (<0.5 mg/hour) and duration (<2 days). Thwaites and coworkers were first to suggest that a dose threshold exists for neuroexcitatory phenomena and the duration of continuous infusion therapy might also be associated with neurotoxicity. 12 Their study, which was also conducted in hospice patients, did not measure renal function. In this study, gradations of kidney dysfunction were measured and patients were stratified according to severity of renal function. Adverse events were interpreted according to these gradations. Our results show that it was dose and duration of hydromorphone infusion that played a greater role in the genesis of neuroexcitatory adverse effects. Adverse effects that were targeted were those specifically associated with opioid neurotoxicity such as cognitive dysfunction, agitation, and myoclonus. These symptoms are especially disturbing to patients and families. 13 There were several limitations of the study. We did not use the newer methods for measurement of renal function such as the chronic kidney disease epidemiology collaboration (CKD-EPI) method. Although available, this method may lose accuracy in the older patient population and at higher GFRs. 14 We also did not measure the impact of these neuroexcitatory adverse effects on families. We likewise did not focus on the analgesic response of giving hydromorphone in the setting of renal insufficiency. It is well known that opioid metabolites can decrease opioid responsiveness and this would have been a good opportunity to further clarify this relationship. 15
Conclusion
Hospice patients receiving parenteral hydromorphone by continuous infusion in the setting of renal insufficiency are susceptible to neuroexceitatory phenomena, and based on this study, we conclude that hydromorphone neuroexcitation occurs at an apparent threshold of dose at 0.5 mg/hour and durations of continuous infusion greater than 2 days. There are fewer occurrences of neuroexcitatory phenomena when patients with renal failure receive hydromorphone at a shorter duration and lower doses. We would recommend that when patients with renal insufficiency are on high-dose hydromorphone infusion or a regular dose of hydromorphone infusion for a prolonged period of time, these patients be vigilantly monitored for adverse effects.
Footnotes
Author Disclosure Statement
No competing financial interests exist.