
Abstract
Abstract
Palliative radiation therapy has been widely used for treatment of pain from metastatic bone disease. However, reirradiation is required in approximately 20% of patients initially treated with single fraction conventional palliative radiotherapy. There is a paucity of literature as to toxicities associated with reirradiation, and a lack of knowledge overall as to the cumulative dose limits for the organs at risk. We describe an uncommon late grade 4 adverse event of large bowel colitis in a patient initially radiated with 8 Gy in a single fraction, and reirradiated to the same area 3 months later with 20 Gy in 5 fractions due to pain progression.
Introduction
Case Presentation
This 56-year-old female with metastatic breast cancer was seen in consultation to consider palliative radiotherapy to a painful left hip bone metastasis. She was first diagnosed with breast cancer in 1994, and her primary disease was treated with a lumpectomy and axillary lymph node dissection (ALND) followed by adjuvant chemotherapy and breast radiation therapy. Five years later, she developed a contralateral breast cancer and was treated with mastectomy, ALND, and adjuvant systemic treatment. No adjuvant radiation was given. Eight years later she presented with left-sided chest pain, and an x-ray showed bone abnormalities that were consistent with bone metastases. She was subsequently treated with several courses of systemic therapy and palliative conventional radiation therapy to various sites of painful bone metastases with no unusual toxicities reported.
The radiation courses of interest were delivered first to the left hip in June 2009 where part of the large bowel (including the sigmoid colon) was included in the treatment field as shown in Figure 1. A dose of 8 Gy in a single fraction was delivered using a standard beam arrangement of an anterior-posterior parallel opposed pair and a beam energy of 18 MV photons. The treatment plan was reviewed, including slice-by-slice evaluation of the dose to the tissues, and no unusual deposition of high doses was observed. Following radiation, no acute or subacute toxicities were noted, and the patient's pain did improve within the subsequent few weeks. Three months later, she experienced progression of her left hip pain and investigations confirmed radiographic local disease progression. It was then decided to reirradiate the left hip with a similar technique using, however, a more limited field centered on the left hip and fractionating the reirradiation course. She was treated with 20 Gy in 5 fractions (Figure 2). Despite the smaller re-irradiation field dimensions, a portion of the large bowel (including the sigmoid colon) that had been previously radiated was included in the reirradiation portal, in order to treat the hip effectively (Figure 2). The treatment plan was again reviewed and no unusual high doses were observed in the tissues. Clinically, the patient tolerated the retreatment well with no acute or subacute toxicities, and the pain did improve.
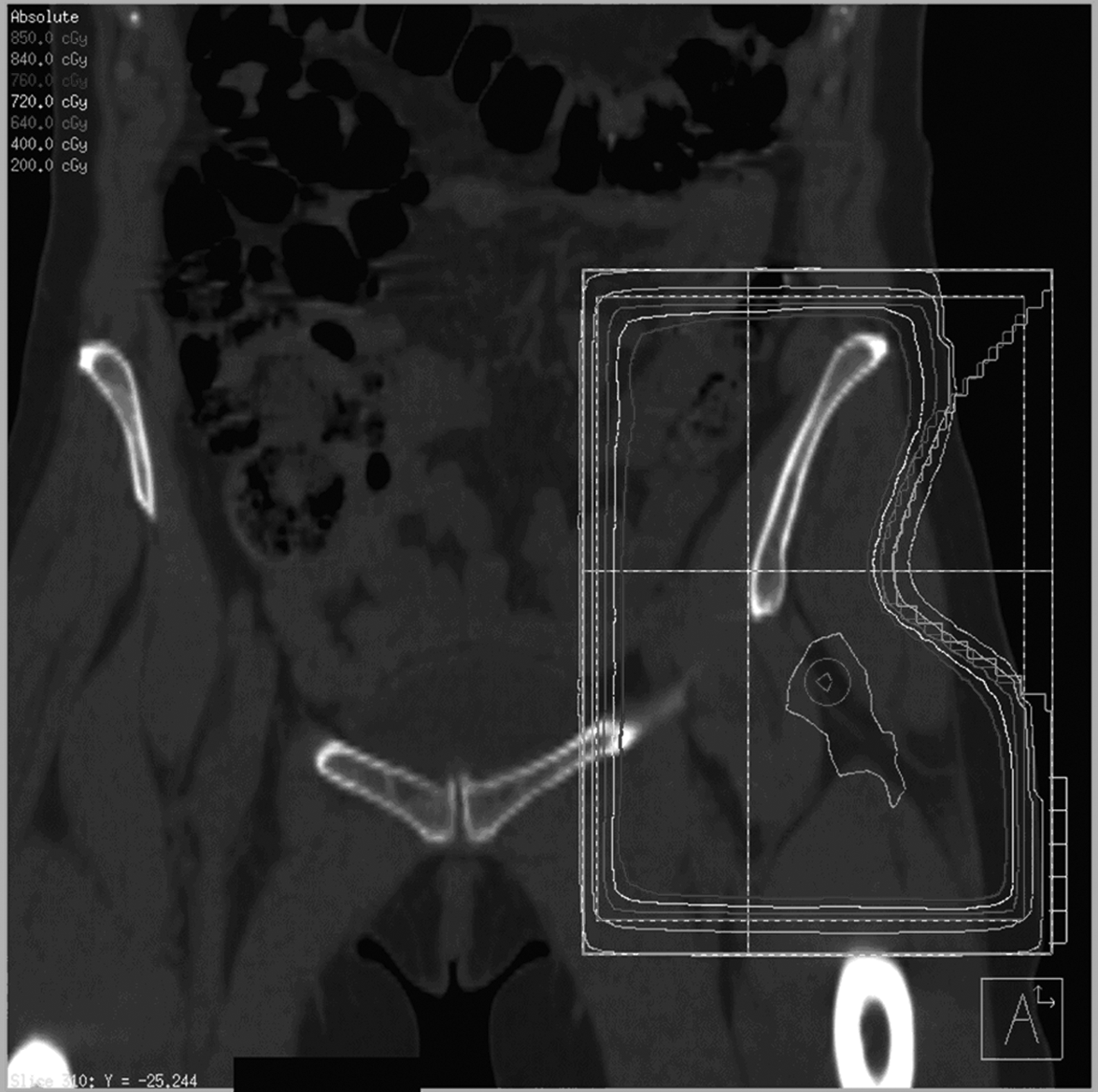
A coronal view of the radiation treatment plan for the 8 Gy in 1 fraction treatment using an anterior-posterior parallel pair technique and 18 MV photons. Representative isodose lines are shown.

A coronal view of the radiation treatment plan for the 20 Gy in 5 fraction treatment using a more limited an anterior-posterior parallel pair technique and again 18 MV photons. Representative isodose lines are shown.
One year following her reirradiation, she presented to the emergency room with a one-month history of hematochezia and a drop in her hemoglobin to 70 g/L (normal range, 120–160 g/L). She was assessed by the gastroenterology service and underwent an abdominal computed tomography (CT) scan. Circumferential wall thickening of the sigmoid colon in its mid portion was observed. The patient underwent a gastroscopy and colonoscopy. Gastroscopy was normal; however, the colonoscopy showed segmental areas of colitis. The area of pathology was documented to arise 15 cm from the anal verge and extended to the descending sigmoid junction. There was mention of friable mucosa and abnormal vascularization (telangiectasias) suggestive of RIC (Figure 3), and the biopsies performed ruled out inflammatory bowel disease. Treatment was initiated with 5-aminosalicylic acid, iron supplement, and transfusions. Multiple attempts to coagulate the bleeding mucosa were attempted with no benefit, and the patient continues to undergo routine transfusions now 5 months following diagnosis as she refuses surgical intervention.
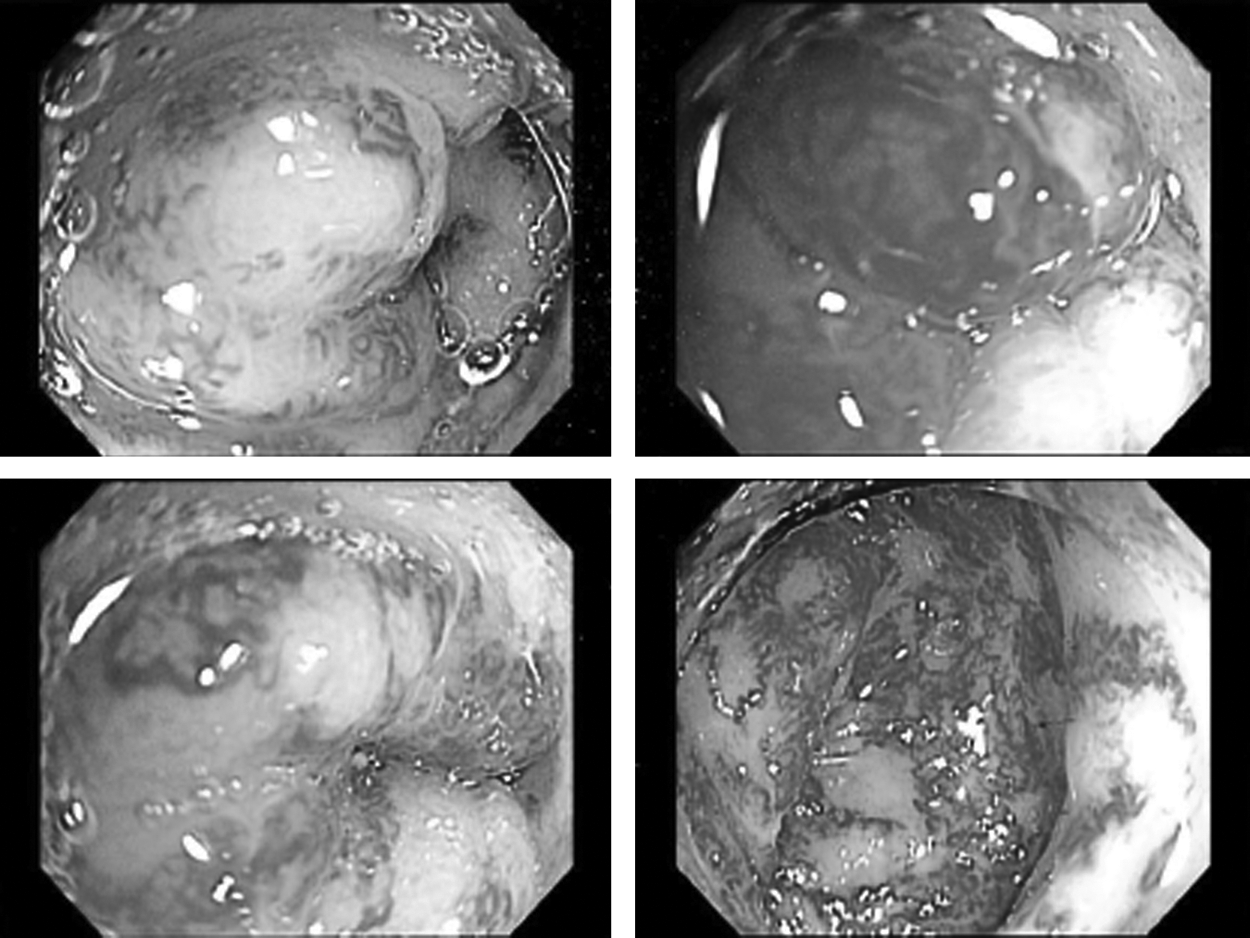
Colonoscopy pictures showing telangiectasias and friable mucosa within the sigmoid colon suggestive of RIC.
Discussion
We report on a patient who unexpectedly developed grade 4 RIC as a late toxicity 12 months after receiving standard conventional palliative radiation treatments to a hip metastasis. The patient was first treated with 8 Gy in a single fraction and retreated 3 months later with 20 Gy in 5 fractions. Upon review of the treatment plans, we could not explain the observed toxicity by unexpected high doses within the bowel and clinically no unusual acute or subacute toxicities were observed. The only factor that may have contributed to a higher risk of late toxicity was the short time interval between courses (3 months); however, the radiation doses were still generally considered to be within large bowel tolerance.
RIC is defined as an inflammation of the colon after exposure to radiation therapy. It is generally a self-limiting toxicity in which patients are asymptomatic and do not require significant medical intervention. When treatment is necessary, it is usually limited to coagulation of the affected bleeding mucosa or supportive treatments. RIC is usually associated with significantly higher doses of radiation in the radical curative setting as opposed to low-dose conventional palliative radiotherapy schedules. 6 This is a first report of this toxicity in the context of palliative reirradiation.1–4,7 Therefore, radiation oncologists should be aware that this severe and debilitating toxicity is possible with conventional reirradiation, and that treatment planning should attempt to avoid reirradiating bowel within the treatment field.
Conclusion
The purpose of this case report is to highlight the potential for grade 4 RIC following conventional palliative reirradiation. Although rare, radiation oncologists should consider this potential toxicity in their radiation treatment planning and advise patients of the risk as an unlikely but possible serious late toxicity.
Footnotes
Acknowledgments
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
L.M., L.M-C., A.S. and D.L. have been involved in drafting the manuscript, revising it critically for important intellectual content and have given final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.