
Abstract
Abstract
Major efforts have been pursued to improve palliative care education for physicians at all levels of their training. Such changes include the incorporation of palliative care curriculum and guidelines, an established process for competency-based evaluation and certification, faculty development, innovative educational experiences, the improvement of textbooks, and the establishment of accredited palliative medicine fellowships. Hospice and palliative medicine (HPM) has been clearly defined as a subspecialty and a crucial area of medical education. As innovative curricular approaches have become available to educate medical and other interprofessional trainees, this article aims to describe different models and methods applied in curriculum evaluation, tailoring such approaches to the field of palliative medicine. A stepwise process of curriculum development and evaluation is described, focusing on available curriculum evaluation competency-based tools for each level of learners. As HPM evolves and its educational programs grow, curriculum evaluation will provides invaluable feedback to institutions and programs in many ways.
Background
Major efforts have been pursued to improve palliative care education for physicians at all levels of their education. Such changes include the incorporation of palliative care curriculum and guidelines, an established process for evaluation/certification/licensure, faculty development, new venues for education, the improvement of textbooks, and the establishment of accredited palliative medicine fellowships.3–5
The steadily increasing implementation of HPM curriculum in medical schools has been shown to improve medical students' preparedness and knowledge. 6 Studies have shown that medical school graduates exposed to 20 hours of coursework on palliative and EOL care reported learning palliative care basic objectives and symptom management and assessment. 7 As expected, bedside teaching and clinical encounters positively contribute to communication skills training in palliative care. 8 The increase in formal HPM curriculum in medical schools is encouraging; however, the negative perceptions from the “hidden curriculum” (that inferred from behaviors and implicit in medical culture) may impair learning. 4 Because of its interprofessional nature, HPM education has the potential of educating medical learners on the advantages of interdisciplinary and transdisciplinary teams when caring for chronically and terminally ill patients. 9
Most recently, medical schools began to provide required EOL instruction for accreditation by the Association of American Medical Colleges (AAMC) and the Liaison Committee on Medical Education (LCME), even at early stages of medical education (pre-clerkship).10,11 These skills and competencies are to be integrated and evaluated into the medical school curriculum.
At the postgraduate level, primary care residency programs such as internal medicine have incorporated HPM into their curriculum, as mandated by their regulatory organizations several years ago. 12 Weissman and Block reviewed the EOL requirements of postgraduate training programs and found that the programs with most comprehensive EOL content were internal medicine, geriatrics, and neurology; most surgical specialties contained no EOL requirement except ethics. 13 Palliative care requirements have been identified as important geriatric competency elements for family medicine and internal medicine residents and geriatric fellows. 14 Surgical residency programs have most recently included HPM curricular elements into their required topics. 15
HPM was established as a new subspecialty by the American Board of Medical Specialties (ABMS) in 2006. 16 Several medical specialties boards have core competency requirements in HPM and want their diplomates to have access to subspecialty certification in the HPM field. Recognizing a shared interest in this subspecialty, 10 participating ABMS boards now co-sponsor the subspecialty (anesthesiology, emergency medicine, family medicine, internal medicine, obstetrics and gynecology, pediatrics, physical medicine and rehabilitation, psychiatry and neurology, radiology, and surgery). Simultaneously, the Accreditation Council for Graduate Medical Education (ACGME) began accrediting training programs preparing physicians for subspecialty in the HPM field. 17 As of January 2010, there were 74 active programs offering 181 fellowship positions. A total of 73 programs have been accredited by the ACGME and 3 programs have been accredited by the American Osteopathic Association. 18 The American Academy of Hospice and Palliative Medicine (AAHPM) partnered with ACGME to develop HPM core competencies for fellows. Such competencies have been disseminated to standardize curriculum development and evaluation of HPM fellows as this subspecialty. 19
Pediatric palliative care is also an emerging field. Pediatric residents who have benefited from pediatric palliative care teaching stated that they have learned important skills in pediatric EOL care and that they have enhanced confidence in their ability to care for dying patients and their families. 20 Additionally, there have been initiatives such as the Initiative for Pediatric Palliative Care (IPPC), an education and a quality improvement effort aimed at enhancing culturally respectful, family-centered care of children living with life-threatening conditions. This initiative aims to educate interprofessional learners who interact with very ill and dying children. 21 A group of pediatric palliative care leaders is working on the Pediatric Hospice and Palliative Medicine Competencies Project with the aim of creating a resource for pediatrics specific HPM competencies. 22
In summary, HPM education continues to grow impressively throughout all levels of medical education. As innovative curricular approaches have become available to educate our trainees, this article aims to describe different models and methods applied in curriculum evaluation, tailoring such approaches to our field. We will describe generalities of how to evaluate curriculum, focusing on aspects related to the learner's assessment in palliative care.
General Concept: What Is Curriculum As It Applies to Medical Education?
Harden defines curriculum as a sophisticated blend of educational strategies, course content, learning outcomes, educational experiences, assessment, the educational environment, and the individual student's learning style, personal timetable, and program of work. 23 Furthermore, Harden has introduced the innovative concept of curriculum mapping. Curriculum mapping is the process that describes what is taught (the content, the areas of expertise addressed, and the learning outcomes), how it is taught (the learning resources, the learning opportunities), when it is taught (the timetable, the curriculum sequence), and the measures used to determine whether the student has achieved the expected learning outcomes (assessment or evaluation).
The process of curriculum development and delivery in medical education requires higher levels of organizational skills. First, medical curriculum must have clear learning objectives and criteria. 24 Key players such as trainees and faculty must be previously aware of the objectives. Once taught, the trainees' evaluation must be based on what was taught and must be clearly documented. Lastly, trainees should receive feedback in a timely manner and a process should be in place to address the individual needs of trainees. 25
General Concept: Defining Curriculum Evaluation
The ultimate evaluation of a medical curriculum seeks evidence for developing practice, setting policy, planning standards for education, and making educational decisions. 26 Effective curriculum evaluation begins before the educational experience starts. Medical educators should determine the attitudes, knowledge, and skills that are necessary to bring about the desired behavior. The ultimate challenge is to design/implement medical curriculum and pedagogical strategies in a way that leads medical learners to increase their knowledge and apply it as reflected in clinical performance that enhances the quality of patient care, an outcome at the result level of Kirkpatrick's evaluation model as illustrated in Figure 1.27,28 Fig. 1 Kirkpatrick described four levels of evaluation in which the complexity of the behavioral change increases as evaluation strategies ascend to each higher level. 27
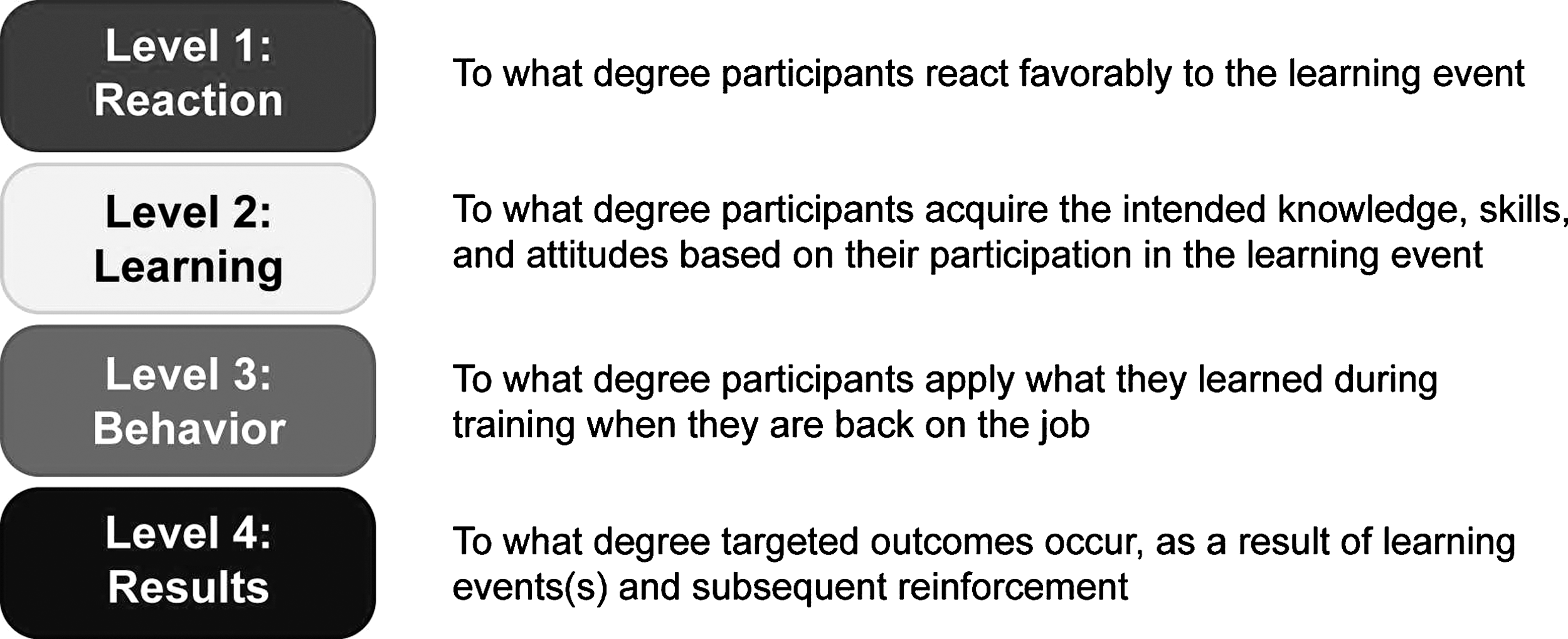
Kirkpatrick Four Levels™ Evaluation Model. ©2010 Kirkpatrick Partners, used by permission. All rights reserved.
The Kirpatrick model's four levels include: (1) learner's reaction to the educational experience or curricular component; (2) learning that refers to changes in attitudes, knowledge, and skills once the curricular experience is delivered; (3) behavior or changes in practice and the application of learning to practice; and (4) results to trigger change at the level of the learner and the organization. 27 When this model is adapted to health care education, additional factors are considered such as change in organizational practice as it refers to clinical skills and benefits to both learners and their patients. 29
Specific Concept: Common Types of Learner-Focused Curriculum Evaluation Used in Hospice and Palliative Medicine
In 1998, the ACGME and the ABMS initiated the Outcome Project to ensure and improve the quality of graduate medical education for all specialties. 30 The project envisions an accreditation process that assesses a program's actual accomplishments through educational outcomes or competencies, rather than just their potential to educate. Competencies are defined as groups of skills, behaviors, or knowledge that are identified as performance standards for a particular job22,31 In medical practice, competencies are written as real-life skills represented in six areas of skill and knowledge required for effective professional medical practice (patient care, medical knowledge, practice-based learning and improvement, interpersonal and communications skills, professionalism, and systems-based practice). Following this competency-based model, HPM education experts published competencies to evaluate fellows during training. 19 Once competencies are defined, different and multiple methods can be matched to evaluate such competencies and multiple methods for each competency, understanding that direct observation in clinical settings is the typical method of evaluation. Observation is a way of gathering data by watching behavior or events, or by noting physical characteristics in their natural setting. 32
Next, we will exemplify how the Kirkpatrick model and the ACGME competencies can be applied to evaluate the effect of an HPM educational activity in family meetings:
Level 1 Reaction: After a training session on family meetings participants are asked if they like the training. (ACGME competencies: professionalism and practice-based learning)
Level 2 Learning: Participants are evaluated in a formative observed structured clinical encounter (OSCE) setting to assess the degree to which participants acquired the knowledge and skills to effectively lead a family meeting (ACGME competencies: medical knowledge, interpersonal and communication skills).
Level 3 Behavior: Observing participants apply what they learned while leading a real family meeting and goals-of-care discussion, followed by learner reflection on performance and reinforcement of communication principles by the supervising faculty (ACGME competencies: practice-based learning, patient and family care, interpersonal and communication skills).
Level 4 Results: Evaluating the results as reflected in the satisfaction of the patient/family member with the leaner's work after a family conference. At a more macro level there are opportunities to incorporate a quality improvement project to track how behavior changed pre- and posteducational activity in family meetings as reflected in the documentation of family meetings and in patient/family satisfaction surveys (ACGME competencies: systems-based practice, patient and family care, interpersonal and communication skills).
Medical students
Primary palliative care refers to the basic skills and competencies required of all physicians and other health care professionals. 33 The LCME recognized the need for EOL education among medical students. Since the incorporation of primary palliative care principles into medical schools, several studies have shown multiple curriculum delivery methods when teaching palliative and EOL care to medical students. The ideal HPM curriculum for medical students has not been defined; however there is evidence in several studies that exposing students to clinical experiences during their clinical years leads to more significant learning in palliative care because learners get to practice under supervision the skills they learned (Kirkpatrick level 3).4,34 Common teaching methods included didactic sessions, assigned readings and case reviews, diverse forms of clinical experiences, and journaling to explore reactions. 6 Learner evaluation methods included different types of surveys, pre and post-tests, 35 360-degree evaluations, 36 and comprehensive knowledge testing. 37 Specifically for patient encounters, evaluation methods tested (1) Interviewing skills (standardized patients, 360-degree evaluations, OSCE, and checklists); (2) teamwork (checklists, global ratings, and 360-degree evaluations); (3) patient education and counseling (360-degree evaluations, OSCE, checklists, and patient evaluation), 15 and communication skills (unfolding cases). 38
However, one study found that 39% of students felt unprepared to address patient and family issues related to dying, and more than 40% of residents reported being unprepared to teach EOL courses to students. The report stated that less than 18% of students and residents had participated in a formal EOL curriculum. 39 There is a critical need for the establishment of standardized, required core competencies in palliative medicine and EOL care to ensure proficiency. Efforts to define such competencies have begun, particularly relating to care for elders. The AAMC in partnership with the John A. Hartford Foundation has established competencies in geriatric education, defined as minimum graduating medical student competencies needed to assure competent care to older patients by new interns. Within this set of competencies, palliative care learning outcomes have specifically been described: pain and symptom management; psychological, social, and spiritual needs of patients with advanced illness and their family members; and the importance of interdisciplinary care. 40
Residents
The ACGME Outcome Project is a long-term initiative to emphasize educational outcomes in the accreditation of residency education programs. ACGME identified six general competencies for residents. Such competencies allow programs to determine how physicians are adequately prepared to practice medicine in the changing health care delivery system. 41 Moreover, the Outcome Project aims to develop tools for programs to use as part of an overall evaluation system. ACGME and the ABMS delivered the Toolbox of assessment methods, which includes descriptions and examples of instruments recommended for use by programs as they assess the outcomes of their educational efforts. The Assessment Toolbox proposes several evaluation methods, including chart reviews, patient assessments, 360-degree evaluations, OSCEs, checklists, simulation, and standard examination, among others. 42
EOL training for residents has been recommended by regulatory organizations such as the ACGME and the Residency Review Committee (RRC). 3 Some studies have described successful educational experiences tailored to residents with the potential of meeting objectives in virtually all of the ACGME core competencies including patient care, medical knowledge, communication, lifelong learning, systems-based practice, ethics, and professionalism.36,43 At this time the ACGME competencies are not specific to HPM, although there is a taskforce working on developing HPM competencies for residents.
Fellows
As a recognized subspecialty, HPM has quickly and efficiently developed pathways for board certification, fellowship standards, and fellowship accreditation to comply with regulatory entities such as the ACGME and the ABMS and to adapt to their competency framework. In 2007, Morrison and colleagues 19 published HPM core competencies to evaluate progress as fellows advance through novice and advanced beginner levels, and move toward expert levels of competency. 44 The HPM competencies are the result of a collaborative effort among field experts, who based their work on the ACGME competency domains. Once developed, the HPM competencies document was widely distributed for feedback and comments. The final competencies document includes patient and family care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice. 19 Subsequently, competency-based assessment methods were carefully selected for each ACGME domain, and compiled in the HPM Toolkit of assessment methods. 45 A summary of HPM competency-based assessment methods is shown in Table 1. The development of competencies and assessment methods for HPM fellowships has been crucial in the rapid advancement of this field.
Toolkit of Assessment Methods from www.aahpm.org/fellowship/default/competencies.html
Note: These assessment toolkit instruments have for the most part not been psychometrically assessed for validity or reliability.
General Concept: Interprofessional Education and Curriculum Evaluation
The delivery of palliative care can be best accomplished in a collaborative environment integrating a bio-psychosocial-spiritual model of interprofessional team members from different fields such as medical, nursing, and psychology. HPM training of interprofessional learners is a natural way to begin collaboration from the early stages of their careers.9,46 Interprofessional education occurs during those occasions when members (or students) of two or more professions learn with, from, and about one another to improve collaboration and the quality of care. 47
Interprofessional education aims to educate other colleagues and patients about one's own professional role, responsibilities, and the general scope of practice. It is a true example of collaboration among health professions to establish common goals, provide care for patients and their caregivers, and facilitate shared decision making. 48 Interprofessional education has been widely used in different settings.
Most of the evaluation methods used focus on measuring reactions to the innovative concept of interprofessional education, 47 change in attitudes and qualitative knowledge, and skills improvement. 49 The use of interprofessional education has showed positive outcomes in service delivery or patient care 50 and the development of quality improvement initiatives. 51
Interprofessional education in palliative care is advancing; however, those advances are outside the scope of this article.
A systematic review of interprofessional education curricula found that Kirkpatrick's model was useful 27 when analyzing evaluation outcomes. 47 Table 2 summarizes levels and outcomes of interprofessional curriculum evaluation, with a specific example related to HPM education (learning to conduct a family conference to establish goals of care).
Discussion
Medical education is perpetually reconfiguring itself in response to the needs of constantly changing scientific knowledge, technology, and health care delivery systems. 52 There is a crucial need to redesign medical training. Nonetheless, curricular reform is a very complicated process. 53 Typically, leaders in medical education have chosen to emphasize scientific knowledge over clinical judgment, practical skills, and the development of cardinal virtues such as compassion and integrity. 54 Palliative care aims to improve the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering. 2 As the paths to reforming medical education evolve, 52 more emphasis should be placed on compassionate care, symptom relief, family involvement, and working in interprofessional teams, which are the core principles of hospice and palliative medicine.
An educationally rich palliative care curriculum should include didactic and clinical experiences where learners observe the role-modeling of competent and compassionate palliative care and have supervised experiential opportunities.5,34 Improvements within individual schools/residencies still largely rely on the presence of an effective palliative medicine champion who combines commitment and vision, leadership skills, education skills, and clinical skills. 55 To provide meaningful clinical experiences for learners and to mainstream palliative medicine it is crucial to provide faculty development in primary palliative care skills to non-HPM faculty to ensure care for the growing population of complex chronically and seriously ill people.34,56
As HPM evolves and its educational programs grow, learner-based curricular evaluation provides invaluable feedback to institutions and programs in many ways. First, it is expected that the field will experience drastic curricular changes in a dynamic way. Such dynamic curricular changes have already begun with the establishment of HPM as a subspecialty and the need to educate clinical learners at different levels of training. When evaluating HPM curricula, educators need to look at the “big picture” and map out the different teaching and evaluation activities against established competencies. Using available models of competencies and evaluation tools19,42,45 is most helpful and very time/cost-effective, avoiding “re-inventing the wheel.” Second, programs should also carefully consider their current strengths as their starting point in building and modifying curriculum, and should subsequently fill the gaps with new educational experiences rather than a total curricular reform.
The success of a program is measured by evaluating some of its outcomes such as learner competency. Such outcomes are greatly determined by the type of clinician educators who deliver the educational intervention. Preparing health care professionals for teaching is crucial to enhance teaching effectiveness. 57 Studies have shown that outstanding clinical teachers benefit from faculty development experiences to improve their skills, job satisfaction, and most importantly, the quality of the education they deliver, as evaluated by their students. Highly rated learning experiences included experiential learning, direct feedback, effective peer and colleague networking, and innovative educational methods within single interventions. 57 Lastly, all training programs must report to local and national regulatory entities. Previously described organizations such as the ACGME (residents/fellows) and the LCME (medical students) have sponsored specific competencies and tools to evaluate training outcomes. Programs are judged by their potential to educate when (1) they are compliant with program requirements; (2) they have established objectives and an organized curriculum; and on (3) have evaluation processes in place for learners, teachers, and the program itself. Additionally, all training programs must provide evidence of performance, objective accomplishment, and continuous improvement in their educational processes. 58
As the field of HPM continues to grow and the available HPM assessment tools are more widely used these tools could be tested for reliability and validity at the fellowship level. The challenge is how to foster organized interinstitutional collaboration to evaluate the tools. Secondary to the early integration of palliative care training focused on medical students and residents, there will be a need to evaluate the impact of such training as primary palliative care skills are developed among these learners.
Footnotes
Acknowledgments
The authors wish to thank Dr. Charles Von Gunten for his thoughtful review and Wendy Kirkpatrick for granting permission to use the Kirkpatrick Four Levels™ Evaluation Model.
Author Disclosure Statement
No competing financial interests exist.