
Abstract
Abstract
Objectives:
Informal caregivers of hospice patients experience multiple stressors that can negatively impact physical, psychological, and emotional health. The Caregiver Life Line (CaLL) study was a one-group, intervention-only feasibility study of a telephone cognitive-behavioral stress-management intervention consisting of 10 to 12 weekly telephone counseling calls designed specifically for informal caregivers of home-based hospice patients.
Methods:
Caregivers, who were recruited via seven participating hospices, were assessed at baseline, 3, and 6 months. Psychosocial measures included depression, perceived stress, benefit finding, social support, and quality of life (QoL). Process evaluation was also conducted at 6 months.
Results:
Of the 25 participants, 19 completed the 12-week intervention. The mean age was 60.3 years; 91% were female and 70% married. Forty-eight percent were caring for a spouse; 51% were caring for a parent or other family member. Participating caregivers and hospice staff reported high levels of satisfaction with the intervention. Although the small sample size and lack of a control group limit our ability to assess the efficacy of the intervention, psychosocial outcomes changed in the expected direction and participants reported high levels of self-efficacy regarding their ability to implement the adaptive coping skills. Interestingly, we observed a decrease in physical QoL across the three time points.
Conclusions:
This pilot study demonstrated that the CaLL intervention is feasible and acceptable to informal hospice caregivers. This report describes important lessons learned from the pilot study with the intention of informing future intervention studies with this population.
Introduction
In 2004, The National Institutes of Health “State-of-the-Science Conference Statement: Improving End-of-Life Care” included a recommendation for intervention trials focusing on family caregivers. 10 Two recent systematic reviews of interventions for caregivers of patients using palliative care services identified few high-quality intervention trials and concluded that there was a lack of evidence-based interventions for this population of caregivers.11,12 This study examined the feasibility of the Caregiver Life Line (CaLL) intervention for caregivers of home-based hospice patients to inform the design of a future randomized clinical trial (RCT) if CaLL was deemed feasible and acceptable to both caregivers and hospice staff.
The Caregiver Life Line telephone counseling intervention
Psychosocial interventions that integrate coping skills training, cognitive-behavioral strategies, and positive benefit finding have been shown to improve adaptation to stressful life events.13–15 Numerous studies have documented the effectiveness of telephone-administered interventions for alleviating depression and distress in various populations16–20 A telephone-delivered intervention was deemed particularly relevant to caregivers of home-based hospice patients given their reluctance to leave the home for long periods of time. We theorized that a telephone-based intervention aimed at improving coping skills and integrating a sense of meaning into caregiving activities would lead to increased utilization of adaptive coping strategies and decreased distress in a group of informal hospice caregivers.
The CaLL intervention consisted of 10 to 12 semi-structured counseling calls designed to complement existing hospice services. Telephone counseling sessions occurred throughout the caregiving experience, and continued independently of the timing of the death of the hospice patient. To ensure that we adequately tailored the intervention to meet the needs of hospice caregivers, we initially conducted targeted interviews and focus groups with former hospice caregivers and hospice staff to identify key content areas. 21 The manualized intervention was delivered by a Master's level counselor who received training in both the content of the intervention and the process of delivering the telephone intervention. Study fidelity and quality assurance were maintained through standardized oversight of intervention delivery. An overview of the CaLL session content area is included in Table 1.
Methods
This study employed a single-group, intervention-only research design with a specific focus on feasibility of intervention implementation and obtaining process evaluation data to refine the intervention pursuant to a future RCT. The study was approved by the Colorado Multiple Institute Review Board.
Caregivers were recruited from seven participating hospice programs that were both geographically and demographically diverse (see Table 2). Eligibility criteria included: 1) being a family caregiver of a hospice patient; 2) access to a telephone; 3) English speaking; and 4) no medical, psychological, or cognitive condition that would interfere with the ability to consent and/or participate in the program.
Hospice Partners: Hospice, Falls Church, VA; Denver Hospice, Denver, CO; Hospice of Michigan, Detroit, MI; Hospice of Montezuma, Cortez, CO; Hospice of St. John, Lakewood, CO; Rice Hospice, Willmar, MN; and San Diego Hospice, San Diego, CA.
The baseline and two follow-up assessments, which were conducted over the telephone, included the Center for Epidemiological Studies Depression Scale (CES-D), 22 Perceived Stress Scale (PSS) 23 quality of life (QoL) as measured by the Medical Outcome 36-Item Short-Form Health Survey (MOS SF-36), 24 perceived social support using the ENRICHD Social Support Instrument (ESSI), 25 and the Benefit Finding Scale (BFS). 26 Self-efficacy regarding the participants' ability to utilize the adaptive coping skills presented in the intervention 27 was assessed postintervention. Program evaluation data were collected at the time of the final assessment.
Data analysis included descriptive statistics to depict the participant characteristics and preliminary outcomes, including frequencies, means, standard deviations, 95% confidence intervals, percentages, and nonparametric correlations (i.e., τ). Due to the limited sample size and lack of statistical power, significance testing was not conducted. 28
Results
Recruitment and retention
We have limited information on the number of caregivers approached for the study because only three of the seven hospices maintained accurate records. Fig. 1 provides an overview of participant retention.
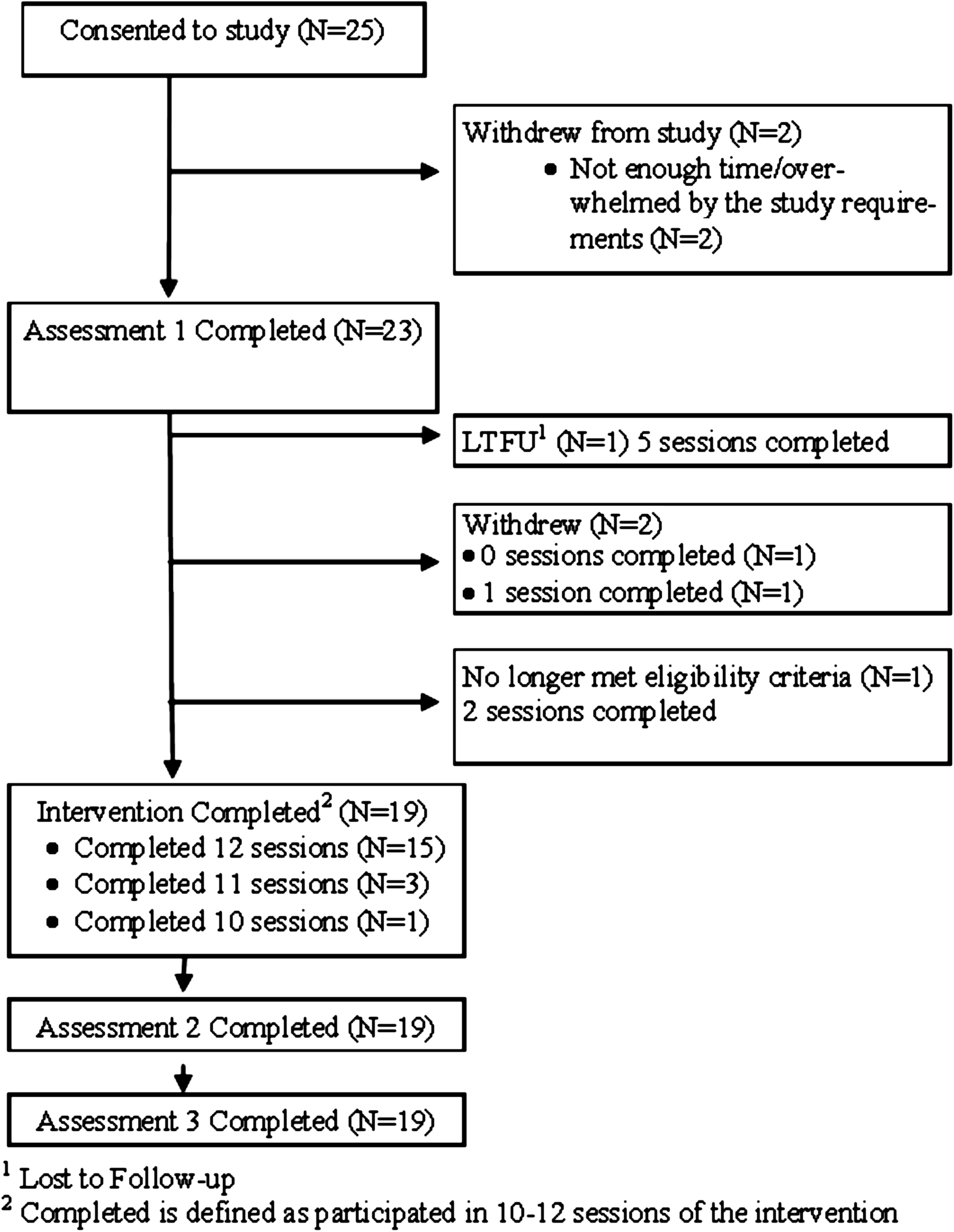
CaLL participation retention.
Of the six caregivers who did not complete the intervention, two had a different family relationship (sibling or grandchild) than the majority of the caregivers (spouse or child), two were sisters who were alternating caregiving duties for their parent, and two were of significantly advanced age (over 85). Table 2 describes caregiver demographics for all participants who completed the baseline assessment.
Acceptability
The process of conducting the intervention was viewed positively by the counselor and all of the participating hospice sites. Additionally, the delivery method, timing, and format of the CaLL intervention were acceptable to the participating caregivers (see Table 3).
Percentages are based on the 19 people who completed the postintervention assessment.
Preliminary psychosocial outcomes
Correlations among psychosocial measures were in the expected direction. Depression scores and perceived stress decreased over time, whereas social support, emotional/social QoL, and benefit finding increased from preintervention to postintervention. Physical QoL decreased across the three time points. Participants reported high levels of self-efficacy regarding their ability to utilize adaptive coping skills. (See Table 4)
Higher score represents poorer outcome.
Higher score represents better outcome.
Center for Epidemiological Studies Depression Scale (CES-D); Perceived Stress Scale (PSS); MOS SF-36; ENRICHD Social Support Instrument (ESSI); Benefit Finding Scale (BFS).
SD, standard deviation.
Discussion
The CaLL intervention was acceptable, feasible, and clinically relevant to our sample of informal caregivers of home-based hospice patients. With the help of our seven hospice partners, we were able to successfully recruit hospice caregivers across a geographically diverse area. The majority of participants were spouses or children of hospice patients; those who had a different caregiving relationship were less likely to complete the full intervention, suggesting that the intervention may be more relevant for close family members. The two oldest caregivers (both 88 years old) did not complete the intervention and future intervention studies should pay careful attention to the retention of older caregivers.
Although our research design and lack of statistical power restricted our ability to comment on the effectiveness of the intervention, encouraging trends were observed. Caregivers experienced a reduction in distress over the three time points. We also noted an increase in benefit finding and social support from baseline to the postintervention assessment. Physical QoL scores decreased across the three time points, which may represent the increased burden of caring for a dying loved one in one's home. Other caregiver interventions have reported limited success in improving overall QoL, although specific aspects of QoL may improve as a result of psychosocial intervention.12,29,30
Self-efficacy regarding one's ability to cope with the challenges of caregiving has been assessed in a number of studies.31–33 Postintervention ratings indicate that participants were highly confident that they could employ the skills and techniques presented during the intervention. Additionally, the postintervention interview data indicate that participants were satisfied with their CaLL intervention experience.
Special challenges and limitations
One of the major challenges in conducting intervention research among hospice caregivers is how to best handle variability related to the timing of the hospice patient's death. More than one third of our participants ceased their caregiving activities prior to completion of the intervention. This was not surprising given that the median hospice length of service in 2008 was 21 days. 34 Clinically, we were able to address this by including sessions that addressed grief and bereavement issues. This becomes more complicated when assessing psychosocial outcomes. We made the decision to base our assessments on intervention-related time points although one might argue that we could have timed our assessments to the patient's death. Future studies should carefully consider how to integrate the timing of death and/or the end of active caregiving into the study design.
Working with multiple hospices across the country allowed for increased diversity in our caregiver population and to determine the ease with which this intervention might be disseminated in the future. One drawback of utilizing distant recruitment sites was that we had limited control over how potential participants were identified and approached by various hospice staff. It was our impression that there was some selection bias regarding which caregivers would be “good” for the study, which may have influenced the results of the intervention.
Lack of a comparison control group makes it difficult to interpret the observed findings across the three time points. We might postulate that the improvement in distress and perceived stress that was observed in study caregivers is likely to be more than what we would expect in a usual care comparison group given the results of RCTs with caregiver populations.11,12
Conclusions
This CaLL pilot study demonstrated acceptability and feasibility of a telephone-based stress-management and coping-skills intervention for informal caregivers of home-based hospice patients. Participants reported high levels of satisfaction with the program and high levels of self-efficacy regarding their ability to utilize adaptive coping skills. Although our small, single-group design limited our ability to interpret our psychosocial outcomes, these preliminary findings suggest that the intervention may help to buffer some of the stressful aspects of caregiving. This feasibility study also documented challenges of conducting a trial across diverse hospices and among participants who are caring for loved ones with unpredictable life expectancies, informing design of a planned RCT.
Footnotes
Acknowledgments
This research was supported from a grant from the American Cancer Society (PEP-07-212-01-PEP1). The authors thank Jean Schleski and Jenny Vancura for their dedication and participation on this project.
Author Disclosure Statement
No competing financial interests exist.