
Abstract
Abstract
Objectives:
Little data are available on palliative home care for children. The objective of this study was to evaluate the effectiveness of a specialized pediatric palliative home care team (PPHCT) as experienced by parents and health care professionals (HCPs).
Methods:
Parents and HCPs involved in the care of terminally ill children who died and whom the PPHCT was in charge of were surveyed with questionnaires focusing on satisfaction with the PPHCT, satisfaction with the course of the dying phase, and the development of anxiety, depression, and prolonged grief disorder.
Results:
Forty-three parent dyads participated (return rate, 88%). Satisfaction with the PPHCT scored a median of 10 (numeric rating scale, 0–10). The child's death was predominantly experienced as very peaceful (median, 9); 71% died at home. According to parents, involvement of the PPHCT led to highly significant (p<0.001) improvements in the children's symptoms and quality of life, as well as in aspects of communication and administrative barrier reduction. Anxiety was detected in 25% of parents, depression in 19%, and prolonged grief disorder in 13%. HCPs (return rate, 83%) evaluated all investigated care domains (particularly cooperation/communication/family support) as being significantly improved (p<0.001). Thirty-five percent of HCPs felt uncertain concerning pediatric palliative care; 79% would welcome specific training opportunities.
Conclusions:
Involvement of a PPHCT is experienced as a substantial improvement of care by parents and HCPs. Coordination of palliative care during the last phase of life appears to be an important quality factor for the home care of dying children and their families.
Introduction
Major barriers according to parents and health care professionals (HCPs) are lack of continuity of care, deficiencies in communication, ineffective symptom management, insufficient education, and—in particular—lack of coordination.6–27 Coordination is often seen as the gateway for problems and solutions.
It has been suggested that specialized pediatric palliative home care teams (PPHCT) could help in coordinating palliative care and improving communication between the different institutions and professionals involved.28–30 The goal of this study was to evaluate whether pediatric palliative home care can be improved by involving a PPHCT. Successful implementation of a new structure in the health care system requires that both the needs of HCPs and those of patients and their families are adequately addressed. Thus, assessment of the parents' and the HCPs' experience with the PPHCT's work were performed simultaneously.
Methods
Study site
The retrospective, nonrandomized study was performed from June to December 2007 at the Coordination Center for Pediatric Palliative Care (CPPC) at the University of Munich, Germany. The CPPC is a multiprofessional specialized PPHCT consisting of three pediatricians (an oncologist, a cardiologist, and a neonatologist), a nurse, a social worker, and a chaplain. It was implemented in 2004 to provide palliative home care for children, adolescents, and young adults with life-limiting diseases in southeastern Bavaria (population approximately 4.5 million). Main tasks of the team are coordination of professional assistance (e.g., transition of care between hospital and home, assistance in appropriate communication, etc.) as well as the provision of palliative treatment in cooperation with local HCPs and a 24/7 medical on-call service.31,32
Participants
Families that lost a child at least 3 months prior to the start of the study and that were receiving palliative home care through the PPHCT between March 2004 and March 2007 after a period of standard medical care were eligible for inclusion in the study. Their main PPHCT contact called them to give information about the purpose and procedure of the study. Families interested in participation were sent the questionnaire materials along with a cover letter, informed consent forms, and a return envelope.
Exclusion criteria were mental health disorder, missing contact data, one-time contact, significant language barriers, and prenatal or perinatal deaths.
All HCPs involved in the care of these children were sent a questionnaire along with a cover letter and return envelope.
The study was approved by the Research Ethics Committee of the University of Munich and only participants who provided informed consent were included.
Questionnaires
Parents
The two parental questionnaires were piloted in four families and adapted according to feedback. Parents were advised to contact the PPHCT for support if they developed psychological distress after completing the questionnaires.
Parental Questionnaire 1 (PQ1) comprised a total of 56 items, and was developed specifically for this study from a comprehensive literature search, review of validated tools, and clinical experience. It assessed sociodemographic data of respondents (8 items), information about the child's condition (4 items), satisfaction with specific aspects of the care provided by the PPHCT (22 items), quality of care before and after PPHCT involvement (12 items), and satisfaction with the dying phase (10 items). For most items, numerical rating scales (NRS, 0–10) were used. Parental Questionnaire 2 (PQ2) comprised validated questionnaires to assess anxiety and depression (Hospital Anxiety and Depression Scale, HADS, 14 items), 33 and prolonged grief disorder (PG-13, 13 items).34,35 PQ2 was distributed to mothers and fathers, and had to be completed individually.
Health care professionals
The Questionnaire for Health Care Professionals (QHCP) was also developed specifically for this study. In a focus group with nine experienced pediatric palliative care professionals, factors regarded as important for successful PPC were identified. Items to capture these factors were written and reviewed by an expert panel. The final QHCP consisted of 22 items (NRS) on quality of care and communication before and after PPHCT involvement. In addition, space for open comments was provided.
Statistical analysis
Descriptive statistics (%, mean±standard deviation [SD], median, range) were calculated for information of the parents' and HCPs' sociodemographic characteristics, objective care data, and evaluations of care. Since some of the variables were not normally distributed, Wilcoxon signed-rank test for nonparametric data was used to evaluate differences in quality of care before and during PPHCT care. The significance level was set at p<0.05. Bonferroni correction of p values for multiple comparisons was performed. Statistical Package for Social Sciences (SPSS, version 18.0, SPSS Inc., Chicago, IL) was used to analyze the data.
Results
Study participants
Parents and children
Of 106 consecutive families, 62 couples fulfilled eligibility criteria. Seventeen couples were excluded according to the exclusion criteria. Of the remaining 45 couples, 43 (96%) agreed to participate. PQ1 was returned by 38 of 43 parent sets (response rate, 88%). In 23 families, both mother and father completed the questionnaire with shared answers. In one case, PQ1 was completed by a father. In the remaining 14 families, mothers completed the questionnaire. PQ2 was returned by all participating mothers (n=38) and by 29 fathers (76%).
Most of the parents were 31 to 40 years old, 82% of respondents were married at the time of the survey, 20% of the families had a migration background. Seven percent of parents had elementary school-level education, 22% secondary school, 3% high school, and 29% university education.
Of the 38 deceased children, 24 were male, median age was 3.4 years (0–34.3). In one case a patient died as an adult but palliative care started during childhood. Congenital (including congenital heart disease) and oncologic diseases were the predominant underlying disorders (Fig. 1). In 82% of the families, there were siblings at the beginning of palliative care, 23% of whom were diagnosed with the same disorder. The interval between the child's death and the survey ranged from 3 to 37 months (median=19.5 months). Data on the care provided by the PPHCT are shown in Table 1.
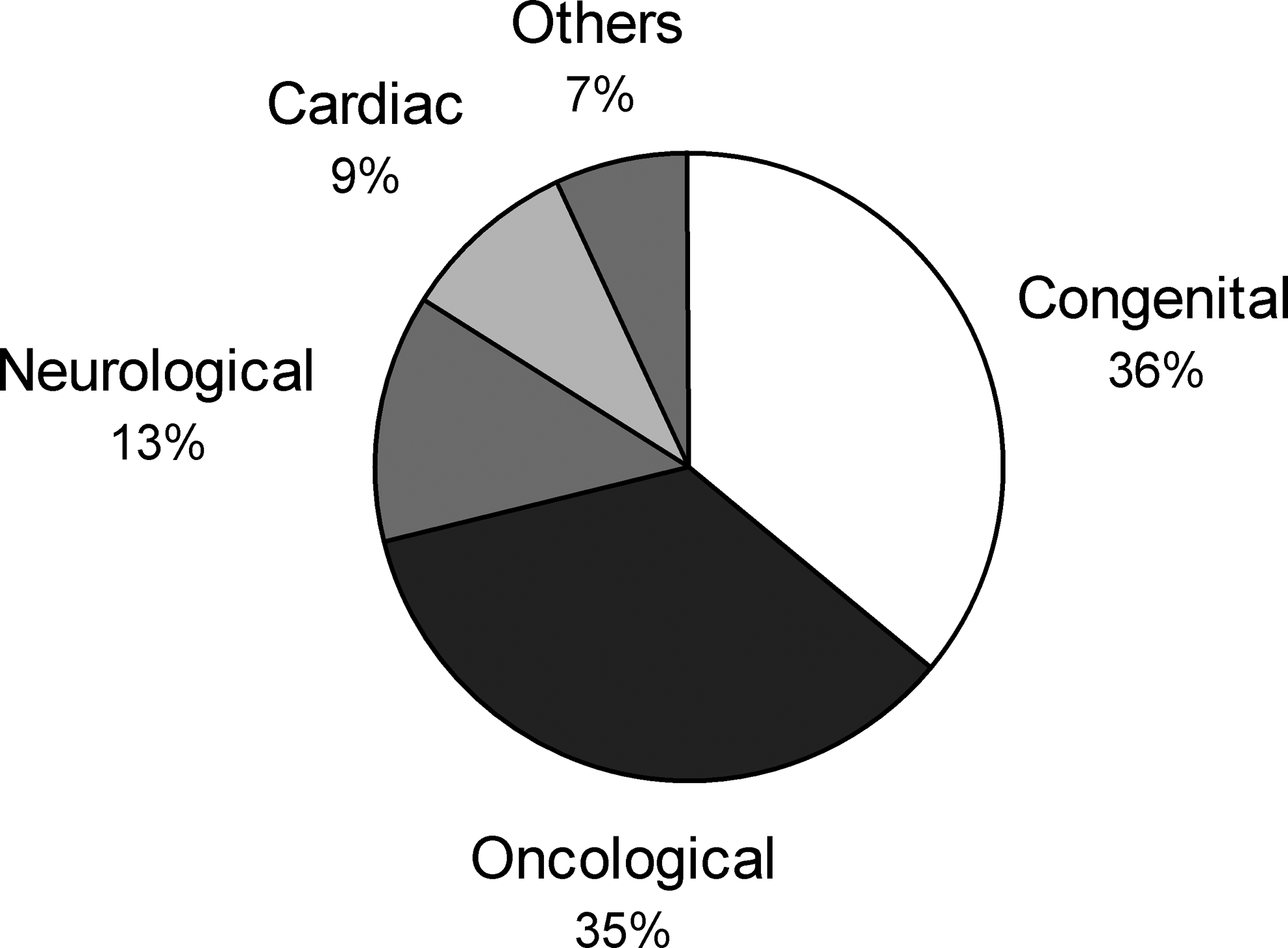
Underlying diseases by main categories (n=45).
PPHCT, pediatric palliative home care team.
Health care professionals
A total of 105 HCPs (54 physicians, 28 nurses, 8 social workers, 5 psychologists, 5 physiotherapists, 3 chaplains, and 2 case managers) were involved at least once in the palliative care of one or more of the 62 deceased children, and were thus sent the questionnaire materials. Eighty-seven HCPs returned the questionnaire (response rate, 83%) with an equal distribution among the professional groups.
Parents' assessment of care
Satisfaction with the PPHCT as a whole was rated on a NRS with a median of 10 (mean=9.2±1.69 [SD]; range, 4–10). Parents were asked to retrospectively evaluate quality of care before and during involvement of the PPHCT. There were significant improvements in 5 of 6 issues. Both parents' distress induced by perceived children's symptoms (p<0.0017, Fig. 2A), as well as distress through administrative barriers decreased (P<.0083). Children's QOL as evaluated by parents improved (p<0.0017, Fig. 2B), HCPs' willingness to listen to parental questions and/or problems increased (p<0.00017, Fig. 2C), and communication among HCPs improved as well (p<0.00017, Fig. 2D). After Bonferroni correction, the improvement in parents' satisfaction with being able to be there for their child was no longer significant.
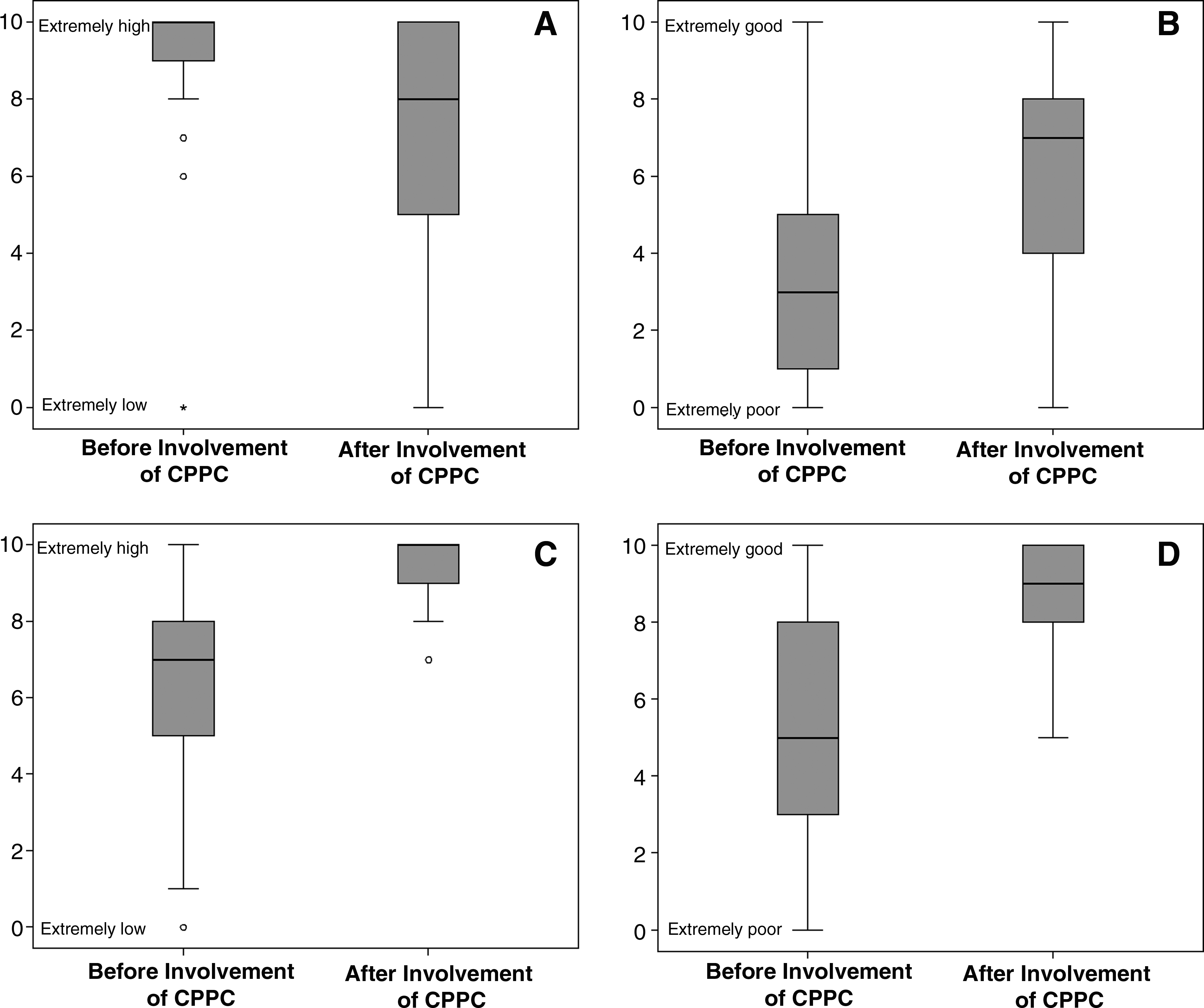
Box plot diagram (according to parents' ratings): Parents' distress due to children's symptom load (
Eighty percent of children had been in hospital before they were cared for at home or in a hospice. Evaluation of the transferring process from hospital (n=19) or hospice (n=2) to home was rated at a median of 8 (mean=7.3±3; range, 0–10). The 24/7 on call service of a PPC-specialized physician was rated as very important by 97% (median=10, mean=9.4±1.45; range, 3–10). 18% of the families never used the on-call service, 38% used it one to three times, and 44% used it more than three times. The siblings' needs were reported to have been sufficiently considered in 42% of cases.
Regarding the course of the dying phase, the child's death was evaluated as peaceful with a median of 9 (mean=8.4±2.53; range, 0–10). Of 38 parents, 37 (97%) stated that their child's dying place had been “a good place” for their child. Although 91% of parents reported that they had the opportunity to talk about death with the PPHCT and in 58% to talk about death with their own child, half of respondents stated that their child's death occurred in an unexpected, sudden way. In 21 cases, both parents were present at the time of death, in 12 cases the mother was present, and in 5 cases the child died at hospital without the presence of relatives.
Parents' adjustment after the death of the child
Parents' self-reported current QOL at the time of survey was rated at a median of 5 (10=highest possible QOL, mean=5.8±2; range, 1–10). Four parents indicated feeling rather lonely and wished to have more support. Parents rated their contentment with post-mortem care at a median of 8.5 (mean=7.1±3.2; range, 0–10).
Twenty-six percent of mothers and 24% of fathers showed clinically relevant anxiety (HADS anxiety score≥11). Twenty-one percent of mothers and 17% of fathers showed clinically relevant depression (HADS depression score≥11). Three mothers and two fathers developed prolonged grief disorder; this included one set of parents where both had developed prolonged grief. One mother asked for psychological support, as she was suffering from depression.
Parents' comments
Ninety-five percent of mothers and 89% of fathers left optional comments on their questionnaires. In most cases parents stated that they felt substantially relieved through the PPHCT involvement. Many parents would have liked earlier stage involvement of palliative care. Some parents felt that the PPHCT was working to full capacity just with caring for the dying child alone, so that not enough time might have been left to provide care and support to the remaining family and siblings.
HCPs
The HCPs' satisfaction with all assessed aspects of care improved significantly after involvement of the PPHCT. Amongst others, the increased support for the whole family is followed by improved cooperation and communication efforts among the care providers (Table 2). Thirty-five percent of the participants felt rather unsure in pediatric palliative therapy and symptom control, 30% in ethical or legal EOL issues, 79% would welcome specialized training, and 40% reported a lack of psychosocial support for themselves (e.g., supervision). The identification of these issues was evenly spread among different health care professions, except for psychosocial support, where psychosocial professionals felt better supported than the other groups
NRS related scores: 0=lowest quality,10=highest quality.
P<.001 (Wilcoxon signed-rank test [two-tailed]; Bonferroni-corrected P<.00014)
PPHCT, pediatric palliative home care team; CPPC, Coordination Center for Pediatric Palliative Care.
Sixty-four percent of HCPs left optional comments on their questionnaires. In 53 cases they reported that working with a PPHCT makes them feel more assured in their work. Many HCPs (mostly nurses) stated that involving a PPHCT makes it possible to fulfill a family's wish to care for the child at home during the dying phase.
Discussion
Little data are available on the effectiveness of pediatric palliative care. Hays et al. 36 suggested that the children's QOL can be used as an indicator for the quality of EOL care. It can be influenced by optimizing communication, decision support, and co-case–management by care providers. The children's QOL, as assessed by the parents, significantly improved in our study.
From both the parents' as well as the HCPs' point of view, communication within the local caring team improved after PPHCT involvement as well. Parents stated that they felt more comfortable talking about death with their child after involvement of the PPHCT. Kreicbergs et al. 10 showed that communication regarding this sensitive issue may help to reduce psychological and physical post mortem distress.
PPC requires a broad multiprofessional approach, every single profession being an important part of the care team. By coordinating all HCPs involved, available help for the dying child and its family can be used more efficiently.37,38 Parents as well as HCPs stated that without coordination of home care valuable energies and resources get lost. In addition, some studies show that the hospital/home interface is a particularly sensitive point.39,40 Our results suggest that PPC can be very valuable in stabilizing this transition.
Assessment and management of symptoms and suffering in children are difficult.41,42 Several studies report problems in symptom relief for a large variety of different symptoms.10,22,43–46 In this study, symptom load in children appeared to decrease significantly after PPHCT involvement. Parents' perception of symptom alleviation might not only be due to medical amelioration, but also to the improvement of the care conditions. Wolfe et al. 47 stated that especially in cases of unsuccessful symptom control greater attention must be paid to the way symptoms are perceived. Importantly, parents in our study reported an improved quality of life after PPHCT involvement, although their child's palliative situation progressed steadily.
Available data show that it is of crucial importance for parents to receive information about when, where, and how the child will die.10,20 Most of the parents in our study experienced the child's death as very peaceful. The parents' wish that their child should die at home can usually be realized only in a minority of cases. A study on oncologic patients in PPC suggested that this number can be raised by adjusting care structures to the children's and parents' needs. 48 We found that the PPHCT enabled children to die at home in the majority of cases, which correlates with the parents' high satisfaction regarding the place of death. Overall, the percentage of children dying at home was raised from 50% to 92% for children over one year of age and from 10% to 41% for infants less than one year of age through involvement of the PPHCT. Our data support the claim that a 24/7 on call service is a vital factor to ensure feelings of safety in the parents.
The loss of a child is one of the most stressful life events possible, often resulting in a crisis of meaning. Parents use rational and irrational strategies to cope with this event and find a renewed purpose in life. 49 In our study, clinically relevant levels of anxiety and depression developed in about 25% of parents, mostly within the same couple. Thus, appropriate PPC might be a method to alleviate the grieving period, which is known to be particularly severe in bereaved parents.49–52
A high demand in specialized training opportunities for HCPs as identified by previous studies is clearly supported by our findings.53–56 In addition, psychological support for HCPs is needed to limit distress among professionals in this highly wearing field.
This study has several limitations. Findings are primarily based on parents' perceptions, the recollection of which may change over time. Particularly, the retrospective collection of QOL data increases this bias. Additionally, parents' responses may be subject to social desirability. Due to the broad and sensitive spectrum of assessed items we developed tailored questionnaires which included non validated scales. The validation of these survey instruments will be subject of further studies. Absolute numbers are small, which limits generalizability, particularly as this is a single-center study. On the other hand, sampling errors were reduced by contacting all consecutive families who were in the care of the PPHCT during a specified period of time.
Conclusions
According to the parents, involvement of a specialized PPHCT led to a significant improvement in relevant domains of palliative care investigated. Coordination of the HCPs involved in the last phase of life appears to be a pivotal quality factor for home care of dying children and their families. Working with a PPHCT was also experienced as a substantial improvement by the involved HCPs, who report a high demand for training opportunities in PPC. Additional multicenter studies are needed to optimize the care provided to dying children and their families.
Footnotes
Acknowledgments
The authors express their gratitude to the families and health care professionals who shared their experiences in the hope of improving services. The authors are also grateful to Holly G. Prigerson and Ulrika Kreicbergs for their support in the preparatory stage of the study.
Author Disclosure Statement
No competing financial interests exist.