
Abstract
Abstract
Objectives:
There are limited studies characterizing cancer-related symptoms in outpatient advanced prostate cancer patients. The aim of this retrospective study was to describe the impact of an outpatient palliative care (PC) consultation on symptoms in patients with advanced prostate cancer.
Methods:
We retrospectively reviewed the medical records of 55 consecutive patients with advanced prostate cancer seen in our institution's outpatient PC center. Information regarding demographics, disease status, Edmonton Symptom Assessment System (ESAS) scores, Eastern Cooperative Oncology Group (ECOG) Performance Status, laboratory data, and pharmacological interventions were analyzed.
Results:
The median age of the study's patients was 66 years old, with 73% Caucasian ethnicity. All patients had metastatic disease and 96% had received prior cytotoxic chemotherapy. The most frequently occurring symptoms upon presentation were pain, fatigue, and drowsiness (>50%). Pain and fatigue were also the most severe symptoms, each having median ESAS scores of 7 (on a 0–10 scale). We instituted a median of 3 pharmacological interventions per patient, with a median of 15 days to follow-up assessment. At follow-up, patients reported significant symptom improvements in pain, drowsiness, fatigue, depression, sleep, sense of well-being, and anxiety.
Conclusions:
Based on our preliminary data, we conclude that patients with advanced prostate cancer referred to PC experience severe and clinically significant symptoms. An outpatient PCconsultation is associated with significant symptom improvement in this subset of a distressed population. Future prospective studies are warranted to further describe symptom burden and the role for outpatient PC for advanced prostate cancer patients.
Introduction
There are limited investigations that characterize the symptom burden and the impact of the outpatient palliative care (PC) consultation in advanced prostate cancer patients referred to outpatient supportive care center. In this retrospective review we aim to characterize the frequency and severity of symptoms in advanced prostate cancer patients referred to outpatient supportive care center and the impact of an outpatient PC consultation.
Methods
We retrospectively reviewed 55 charts of consecutive, prostate cancer patients who had been referred to the outpatient PC center at M. D. Anderson Cancer Center from January 2003 to December 2008. The Institutional Review Board approved this study.
Process of the outpatient palliative care service
Care is provided by a PC team led by board-certified PC specialists. All 10 specialists work as a team and provide mutual coverage in cases of absence or illness so that there are never clinic cancellations. This helps the team maintain a homogeneous approach to assessment, management, and communication with patients and their families. The other team members include a palliative trained registered nurse, a pharmacist, a nutritionist, a chaplain, a social worker, and a counselor. Other services such as wound management, speech therapy, occupational therapy, and physical therapy are consulted when needed. The care of all patients follows a standardized management plan. 7 Patient and their families are initially assessed by the palliative trained registered nurse using tools such as the Edmonton Symptom Assessment Scale (ESAS), and constipation and family support questionnaires. The findings are then discussed with a PC specialist, who then conducts an interview with the patient and the family and performs a physical examination. The physician and nurse then ask appropriate members of the interdisciplinary team to participate based on the patient's and family's individual needs. These interventions and care provided by the interdisciplinary team follow PC guidelines established by the National Comprehensive Cancer Network and National Consensus Project. 2 These guidelines focus on (a) assessing and managing cancer-related symptoms; (b) providing assistance to the patient's and caregivers' understanding of the disease and treatment goals; and (c) providing assistance to the patient and her or his caregivers in coping with the life-threatening illness and in decision making.
Patients were eligible for inclusion if the following criteria were met: (1) a diagnosis of advanced prostate cancer defined as locally recurrent or metastatic; (2) seen at both the genitourinary oncology clinic and the PC clinic; and (3) attended at least one outpatient follow-up visit within 1 month of the initial PC consultation. Data regarding patient age, disease state, ESAS score, Eastern Cooperative Oncology Group (ECOG) Performance Status, and survival were reviewed. In addition, laboratory data, including hemoglobin, testosterone, and prostate-specific antigen (PSA) levels were collected. Medication changes resulting from our initial PC consultation were recorded.
The ESAS was designed to determine the severity of 10 symptoms commonly experienced by cancer patients during the previous 24 hours. These symptoms are pain, fatigue, nausea, depression, anxiety, drowsiness, dyspnea, anorexia, insomnia, and feelings of well-being. The ESAS has been validated and proven reliable in the assessment of symptoms in cancer patients. 6
We reported descriptive statistics as percentages of patients reviewed, and calculated the median values for patient characteristics and ESAS assessments. Analyses were performed using GraphPad Prism version 5.02 for Windows (GraphPad Software, San Diego, CA). The statistical significance between the baseline and follow-up ESAS scores was calculated using the Wilcoxon signed-rank test. Statistical significance was defined as a P value<0.05.
Results
The patient characteristics are summarized in Table 1. Excluded were 1733 patients seen in the outpatient supportive care center during the same time period because they had diagnoses other than advanced prostate cancer.
ECOG, Eastern Cooperative Oncology Group.
Fatigue, drowsiness, and pain were the most frequent clinically relevant symptoms (defined as ≥4 on the ESAS) as shown in Fig. 1. The median numbers (interquartile) of clinically relevant ESAS symptoms per patient were 4 (3–6) and 3 (1–5) at baseline and follow-up, respectively (P=0.14). The median time to follow-up from baseline was 15 days. As illustrated in Fig. 2, patients had statistically significant improvement from baseline to follow-up assessment in 7 of the 10 ESAS symptoms.
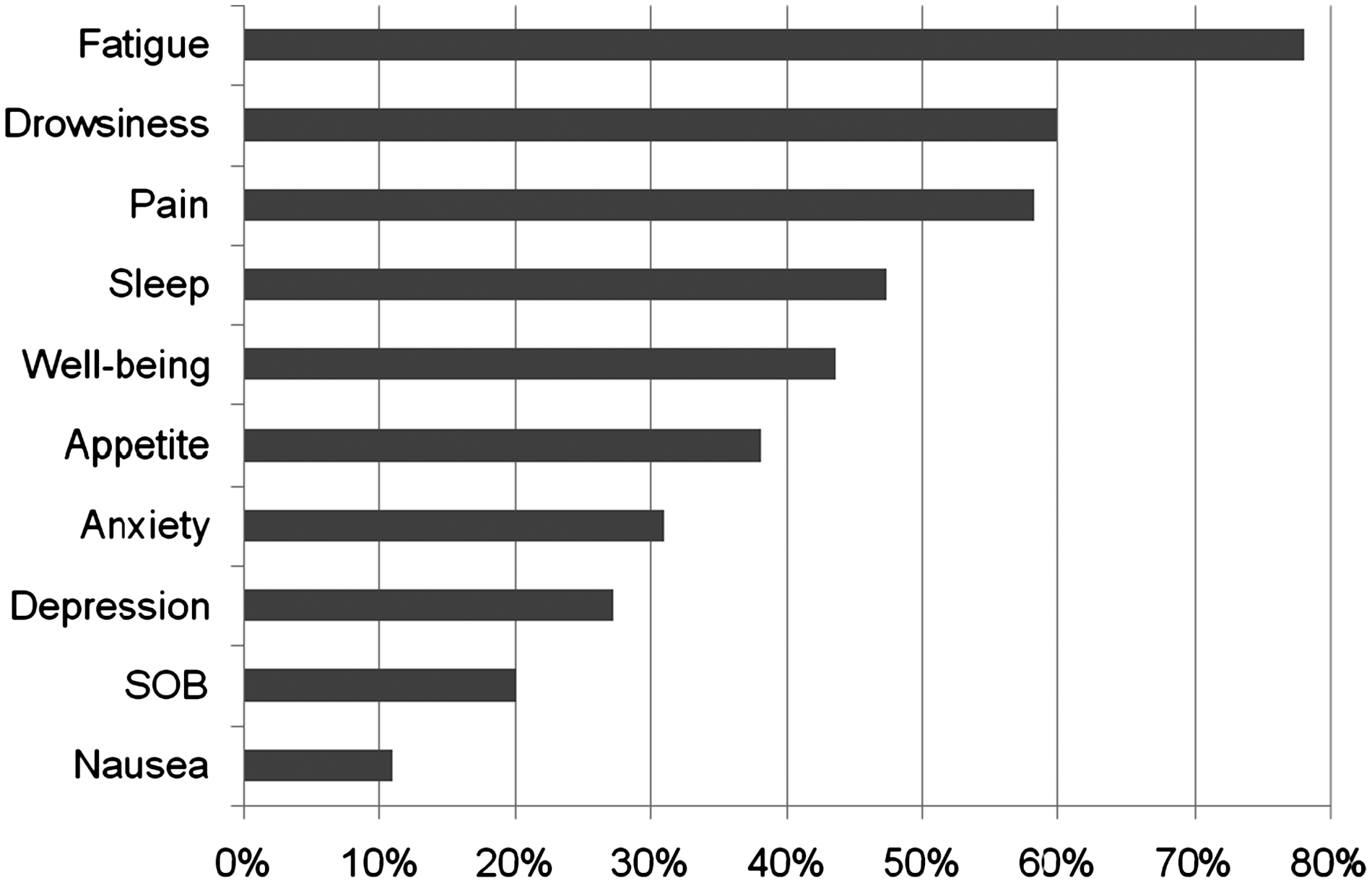
Patients with symptom severity ≥4 by Edmonton Symptom Assessment System at baseline (n=55).

Median symptom scores of patients with symptom severity ≥4 at baseline by Edmonton Symptom Assessment System and at follow-up.
The median pharmacological interventions (medication discontinuation, initiation, and frequency or dosage adjustments) per advanced prostate cancer patient at initial consult were 3 interventions (1.5–4 interventions; interquartile). The most frequent medication interventions included adjustment or initiation of opiates (69%), laxatives (40%), antiemetics (22%), methylphenidate (20%), and antipsychotics (20%) as shown in Fig. 3. All patients also received supportive counseling from the PC team.
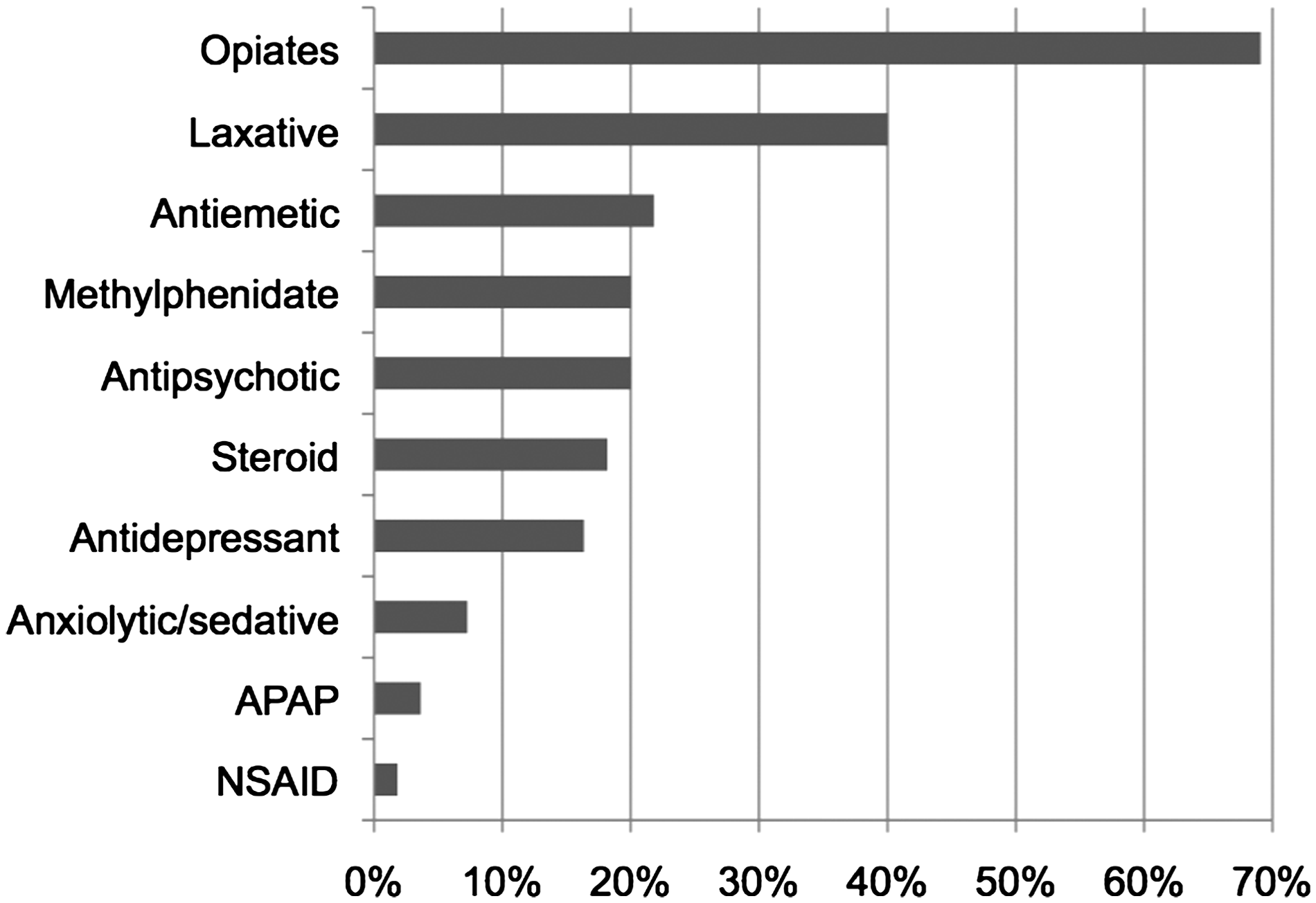
Medication interventions by class completed at baseline consult by the outpatient palliative care service.
At the time of our retrospective review, 98% of patients were deceased with a median of 175 days from baseline PC consultation to death.
Discussion
Our report demonstrates that patients with advanced prostate cancer presenting to outpatient supportive care center often experience severe and clinically significant symptoms. We found that consultation with an outpatient PC service was associated with statistically significant improvements in the patients' pain, drowsiness, fatigue, depression, sleep, sense of well-being, and anxiety.
Data are limited on the severity of symptoms in advanced prostate cancer patients and on the impact of a consultation with a PC service.8–10 Many investigations regarding the palliation of symptoms for advanced prostate cancer patients have emphasized the timing and frequency of hormone deprivation therapy in the androgen-dependent prostate cancer setting or the palliation of bone pain with radiotherapy or cytotoxic chemotherapy for advanced androgen-independent prostate cancer (AIPCa). Other measures for symptomatic relief for metastatic bone disease include narcotic analgesics, corticosteroids, bisphosphonates, radiation therapy, radioisotopes such as strontium-89, and cytotoxic chemotherapy.7–13
In the present study, the median duration between referral to the PC service and death in patients with advanced prostate cancer was 175 days and compares favorably with overall timing of outpatient cancer patients referral to PC as in prior published studies by Dalal and colleagues of 141 days (outpatients PC), 15 and by Osta and co-workers of 42 days (inpatient and outpatient). 16
In our study, 7 out of 10 symptoms evaluated improved significantly at follow-up assessment. Similar to other studies involving patients with advanced cancer, referrals to our PC service also occurred when the course of illness seemed imminently threatening.14–17 However, the World Health Organization states, “Palliative care is applicable early in the course of illness, in conjunction with other therapies that are to prolong life, such as chemotherapy or radiation therapy.” 18 Early referrals to the PC service are essential to supporting quality of life and providing early relief of physical and psychosocial distress, including pain and fatigue.14,19–21
Our analysis is also consistent with previous reports that significant pain is one of the most common morbidities experienced by men with AIPCa. More than 90% of men with AIPCa develop bone metastases and experience debilitating bone pain. 22 In our investigation, 58% of AIPCa patients had clinically significant pain (defined as ESAS score ≥4) at presentation to the outpatient PC clinic. Not surprisingly, optimizing opiate regimens and treatment of constipation were the most common pharmacological interventions at baseline (in 69% and 40% of patients, respectively).
Fatigue was the most frequent symptom of patients presenting to the PC clinic, with a 78% incidence of clinically significant fatigue (ESAS ≥4). In addition to the high frequency of this symptom, it also tended to have a high level of severity, with the median ESAS score for fatigue being 7. There were likely several contributing factors to the fatigue experienced in our patient population, including the effects of pain, anemia, sleep disturbance, malnutrition, emotional distress, and having received cytotoxic chemotherapy. 23 In addition to these contributing factors, all patients had hypogonadism with a median testosterone level of 20.5 ng/dL (range, 10–198). Androgen deprivation is considered the cornerstone treatment of metastatic prostate cancer. 2 Despite the progression to an androgen-independent state, androgen deprivation is seldom discontinued due to the coexistence of androgen-dependent cancer cells and the increased symptoms and decreased survival observed in an androgen-enriched state.24–26 Androgen deprivation can increase fatigue for patients with advanced or recurrent prostate cancer and decrease quality of life from baseline levels.27,28 In addition, androgen deprivation is known to occur in patients with advanced cancer and in those with chronic opiate exposure.29,30 There have been few investigations into the incidence, severity, and factors associated with fatigue in advanced prostate cancer patients.
A major limitation of this study was that it was a retrospective review of data. Another limitation of the study was the limited sample size due to the few prostate cancer patients referred to the outpatient PC clinic (55/1788). There is also risk of bias in regards to the impact of PC as reduction of symptoms at follow-up could be due to PC and concurrent chemotherapy (administered with PC in 69% of patients). Prior studies have found chemotherapy itself could improve pain and quality of life. 5
Conclusion
In our preliminary review, patients with advanced prostate cancer who were referred to the outpatient PC clinic had severe symptom distress. The PC consultation was associated with significant improvement in ESAS scores for several symptoms and overall well-being at follow-up. Future prospective studies to investigate the impact of interventions provided by PC services for advanced prostate cancer patients are warranted.
Footnotes
Acknowledgments
Drs. Yennurajalingam and Atkinson contributed equally to this paper.
Author Disclosure Statement
No competing financial interests exist.