
Abstract
Abstract
Introduction:
Prognostic scoring systems are increasingly used in cancer care. One of these systems is the Palliative Prognostic Index (PPI) which is based on clinical findings. Few studies validated the PPI in different settings. Our aim was to test the predictive value of the PPI in an acute cancer care setting.
Methods:
Prospective study that included patients with advanced cancer admitted to a tertiary cancer center in Kuwait. Patients were divided according to the PPI score into three groups: A (PPI≤3), B (PPI>3– ≤6), and C (>6).
Results:
The study included 91 hospitalized patients. At the time of PPI assessment, the plan of treatment was best supportive care only in 70 (77%) patients. The majority (80%) of included patients died in-hospital. The in-hospital mortality rate for patients with a PPI>6 was significantly higher than those with ≤6 (93% versus 56%, p<0.001). Using a cutoff point of PPI>6, in-hospital mortality was predicted with a 73% sensitivity, 78% specificity, 93% positive predictive value, and 41% negative predictive value. The median survival was 61 days (95% confidence interval [CI]: 25.8–96.2) for group A, 20 days (95% CI: 4.5–35.5) for group B, and 6 days (95% CI: 4–8) for group C. The difference in survival was highly significant (p<0.001).
Conclusion:
The results suggest that the PPI may be helpful for oncologists in predicting survival and in-hospital mortality of patients with advanced cancer in the acute care setting.
Introduction
Although physicians' prediction of survival was found to be an independent predictive of prognosis, 2 it is known that physician's estimation is generally inaccurate and overoptimistic. 3 A number of factors may be useful in predicting survival in patients with advanced cancer. Performance status scoring systems like the Eastern Cooperative Oncology Group and the Karnofsky Performance Status scales and a number of quality of life measurement scales were found to be of predictive value. 1 Also, some symptoms such as tiredness, dyspnea, and anorexia independently predicted survival.2,4,5 In addition, a number of biological parameters were found to be independently predictive of survival of patients with advanced cancer like the total white blood cell count and the lymphocyte percentage. 6
In order to overcome inaccurate prediction when using the above mentioned factors individually, a number of prognostic models incorporating many predictive factors were developed like the Palliative Prognostic Index (PPI).1,7
The PPI was developed by Morita et al. 4 in 1999 and is based on five clinical parameters: the palliative performance scale, oral intake, edema, dyspnea at rest, and delirium. It is a simple index that does not include biological parameters and its use for survival prediction is of more value near the end-of-life. 7
In previous studies, patients were stratified according to the PPI score into groups with significantly different survival, being shorter for higher scores.4,8 The predictive value of the PPI was validated in few studies, mainly in a palliative care setting.4,8–10
The aim of the current study was to assess the ability of the PPI to predict the survival and in-hospital mortality in a different setting, an acute cancer care facility in Kuwait.
Methods
This is a prospective observational study to test the PPI's ability to predict the survival and in-hospital mortality of patients with advanced cancer. The study included hospitalized adult patients (age ≥18 years) with pathologic diagnosis of cancer and evidence of advanced disease beyond cure. Patients with cancer receiving anticancer treatment with curative intent were excluded.
The PPI was assessed according to the guidelines described by Morita et al. 4 who developed the index. The five items of the PPI and the partial score assigned to each item are illustrated in Table 1.
The total PPI score ranges from 0 to a maximum of 15; where 0 indicates the best performance status and absence of symptoms associated with poor prognosis, and 15 indicates the worst performance status and the presence of all the four poor prognosis symptoms.
The Palliative Performance Scale in its second version (PPSv2) was assessed according to the instructions described by Victoria Hospice Society. 11 The PPS assesses the functional status of the patient using five parameters: ambulation, activity and evidence of disease, self-care, intake, and conscious level. On a scale from 100% to 0% with 10% decrements the PPS divides patients into 11 categories where 100% signifies normal functional status and 0% signifies death.
Delirium was diagnosed according to the diagnostic criteria of delirium due to a general medical condition described in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 12
According to the total PPI score, patients were divided into three groups: group A with a PPI≤3, group B with a PPI ranging from >3 to ≤6, and group C with a PPI>6.
Pearson χ2 test was used for comparison of proportions. Independent sample t test was used to compare means between two groups. Survival was calculated from the date of PPI assessment to the date of death or last follow-up. The Kaplan-Meier method was used to estimate survival, and the log-rank test was used to test the significance of difference in survival. Statistical methods were performed using the Statistical Package for the Social Sciences (SPSS), version 17 (SPSS Inc, Chicago, IL). A p value<0.05 was considered significant.
Results
Patients' characteristics are shown in Table 2. Among the 75 patients with solid tumors, 58 (77%) had evidence of distant metastases and the most common sites were liver in 29 (38.7%) patients, bone in 19 (25.3%), lung in 18 (24%) and brain in 13 (17.3%). Twenty-one (23%) patients were receiving anticancer treatment with palliative intent. The anticancer treatment was chemotherapy in 19 patients, combined chemotherapy and radiotherapy in one and radiofrequency in one. For the majority (77%) of included patients, the decision was to stop further anticancer treatment and to continue supportive care only.
The prevalence of the PPI individual items is shown in Table 3.
The mean PPI score of patients who died in-hospital was significantly higher than that of those who were discharged alive (8.2 [± 3.8] versus 3.2 [± 2.9]; p<0.001). Patients with a PPI>6 were more likely to die as inpatients compared to those with ≤6 (93% versus 56%, p<0.001).
Using the cutoff point of PPI>6, in-hospital mortality was predicted with a sensitivity of 72.6% and a specificity of 77.7%. The positive predictive value (PPV) was 93% and the negative predictive value (NPV) was 41.2%.
The median survival, calculated from the date of PPI assessment, differed significantly between groups A, B, and C and was 61 days (95% CI: 25.8–96.2), 20 days (95% CI: 4.5–35.5), and 6 days (95% CI: 4–8), respectively (p<0.001).
Kaplan-Meier survival curves of the three groups are shown in Figure 1.
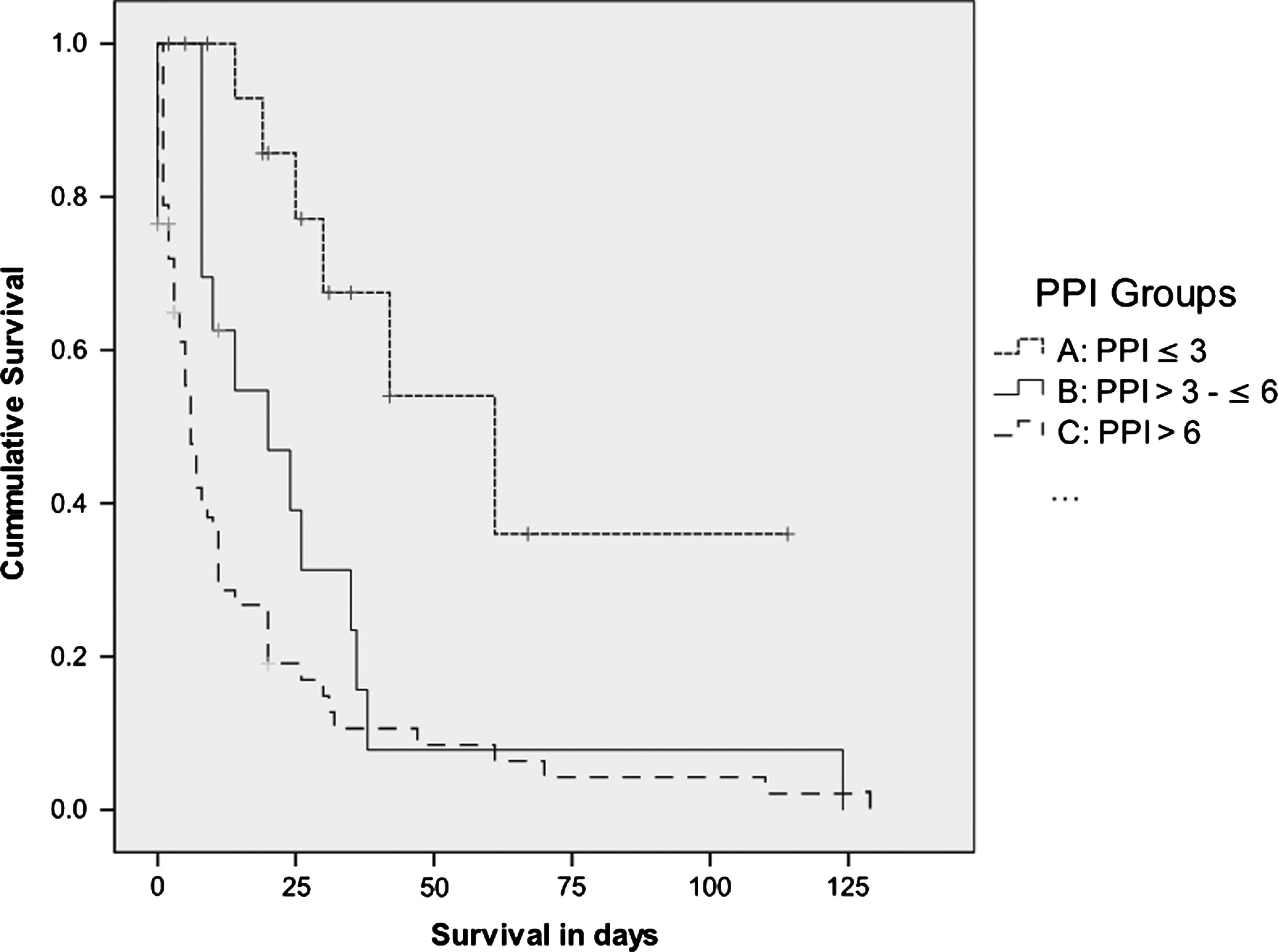
Kaplan-Meier survival curves calculated from the date of Palliative Prognostic Index (PPI) assessment.
Among the 21 patients who were receiving anticancer treatment with palliative intent, the survival of patients with a PPI>6 was shorter than those with a PPI≤6 (median=11 days [95% CI: 0–24] versus not reached, mean=18 days [95% CI: 0–39] versus 77 days [95% CI: 48–106]; respectively). The difference was statistically significant (p=0.015).
In addition, among the same group, the percentage of patients with a PPI>6 who were discharged alive was less than that of patients with a PPI≤6 (38% versus 69%, respectively). However, the difference was not statistically significant (p=0.15).
Discussion
Since the development of the PPI by Morita and colleagues 4 in a palliative care unit in Japan, few studies tested its predictive value in different settings. Stone et al. 8 validation study was carried out in an Irish specialist palliative care service that included a consultancy service based in a large teaching hospital, a community-based hospice home care service and a six-bed hospice inpatient unit. Shrope-Mok et al. 9 form the United States conducted their study in the intensive care unit (ICU) setting.
Another study from a palliative care consultation service in Australia included a subset (35%) of non-cancer patients. 10 The population of the current study is more similar to that of Stone et al., 8 which included patients with cancer only and a group of them was receiving anticancer treatment. The setting of this study is different from the previous studies in that it was carried in a tertiary cancer care centre away from specialist palliative care services. This may reflect the value of the PPI for oncologists.
Using the PPI cutoff points of 3 and 6, patients included in the current study were divided into three groups of significantly different survival. This confirms the usefulness of the PPI in predicting survival which was illustrated in other studies.4,8 However, there is no consensus regarding the cutoff points. Morita et al. 4 used cutoff points of 2 and 4 while Stone et al. 8 used cutoff points of 4 and 6. The difference in results between our study and others may be due many factors like differences in the population studied and sample size and the variability in clinical judgment. For example, in the population investigated to develop the PPI, 49% had gastrointestinal malignancies and 6% had breast cancer 4 ; compared to 15% and 19%, respectively, in the current study. Furthermore, half of the cancer population in Kuwait are non-Kuwaitis, and the majority are expatriates from lower-income countries where cancer is diagnosed usually in a late stage (unpublished data).
Reports from around the world show that a significant proportion of cancer patients still die in acute care facilities. 13 Hence, the availability of a clinical tool to predict in-hospital mortality effectively would be useful to improve the end-of-life care of advanced cancer patients. This is the first report to test the ability of the PPI to predict the in-hospital mortality in a group of patients with cancer admitted to a cancer center. In one study the prediction of in-hospital mortality using the PPI was conducted in a community hospital ICU and included patients other than cancer patients and the actual contribution of cancer patients to the study sample was not clear. 9 In that study, a PPI with a cutoff point ≥6 predicted the ICU mortality with a 69% sensitivity, 92% specificity, 36% PPV, and 98% NPV. However, the PPI was less sensitive than the Acute Physiology and Chronic Health Evaluation (APACHE) IV in predicting mortality. 9 In the current study, a PPI>6 predicted in-hospital mortality with a 73% sensitivity, 78% specificity, 93% PPV, and 41% NPV. These figures suggest that the PPI may be a useful tool for oncologists in predicting the in-hospital mortality of patients with advanced cancer.
Administration of chemotherapy near the end-of-life of patients with cancer is considered an indicator of poor quality end-of-life care. 14 The palliative prognostic scoring systems may be of help for oncologists in selecting patients who are unlikely to benefit from palliative chemotherapy. Tassinari et al. 15 and Giovani et al. 16 suggested the introduction of another palliative prognostic scoring system, the Palliative Prognostic (PaP) Score, to select patients who may benefit from palliative chemotherapy and to reduce chemotherapy administration near the end of life.
The results of the current study suggest that the PPI may be another useful tool for oncologists, not only for predicting in-hospital mortality and survival, but may be useful as well in determining when to stop systemic chemotherapy for patients with advanced cancer. Although the number of patients receiving cancer-modifying therapy was small in the current study, sub-analysis of this group of patients showed that a PPI>6 was associated with a significantly lower survival of only 11 days and more likelihood to die in-hospital. In the study conducted by Stone et al. 8 to validate the PPI, 43% of included patients with cancer were receiving anticancer treatment. However, in their article, they applied the statistical analysis to the whole group of patients including those not receiving anticancer treatment. 8
In conclusion the PPI may be a useful tool for oncologists in predicting survival and in-hospital mortality of advanced cancer patients. Further studies including larger number of patients and a better design may be needed to test the predictive value of the PPI in cancer care settings other than palliative care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.