
Abstract
Abstract
Background:
Although pain, sexual dysfunction, and depression are common in patients receiving chronic hemodialysis, these symptoms frequently remain untreated. We sought to characterize renal provider perceptions and practice patterns regarding the treatment of these symptoms.
Methods:
We surveyed renal providers whose patients were participating in a clinical trial of symptom management at nine hemodialysis units in southwestern Pennsylvania. We used Spearman's correlation to assess the association of provider characteristics with the reported frequency of providing treatment.
Results:
Overall, 27 of 35 (77%) providers completed the survey. While 21 (78%) believed symptom management to be “very” important and 23 (85%) reported spending a “moderate” to “a lot” of time managing symptoms, <50% reported treating pain and <20% reported treating sexual dysfunction or depression “most” or “all” of the time. Most providers believed it was nonrenal providers' responsibility to treat these symptoms. A greater reported comfort level managing symptoms was associated with a higher reported frequency of treating pain (r=0.6; p<0.01), sexual dysfunction (r=0.67; p<0.01), and depression (r=0.43; p<0.03). Providers who believed it was nonrenal providers' responsibility to treat these symptoms reported treating pain (r=−0.62; p<0.01) and depression (r=−0.48; p=0.02) less frequently.
Conclusions:
Despite reporting considerable importance and substantial time managing symptoms in general, renal providers commonly describe not treating pain, sexual dysfunction, and depression in hemodialysis patients. Given renal providers' beliefs that nonrenal clinicians are primarily responsible for treating these symptoms, multidisciplinary approaches to symptom management in these patients are needed.
Introduction
Methods
Study population
We surveyed renal providers caring for hemodialysis patients enrolled in a multicenter randomized clinical trial comparing two strategies for the management of pain, sexual dysfunction, and depression (the Symptom Management Involving End-Stage Renal Disease [SMILE] study). 24 The parent trial enrolled patients from nine outpatient dialysis units in metropolitan Pittsburgh, Pennsylvania, including VA, academic, and private practice units. The current study was a stand-alone ancillary study to the parent trial. Study procedures were approved by the institutional review board (IRB) of the VA Pittsburgh Healthcare System.
Survey administration and data collection
Using an investigator designed survey (Appendix), we assessed four discrete domains related to provider perceptions and practice patterns for the management of pain, sexual dysfunction, and depression: 1) extent of past training on the management of these three symptoms, 2) level of comfort managing these symptoms, 3) perceptions of who is primarily responsible for the provision of therapy, and 4) frequency of treatment. Additionally, the survey assessed the importance renal providers attach to and time spent managing symptoms in general. During the conduct of the parent trial (June-December 2010), study personnel mailed or personally delivered the survey along with a cover letter describing the survey's purpose, an informed consent form, and a pre-stamped return envelope.
Statistical analyses
We described survey responses using medians with interquartile ranges (IQR) for continuous data and frequencies for categorical data. We used Spearman's correlation coefficients to describe the associations of providers' past training, comfort, perceptions of responsibility, importance attached to and time spent on symptom management, years treating hemodialysis patients, and number of active hemodialysis patients with the frequency that providers reported treating pain, sexual dysfunction, and depression. Statistical significance was computed using exact methods and is denoted by a two-tailed p-value <0.05. All analyses were conducted using Stata 11.0 (College Station, TX) and SAS 9.2 (Cary, NC).
Results
Provider characteristics
Overall, 27 of 35 (77%) renal providers completed the study survey (20 nephrologists, 5 physician assistants, and 2 nurse practitioners). Providers' median age was 46 years (IQR 37, 55); 17 (63%) were male; and 20 (74%) were white. Respondents reported a median of 16 years of experience treating dialysis patients (IQR 8, 26) and a median of 45 hemodialysis patients actively under their care (IQR 35, 100). Providers reported evaluating their hemodialysis patients a median of three times per month (IQR 1, 4), with most spending 10 minutes at each visit (median 10; IQR 10, 10).
Survey responses
Nearly half of providers reported “little” prior training on the treatment of pain (N=12; 44%) or depression (N=11; 41%), while 22 (82%) reported “little” or “no” prior training on the treatment of sexual dysfunction (Figure 1A). While 18 (69%) providers reported feeling “somewhat” or “very” comfortable treating pain and depression, less than half (N=13; 48%) reported being “somewhat” or “very” comfortable treating sexual dysfunction (Figure 1B). Over three quarters (N=21; 78%) of providers reported that symptom management in general was “very” important and 6 (22%) believed it was “somewhat” important. A total of 23 providers (85%) reported that they spent a “moderate” or “a lot” of time managing symptoms in general. However, only 8 (30%) reported treating pain “most” of the time, 3 (11%) described treating sexual dysfunction “most” of the time, and 5 (19%) reported treating depression “most” of the time (Figure 1C). Only 2 (7%) providers reported treating pain “all” of the time while none reported treating sexual dysfunction or depression “all” of the time (Figure 1C). The majority of renal providers reported that it was the responsibility of the patients' primary care provider or nonrenal clinician to manage these three symptoms (59% for pain, 63% for sexual dysfunction, and 82% for depression) (Figure 1D).
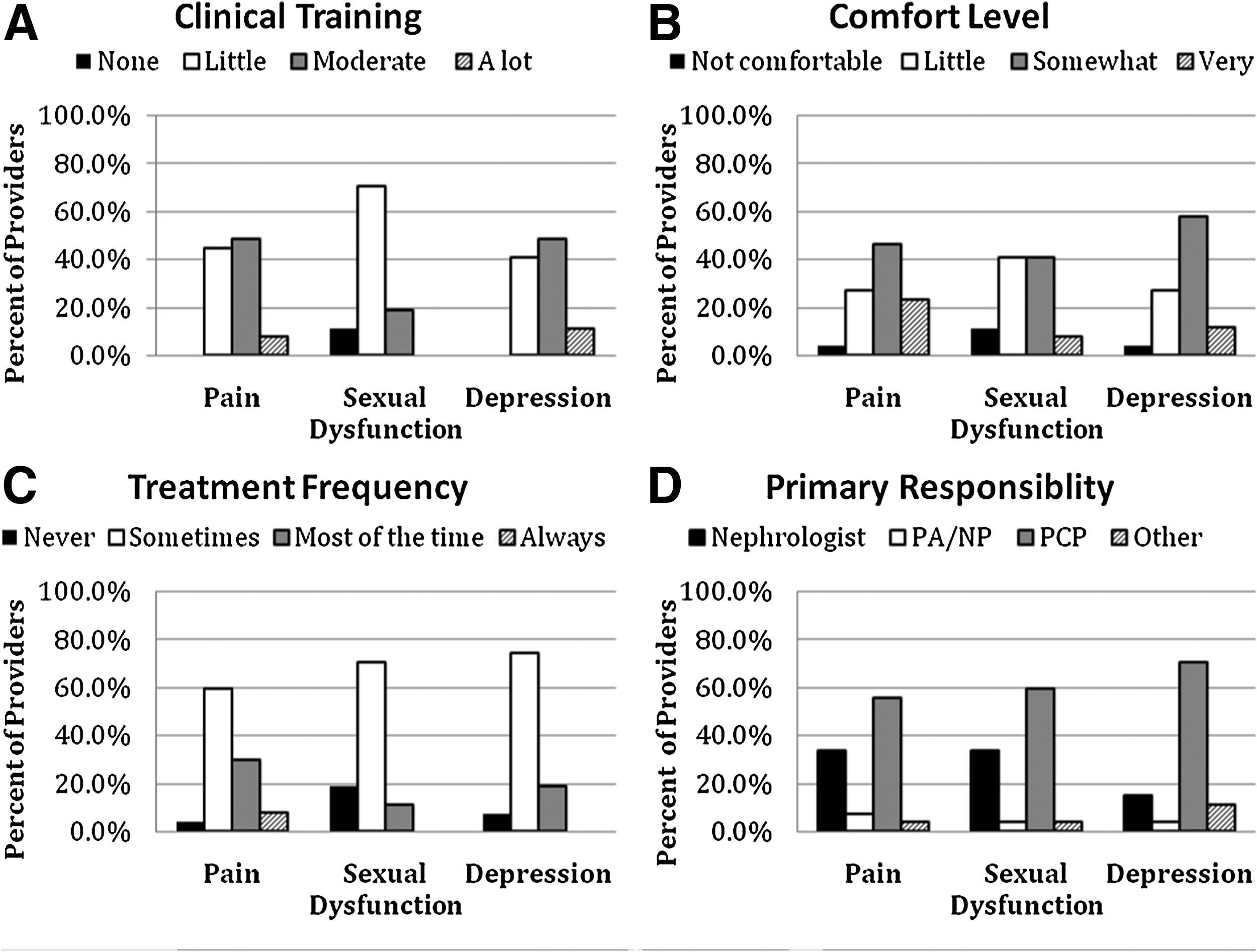
Provider survey responses regarding the management of pain, sexual dysfunction, and depression*. PA, Physician Assistant; NP, Nurse Practitioner; PCP, Primary Care Physician.
Associations among provider characteristics and perceptions with reported practice patterns
Greater levels of comfort treating pain, sexual dysfunction, and depression were associated with a higher reported frequency of treating each of these symptoms (Table 1). However, the extent of prior training on the management of pain, sexual dysfunction, and depression was not associated with the frequency with which providers reported treating these symptoms (Table 1). Similarly, the importance providers attached to symptom management in general, years of experience treating hemodialysis patients, and number of hemodialysis patients under their care were also not associated with the frequency with which they reported treating any of the three index symptoms (Table 1). However, renal providers who considered other clinicians (i.e., primary care providers, nonrenal specialists) to be primarily responsible for the management of pain and depression reported treating these symptoms less frequently than those who identified themselves as being responsible for the provision of treatment (Table 1). Provider type (nephrologist versus NP/PA), age, gender, and ethnicity had no impact on the frequency with which providers reported implementing treatment (data not shown).
Denote provider reported level of training on pain, sexual dysfunction, and depression; comfort managing these symptoms; and who they believe is responsible for the treatment of these three symptoms.
† Denotes importance provider attached to symptom management in general.
∑ Denote number of years of experience treating hemodialysis patients and number of active hemodialysis patients under their care.
Discussion
Although renal providers indicate that they attach significant importance to symptom management in general, a minority of providers in the current study reported that they treat these three symptoms most or all of the time. This is consistent with past research that has demonstrated that these symptoms are commonly undertreated in hemodialysis patients.17–23 The discordance between the importance renal providers attach to symptom management in general and the frequency with which they report actually providing treatment for these specific symptoms suggests that factors other than providers' concern for the burden of symptoms in their patients may be driving their practice patterns.
Many providers felt it was the responsibility of primary care providers to manage pain, sexual dysfunction, and depression in hemodialysis patients and this perception appeared to influence the frequency with which they reported treating these symptoms. Nearly half of patients participating in the parent trial reported that they considered their nephrologist to be their primary care provider. While we did not specifically record whether study patients actually had a primary care provider, this suggests that a substantial proportion of hemodialysis patients may not have any provider other than their nephrologist to manage these symptoms. In fact, several past studies demonstrated that nephrologists commonly function as the primary health care providers for many dialysis patients.25–29 The incongruence between the views of many renal providers, who report that symptom management is the responsibility of primary care and nonrenal providers, and hemodialysis patients, many of whom consider their nephrologist to be their primary care provider, may help explain the undertreatment of symptoms observed in prior studies. Efforts to better delineate provider responsibilities and to establish multidisciplinary approaches to patient care may facilitate the implementation of symptom ameliorating therapy in the hemodialysis population.
It is also possible that, despite the importance of symptom management, renal providers' practice patterns may be guided by pressures to achieve established clinical performance standards such as dialysis adequacy and anemia management, which are linked to payment through quality incentive programs for dialysis facilities. In this context, renal providers may not devote the time needed to manage symptoms in their hemodialysis patients. If so, this further emphasizes the need for multidisciplinary approaches to symptom management in this patient population that include collaboration with primary providers, social workers, and palliative care specialists.
Our study has several limitations. First, the sample size of providers was small, which may limit the generalizability of our findings. While we included nephrologists, nurse practitioners, and physician assistants from a variety of dialysis settings, future studies will need to validate our findings in larger numbers of providers. Second, our analyses were based on the relationship between provider characteristics and the frequency with which they reported treating symptoms in their patients, not the actual treatment provided. It is possible that symptom-alleviating therapies provided by nonrenal providers accounted for the frequency with which renal providers participating in this study reported not providing treatment for pain, sexual dysfunction, and depression in their hemodialysis patients. Finally, since renal providers were surveyed as part of their patients' involvement in a clinical trial related to symptom management, we cannot determine the impact of the parent study on provider perceptions and practice patterns.
In conclusion, renal providers attach significant importance to the management of symptoms in their hemodialysis patients in general, but report that they do not routinely provide treatment for pain, sexual dysfunction, or depression. Coupled with the observation that many renal providers view the management of these symptoms to be primarily the responsibility of nonrenal clinicians, these findings suggest that efforts to develop multidisciplinary approaches to optimize the provision of symptom-alleviating therapy in this chronically ill and highly symptomatic patient group are needed.
Footnotes
Acknowledgments
This study was funded by a grant from the Department of Veterans Affairs Health Services Research and Development Service (Weisbord HSR&D IIR 07-190). Dr. Green is supported by a grant from the American Kidney Fund Clinical Scientist in Nephrology Program.
Author Disclosure Statement
No competing financial interests exist. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.