
Abstract
Abstract
Background:
Improving access to palliative care is an important priority for hospitals as they strive to provide the best care and quality of life for their patients. Even in hospitals with longstanding palliative care programs, only a small proportion of patients with life-threatening illnesses receive palliative care services. Our two well-established palliative care programs in large academic hospitals used an innovative quality improvement initiative to broaden access to palliative care services, particularly to noncancer patients.
Methods:
The initiative utilized a combination of electronic and manual screening of medical records as well as intensive outreach efforts to identify two cohorts of patients with life-threatening illnesses who, according to University HealthSystems Consortium (UHC) benchmarking criteria, would likely benefit from palliative care consultation. Given the differing cultures and structure of the two institutions, each service developed a unique protocol for identifying and consulting on suitable patients.
Results:
Consultation rates in the target populations tripled following the initiative: from 16% to 46% at one hospital and from 15% to 48% at the other. Although two different screening and identification processes were developed, both successfully increased palliative care consultations in the target cohorts.
Conclusion:
Quality improvement strategies that incorporate pay-for-performance incentives can be used effectively to expand palliative care services to underserved populations.
Introduction
Despite increasing efforts to improve access to palliative care services, particularly to those with noncancer diseases,11,12 significant numbers of patients still have unmet end-of-life medical needs.13–16 Many patients who would benefit from palliative care are not referred or are referred too late to take full advantage of such services.17–19
In 2007, the University HealthSystem Consortium (UHC), an association of 110 academic health centers, conducted the Palliative Care Benchmarking Project, a retrospective analysis of 44 hospitals measuring the percentage of inpatients seen by palliative care that the UHC considered “high risk,” 20 as defined below. The UHC audit showed that only 16% of patients at Massachusetts General Hospital (MGH) and 15% of patients at Brigham and Women's Hospital (BWH) who fell into the UHC-defined high-risk cohorts received a palliative care consultation—figures considerably lower than some institutions with similarly established palliative care services. Both hospitals also fell below the benchmark published in a 2008 consensus statement by the Center to Advance Palliative Care, identifying a target goal of 2.0 new referrals per staffed hospital bed per year for established programs in existence for 5 years or more 21 : in 2007, MGH saw 1.2 referrals per staffed hospital bed per year and BWH saw 1.0 referrals per staffed hospital bed per year. Consequently, palliative care leaders and hospital administration set a goal of improving access to palliative care services.
Partners HealthCare System, which includes MGH and BWH, joined with an insurer to select improved palliative care metrics as pay-for-performance quality improvement measures for the period 2007–2009. One of the performance measures chosen by MGH and BWH was the percent of patients seen by the hospital's palliative care service who, in retrospect, were identified as falling into a UHC high-risk cohort. Partially supported by an internal grant, the MGH and BWH palliative care programs collaborated with each other and their respective quality improvement offices to develop screening procedures that identified patients suitable for consultation.
Methods
Table 1 outlines the characteristics of the two hospitals, both of which are large urban academic medical centers. The Partners Institutional Review Board approved the study. The target population was patients who met the UHC criteria for high-risk patients, namely, inpatients over the age of 18 with a length of stay of 4 days or longer who either met: (1) acute cohort criteria—patients who had not been admitted to the hospital within the previous 12 months but died during the target hospitalization or (2) chronic cohort criteria—patients with 2 admissions in the previous 12 months for whom those admissions and the target admission were assigned 1 of 26 UHC-designated, high-risk diagnosis-related groups (DRGs),a regardless of whether the patient survived or died on the target admission. Although the insurer provided funds for the study, the patient population was not limited to the insurer's patients and could include patients with other or no insurance.
Excludes pediatrics, obstetrics, and psychiatry beds, as per CAPC guidelines
CAPC, Center to Advance Palliative Care; MGH, Massachusetts General Hospital; BWH, Brigham and Women's Hospital.
MGH's goal was to increase the consultation rate in this population from 16% to 23% while BWH's target was from 15% to 25%. The insurer withheld funds representing a material amount of dollars that were returned to the hospital if targets were met. The palliative care teams did not benefit directly from returned funds. For the purposes of the pay-for-performance audit, the measurement period was October 1 to December 31, 2009, compared to October 1 to December 31, 2007.
Screening procedures
Figure 1 outlines the general screening and identification protocols. Due to the distinctive hospital structures and cultures at MGH and BWH, as well as the unique characteristics of the two palliative care services, similar but different staffing and screening strategies were used at the two sites. The main difference was the use of an registered nurse or physician at MGH and a social worker at BWH, and a heavier reliance on initial computerized screening at MGH. Table 2 shows the staffing and resources available at the two sites.

Initial screening protocol for high-risk patients. *To minimize the risk of patients being discharged before being seen, computer screening of patients was performed on day 2 of admission. **At MGH, computer-based screening flagged patients whose medical records indicated a high risk of dying as evidenced by presence of key words in free text medical records indicative of serious illness, e.g., “critically ill,” “congestive heart failure.”
BWH staffing does not include Intensive Palliative Care Unit staffing.
MGH, Massachusetts General Hospital; BWH, Brigham and Women's Hospital; FTE, full-time Equivalent; LICSW, licensed clinical social worker.
Acute cohort
At MGH, patients were screened electronically by a medical record search engine, QPID. 22 QPID searched the records for potentially eligible patients using the above-mentioned UHC criteria, and also narrowed the list by searching for patients whose electronic medical records contained keywords indicating that the patient was seriously ill (e.g. “congestive heart failure,” “multiorgan failure,” or “critically ill”). This list of words was regularly revised as part of the Plan-Do-Check-Act process discussed below. Using both the UHC criteria and the keyword search QPID produced a daily list of 100–200 potential acute patients a day, roughly 30 of whom were newly admitted. A palliative care registered nurse/physician would screen the electronic record of the new patients, and also review records of those patients still in the hospital on days 7, 10, 14, 21, and 31 of their admission. The paper records of those patients identified as high risk for dying were also reviewed. The study nurse also made regular visits to cardiac floors to provide ongoing informal palliative education to nursing staff as well as to further discuss potential study patients.
At BWH, the study team selectively targeted intensive care unit (ICU) patients and patients with long length of stay (>14 days); these patients were screened weekly. In addition, the study social worker or physician made daily visits to the ICU and cardiac floors to ask nursing staff about potential referrals. Finally, the study social worker developed a significant source of referrals from an informal network of social workers, nurses, chaplains, and care coordinators who identified high-risk patients.
Chronic cohort
Computer programs at both institutions identified patients admitted to the hospital twice within the preceding 12 months and who had been discharged with the UHC-designated high risk DRGs. The most common DRGs that triggered consults were: heart failure and shock; respiratory infections and inflammations with complications; and chronic obstructive pulmonary disease. Typically, the teams at both hospitals were alerted to 2–10 potential chronic patients per day. Informal referrals from floor staff resulting from an increased presence on wards, also contributed to additional potentially suitable patients.
Approval by attending
After a study team member reviewed the patient's electronic and paper records and deemed the patient likely to be suitable for a palliative care consultation, the inpatient attending was contacted and informed that the patient had been identified as a high-risk patient and potentially suitable for a referral. At MGH, attendings were contacted via email from a member of the study team. At BWH, the social worker would make contact either in person or via email. Patients were only seen if the attending agreed that a consultation would be appropriate. However, at BWH, medical intensive care unit and hospitalist leadership granted blanket approval for referrals.
Patient consultation
At MGH, all patients were seen by palliative care clinicians and a full consultation was performed; these consults were termed “Supportive Care” rather than palliative care, a term preferred by the program's advisory group. 23 At BWH, acute patients were seen by the inpatient team; chronic patients were seen by a social worker who completed the consult and referred to the inpatient palliative care team only if patients had uncontrolled symptoms. At BWH, the term “Supportive Care” consultation was used for cardiology patients only.
Plan-Do-Check-Act cycle
The intervention was a quality improvement project that employed a traditional Plan-Do-Check-Act cycle, an iterative four-step process that allows for continuous incremental changes each cycle. 24 An essential part of the planning process involved getting early input and strong support from the leadership of both hospitals. The chief medical officers and the quality and safety units at both hospitals were intimately involved with the project and invested in its success. Buy-in from the hospital administration was critical in gaining access to hospital departments, particularly those less familiar with or supportive of palliative care. Early planning for the project also included establishing clinical advisory boards, engaging clinicians likely to care for target patients, and establishing buy-in from the palliative care teams.
The quality improvement cycle of Plan-Do-Check-Act enabled teams to respond quickly to problems that arose. Although outcomes were only formally measured quarterly, both project teams initially met on a weekly basis to review the accuracy and reliability of the screening procedures, discuss progress, and identify problems and possible solutions, thus allowing for continual and timely improvement. Serial changes were made to the electronic screening tools at both hospitals. At MGH, for instance, where initial screening protocols for the acute cohort proved to be labor intensive with relatively low yield, the screening criteria were refined significantly to increase accuracy. Advice was sought from clinicians who had been contacted about referrals and different methods of contacting physicians were trialed in an effort to decrease the non-response rate. Feedback from members of the palliative care teams regarding the appropriateness of consults for the screened patients was also continually elicited.
As familiarity developed between the palliative care services and other hospital units, and as personal relationships strengthened, collaboration improved such that clinicians would proactively identify potential patients for the project. At MGH, the research team's strong relationships with medical intensive care units (MICU) and cardiology were particularly helpful in identifying high-risk patients, and there was a shift away from relying solely on the computer-generated lists. BWH began with intensive outreach to the MICU and cardiology as well as developing an informal network for identifying patients at high risk of death; these relationships and networks expanded over the course of the project.
The palliative care services also recognized that certain teams or referring physicians routinely refused a suggested consultation, and during the intervention, limited resources were directed to more fertile fields.
Results
At MGH, in the final quarter of 2009, the Palliative Care Service consulted on 46% of the patients in the target cohorts, compared to 16% in the final quarter of 2007. At BWH, 47% of the target patients were seen compared to 15% two years previously (Fig. 2 and Table 3). These rates were well above the pay-for-performance targets of 23% and 25% for MGH and BWH respectively. In addition to the increase in the target cohorts, overall consult volumes increased at both hospitals (Table 4).
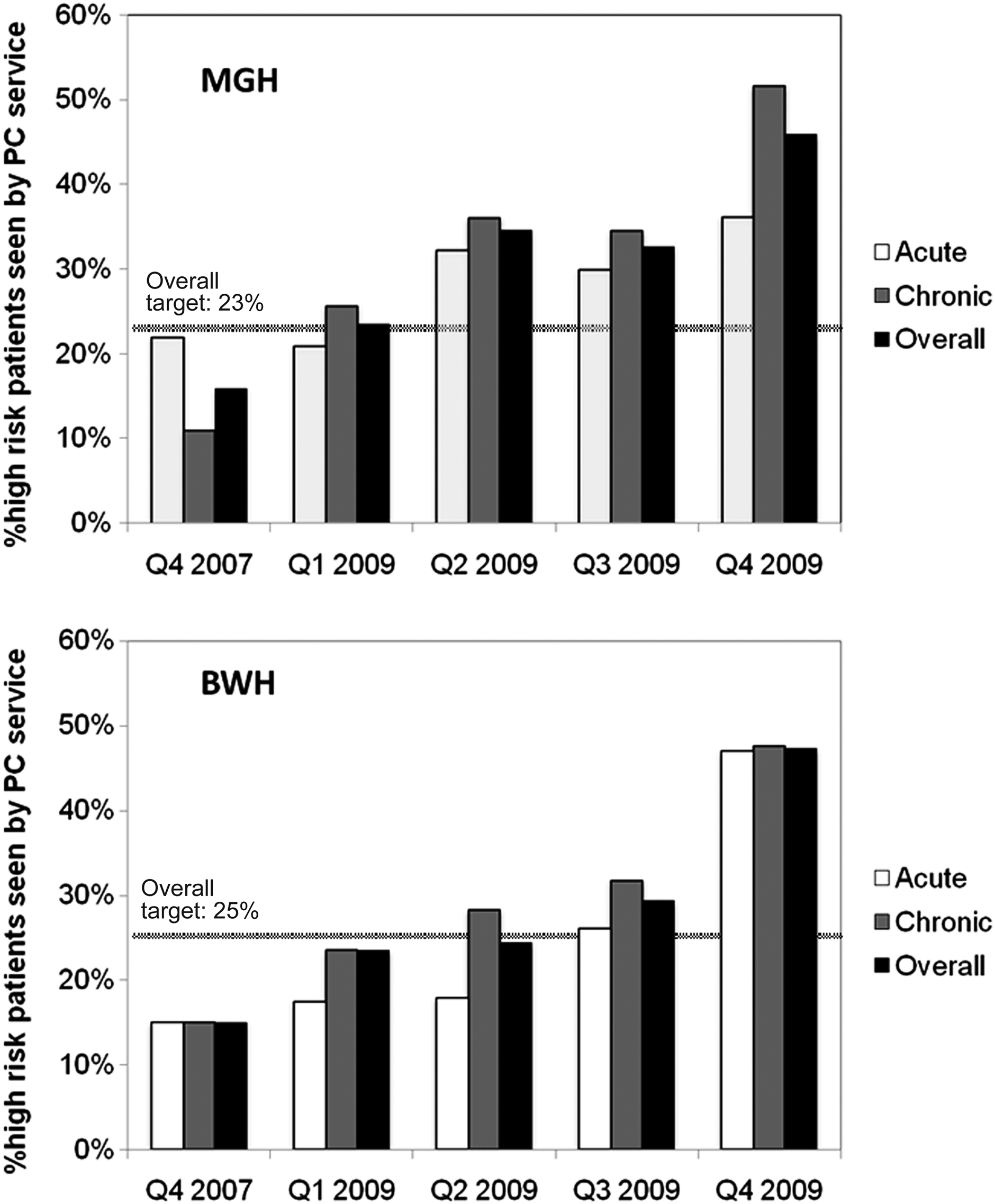
High-risk patients seen by the Palliative Care Service.
The insurer retrospectively provided the hospitals with a list of the patients who fell within the acute and chronic criteria at the end of each quarter.
Given BWH informal referral system, identifying which patients were seen through the QI effort and which came through regular referral channels was not always clear.
These patients were not seen either because they were never identified by the screening protocols, or they were identified but the treating team did not require a palliative care consult.
MGH, Massachusetts General Hospital; BWH, Brigham and Women's Hospital; UHC, University Health System Consortium.
Number of palliative care consults per staffed hospital bed (excludes pediatrics, obstetrics, and psychiatry beds, as per CAPC guidelines) per year.
MGH, Massachusetts General Hospital; CAPC, Center to Advance Palliative Care; BWH, Brigham and Women's Hospital.
At MGH, 51% of e-mail requests resulted in a consult. For those that did not result in a consult, 68% did not respond to the e-mail, while 32% wrote back and declined a consult. While the majority of the rejection e-mails did not provide a reason, common responses were that the attending did not feel that palliative care was appropriate at the time of request or that the patient was being discharged that day.
At BWH, the nonresponse/refusal rate was 23%. Two reasons may have contributed to BWH's lower rate: (1) more of the consults were requested in person by the social worker and (2) the medical ICU and hospitalist leadership had granted blanket permission for their patients to be seen by the service.
Discussion
In this initiative, a quality improvement effort that involved screening records and offering consults proved an effective strategy for expanding access to palliative care in a targeted population of high-risk patients. Consultations in this retrospectively defined, high-risk population tripled at both hospitals over a 3-year period, with overall referral rates increased significantly, most dramatically among nononcology patients.
The opportunity for this quality improvement project was provided by the participation in a pay-for-performance initiative and the choice of palliative care metrics as the key measure. Pay-for-performance programs that link financial payments with achievement of high quality care are increasingly being utilized in health care in an effort to improve patient outcomes as well as encourage appropriate resource utilization.23,25–28
Factors contributing to increased consultation rates
Each of the stakeholders in the pay-for-performance initiative was motivated to participate. For the insurer, previous studies reporting palliative care consultations leading to improved care and cost savings drew attention. For the hospital administration, the most important motivator was “doing the right thing” and improving patient care for those suitable for palliative care, with additional hopes of reducing inappropriate resource utilization. Commitment from hospital leadership ensured sufficient financial backing, including resources for significant information technology support that was necessary to successfully carry out a project of this scope. Supported time from the developers of QPID allowed us to experiment with and create a user-friendly computer-based screening tool that facilitates identification of a variety of patient populations. For the referring clinicians, improved care for patients and potentially decreased workload for themselves were thought to be prime factors.
Benefits to the palliative care services
For both services, motivators included increased visibility and hospital-supported outreach as well as improving end-of-life care for patients. The project was responsible for a number of positive outcomes. Teams were involved earlier in admissions and could have significant impact by attending to the patient's symptoms and the psychosocial needs of both the patients and their families. There were opportunities to access new patient populations. For instance, new patients identified from the acute cohort were often transferred from outside hospitals with complex diseases, high symptom burden, and a need for intensive medical intervention, but this set of patients were usually not referred to the palliative care or were consulted in the very last hours of life. The project also enabled the services to increase contact with units that did not usually utilize palliative care. There were many opportunities to further educate other providers about the management of end-of-life symptoms, psychosocial support, and communication about end-of-life issues. The use of QPID at MGH introduced the palliative care team to a valuable methodology for identifying patients for other projects. At BWH, another important outcome was an increased appreciation of the ability of nonpalliative care social workers to accurately identify patients appropriate for consultation.
The overall consult volume increased significantly for both services from 2005 to 2009. While some of this growth is accounted for by the quality improvement project, we believe that much it was a consequence of the services having higher visibility during the project, both from the increased contact with individual physicians solicited because of the project and increased outreach efforts. In 2010, a year after the intervention was completed, consult volumes declined by 30% in nononcology populations at MGH and by 50% at BWH.
The profile of the palliative care services at the higher levels of hospital management was also significantly raised. Partners HealthCare System deepened its commitment to palliative care, providing support for a leadership retreat as well as a palliative care strategic plan. Subsequently, both services have been expanded throughout the network, have received funding for additional staff and increased resources for palliative care education. As a direct result of the project, both hospitals are now involved in projects working on increasing awareness of the relevance and utility of palliative care for end-stage heart failure patients. Most importantly, a gradual culture change occurred; palliative care grew to be viewed as a standard facet of good medical care for patients with life-limiting illnesses, particularly in the units where efforts were concentrated.
Challenges
Both palliative care teams faced challenges during this project. In targeting the acute patients, patients at risk for death in the hospital, often in their final days, were targeted. Some felt that we were undermining our message of “consult us early.” The costs required to support clinical and administrative study staff were not insubstantial. There have been arguments in the literature that money used to administer pay-for-performance projects may be better used to directly benefit patient care. 25 In this project, developing a database to consistently and accurately identify suitable patients was resource and time-intensive. At MGH, despite significant changes, QPID still identified a high number of patients clearly not suitable for a palliative care consultation, which required additional screening by the registered nurse/physician.
Screening for the UHC cohorts sometimes identified patients for whom the reason for consultation was nebulous or who gained marginal benefit from the consult. When the census was high, some of the staff felt that they were devoting too much effort to reaching the quality improvement goal rather than focusing on more needy patients and families. At times, this significantly impacted upon staff morale. 26 One solution was to develop new models for caring for the study population, particularly those in the chronic cohort. For example, although the initial plan at MGH was that all study patients would receive a full palliative care consultation, for those in the chronic cohort without uncontrolled symptoms but more in need of psychosocial support, patients were seen less frequently (e.g., three times a week rather than daily).
Limitations
This study had several limitations. The two hospitals are major medical centers with mature palliative care services, and thus generalizability may be limited for other types of sites and programs. We measured consultation rates, but are aware that pay-for-performance programs that are associated with improvements in such process of care measures have had less of an impact on patient outcomes or efficiency of care.22,25,27–30 Unfortunately, limited resources prevented us from obtaining data on secondary outcomes such as length of stay, readmission rates, use of intensive care, hospital costs, hospice referrals, or family satisfaction, so we cannot claim that patient care was improved or that there was a more efficient use of scarce resources. Finally, the particularities of the measured outcome—consultation on a select group of high-risk patients, as determined retrospectively by UHC criteria—limit the applicability of the results to other defined populations.
Conclusion
This quality improvement initiative was successful in increasing access to palliative care services in high-risk populations, especially non-oncology patients. Effective screening and identification methods were developed, and the pay-for-performance initiative appeared to motivate clinicians to engage with the palliative care team.
Footnotes
Acknowledgments
The MGH team acknowledges the diligent efforts of Mitchell Harris PhD and Michael Zalis MD with QPID. BWH team thanks Suzanne McHale, Susan Wante and the Center of Clinical Excellence staff for their enthusiastic support.
Author Disclosure Statement
No competing financial interests exist.
| 1. | DRG 010 | Nervous system neoplasms with complications |
| 2. | DRG 014 | Specific cerebrovascular disorders except transient ischemic attack |
| 3. | DRG 079 | Respiratory infections and inflammations, age >17 with complications |
| 4. | DRG 082 | Respiratory neoplasms |
| 5. | DRG 088 | Chronic obstructive pulmonary disease |
| 6. | DRG 089 | Simple pneumonia and pleurisy, age >17 with complications |
| 7. | DRG 092 | Interstitial lung disease with complications |
| 8. | DRG 127 | Heart failure and shock |
| 9. | DRG 144 | Other circulatory system diagnosis with complications |
| 10. | DRG 172 | Digestive malignancy with complications |
| 11. | DRG 174 | Gastrointestinal hemorrhage with complications |
| 12. | DRG 202 | Cirrhosis and alcoholic hepatitis |
| 13. | DRG 203 | Malignancy of hepatobiliary system or pancreas |
| 14. | DRG 205 | Disorders of the liver except malignancy, cirrhosis and alcoholic hepatitis with complications |
| 15. | DRG 239 | Pathologic fractures and musculoskeletal and connective tissue malignancy |
| 16. | DRG 296 | Nutritional and miscellaneous metabolic disorders, age >17 with complications |
| 17. | DRG 316 | Renal failure |
| 18. | DRG 395 | Red blood cell disorders, age >17 |
| 19. | DRG 398 | Reticuloendothelial and immunity disorders with complications |
| 20. | DRG 403 | Lymphoma and non-acute leukemia with complications |
| 21. | DRG 416 | Septicemia, age >17 |
| 22. | DRG 423 | Other infectious and parasitic disease diagnoses |
| 23. | DRG 473 | Acute leukemia without major OR procedure, age >17 |
| 24. | DRG 475 | Respiratory system diagnosis with ventilator support |
| 25. | DRG 489 | HIV with major related condition |
| 26. | DRG 492 | Chemotherapy with acute leukemia as secondary diagnosis |