
Abstract
Abstract
Background:
Increasing demand for palliative care unit (PCU) beds has led to shorter inpatient stays and a requirement to transfer some patients from a PCU to a residential aged care facility (RACF). Concerns have been raised regarding this move with suggestion that patients often die shortly after transfer. Published data investigating this patient group are limited. The aim of the current study was to audit discharges from a PCU to RACFs specifically looking at predictive factors for survival following discharge.
Methods:
A retrospective audit was undertaken of all discharges from the Barwon Health PCU to RACFs between July 2007 and July 2010. Data on patient demographics, clinical and functional status, admission and discharge details, and survival times were examined. Factors influencing survival were evaluated by Cox proportional-hazards regression analysis.
Results:
Sixty-two discharges from a PCU to an RACF were included in the analysis. The mean age at discharge was 76 and the majority of patients had malignant disease. Mean and median survival times post-transfer were 106 and 42.5 days, respectively, and 16% of subjects survived more than 100 days. From univariate analyses age, PCU length of stay, admission Resource Utilization Groups–Activities of Daily Living (RUG-ADL) score, dependent mobility, having lung cancer or cancer of unknown primary, and living alone or in an RACF pre PCU admission affected survival. Multivariate analyses showed age, PCU length of stay, RUG-ADL score, and living situation prior to PCU admission together were associated with postdischarge survival times.
Conclusions:
This study is one of the largest investigating this cohort and suggests a number of factors that may predict survival for patients after discharge from a PCU to an RACF.
Introduction
In North America the last decade has seen the development of acute palliative care units (APCU). Interdisciplinary and typically located within tertiary cancer care centers, they have a focus on rapid symptom stabilization, comprehensive psychosocial care, and timely discharge planning.10–14 Distinction is made between an APCU and the more traditional PCU/hospice on a number of levels including shorter lengths of stay (typically days to 2 weeks), lower inpatient mortality (most <50%), and an academic mandate for education and research. In Australia although most PCUs continue to provide both short and where necessary longer-term care, this occurs within the context of increasing admission requests 3 and consequent pressure to avoid protracted lengths of stay.
An outcome of the move away from longer-term inpatient palliative care is the relocation of patients whose condition stabilizes but who are not able to go home.2,15 In the Australian context these individuals would be considered for transfer to a residential aged care facility (RACF) offering high-level (nursing home) or low-level (hostel) care, as the options for long-term hospice-based accommodation are limited. For the years 2001 and 2002 approximately 12% of live palliative care hospital separations in Australia were to an RACF. 16
A small number of predominantly retrospective studies have addressed transfer from a PCU to an RACF. The majority have involved small sample sizes and most have emphasised the potential problems for patients, their families, and staff.5–8,15 Reith and Lucas, 15 in an audit of patients considered for relocation from hospice to a nursing home, reported that although transfer was considered in 6.9% of admitted patients, only 6 of a total of 347 were actually transferred. In those who were relocated high levels of distress and dissatisfaction were reported by patients and their families. In another study 6 of 10 relatives of patients discharged from a PCU to nursing homes reported the move as unsatisfactory, resulting in additional distress during an already traumatic period. 6
Porock and colleagues 2 in a review of relocation stress suggested a critical 3-month period of increased vulnerability following admission to a nursing home, although this was not specific to palliative patients. The authors noted that evidence addressing experiences around transfer from a PCU to an RACF was scarce but postulated that the unpredictable prognosis associated with a terminal illness may lead to a survival time shorter than that required to adequately adjust to the new environment. This concept of a crisis period after transfer is not uniformly supported. Enes and coworkers 5 noted there was limited research supporting the idea and that the evidence for relocation stress was inconsistent. The authors did agree with Porock et al. 2 that little is known about the experiences of patients discharged from a PCU to an RACF.
Some have suggested that patients from PCUs often die a short time after admission to a nursing home, 8 with one study finding that five of six patients died within 15 days of transfer. 15 A retrospective review of 16 patients discharged from hospice to a nursing home found a mean length of stay after transfer of just over 8 weeks, although 38% of patients died within 3 weeks of relocation. 5 More recently, a large review of outcomes for 2568 patients with advanced cancer admitted to an APCU reported that transfers to a long-term care facility made up only 2% of patients discharged alive, and that this group had a median survival of 29 days (14–44; 95% confidence interval [CI]). 10
Data investigating predictors of survival for anyone admitted into an aged care facility are limited. 17 A recent longitudinal study of 2206 admissions to Icelandic nursing homes reported significant predictors of survival included age, health stability, and activities of daily living (ADL) functioning. 17 Whereas many studies have analysed prognostic factors in palliative patients,14,18–25 few have investigated predictors of shortened survival for those required to be discharged from a PCU to an RACF. Lau et al., 25 in an unpublished retrospective audit of PCU separations over a 3-month period, investigated the addition of the Palliative Prognostic Score (PaP) to clinical predictive survival during discharge planning. In the study 16 patients were considered for nursing home placement and nine were subsequently placed. The authors concluded that the addition of the PaP improved clinical predictive survival and was of assistance in discharge planning. Garrard and Cleasby 26 in a New South Wales Health Palliative Care Advisory Group agenda item recommended that the decision to transfer between a PCU and an RACF be predicated on a number of factors including prognosis, potential future symptoms, and the possible impact on the patient and the family. They advocated the use of a validated prognostic tool to help make this decision.
The aim of the current study was to audit discharges from a PCU to RACFs. Specifically, this research aimed to investigate clinically relevant factors influencing length of survival following transfer. This is important information as it has the potential to allow improved patient stratification to the PCU to RACF discharge pathway.
Methods
Setting
Barwon Health is a comprehensive Victorian regional health service, centered on the provincial city of Geelong and servicing a primary catchment of between 350,000 and 500,000 people. 27 The Barwon Health PCU is a 16-bed facility offering palliative care to patients with malignant and nonmalignant pathologies. Staffed by a multidisciplinary team of doctors, nurses, social workers, pharmacists, physiotherapists, occupational therapists, speech pathologists, dietitians, psychologists, volunteers, and pastoral care workers, the unit aims to provide high-quality patient- and family-oriented care. The PCU accepts admissions from hospitals (including private facilities), RACFs, and the community. There are approximately 30 admissions per month, median length of stay is 14 days, and there is invariably a waiting list of patients requiring admission.
Subjects/data collection
This retrospective audit examined all discharges from the PCU to an RACF between July 2007 and July 2010. Using December 31, 2010 as a cut-off date for analysis, data were collected on patient demographics, primary diagnosis, Charlson comorbidity score28,29 and number of comorbidities, presence of metastatic disease, location prior to and length of PCU stay, Edmonton Symptom Assessment System (ESAS) score and mobility status on admission, Resource Utilization Groups–Activities of Daily Living (RUG-ADL) scores on admission and discharge, and date of death. Information was accessed from Barwon Health institutional databases, medical record review, and the Victorian Registry of Births, Deaths and Marriages.
For patients with more than one malignancy or those with a combination of nonmalignant and malignant pathologies, the disease process principally responsible for admission was recorded as the primary diagnosis. Both high-level and low-level care facilities were considered RACFs. The review received approval from the Barwon Health Human Research Ethics Committee.
Analysis
Of the 65 patients discharged from the PCU to an RACF, three were discharged on two separate occasions. To maintain independence among subjects only the first of these transfers per patient was included for analysis. Survival time was calculated by subtracting day of death from PCU discharge date. Patients alive at study completion (December 31, 2010) were censored to that date.
Descriptive statistics were used to summarize demographic data. Overall cumulative survival was plotted on a Kaplan-Meier curve. Univariate Cox proportional-hazards regression was used to investigate factors impacting upon survival after discharge from a PCU to an RACF. From this, factors with a p value < 0.4 were analysed together using Cox regression with backward stepwise selection method to identify variables associated with shortened survival times. Factors with p values > 0.10 were removed from the model in a stepwise manner until only those with a p value of < 0.10 remained. Analysis was performed using the Statistical Package for Social Sciences (SPSS versions 11.5 and 18; SPSS, Inc., Chicago, IL).
Results
Between July 2007 and July 2010, there were 945 separations (including deaths) from the PCU. Sixty-five (7%) of these discharges were to an RACF with the majority of patients (95%) requiring high-level care. The patient characteristics of the 62 analysed RACF discharges are shown in Table 1. The mean age at discharge was 76 years (39 to 92 years), the mean length of PCU stay 31 days (range 1–104 days), and 13% of primary diagnoses were nonmalignant. Urological, lung, and colorectal were the most common malignancy types. The majority of subjects (82%) were living at home prior to PCU admission and approximately one-third were admitted to the PCU from another hospital. More than half of the patients were dependent regarding mobility upon admission.
Includes prostate, renal, and bladder carcinoma.
Includes bone and soft tissue, gynecological, breast, and skin malignancies.
Includes pancreatic, gastric, esphageal, and liver malignancies.
CNS, central nervous system; GIT, gastrointestinal tract; PCU, palliative care unit; RACF, residential aged care facility; RUG-ADL, Resource Utilization Groups–Activities of Daily Living.
Figure 1 shows the cumulative survival curve for the 62 analysed patients. The median and mean survival times for patients discharged from a PCU to an RACF were 42.5 and 101.2 day (range 3–801 days), respectively. Three (5%) patients were alive at the time of analysis, and 16% of discharged patients survived ≥100 days post-transfer. Comparison of median survival times between primary diagnoses is displayed in Figure 2. The majority of discharged subjects with lung cancer and cancer of unknown primary died ≤28 days from discharge, whereas patients with central nervous system (CNS) and head and neck malignancies each had median survival times of > 80 days.
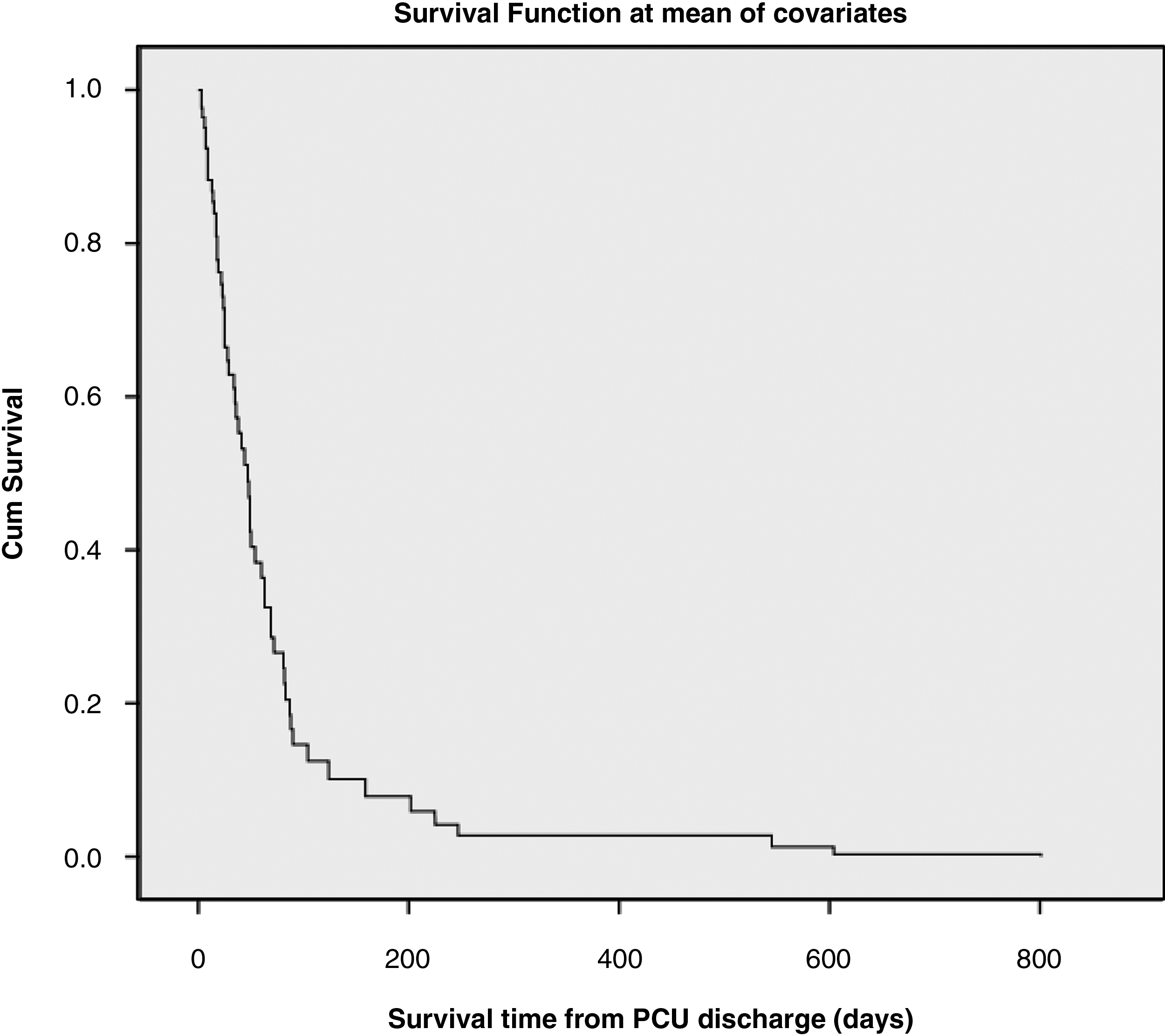
Graph of cumulative survival after discharge from a PCU to an RACF (62 subjects).
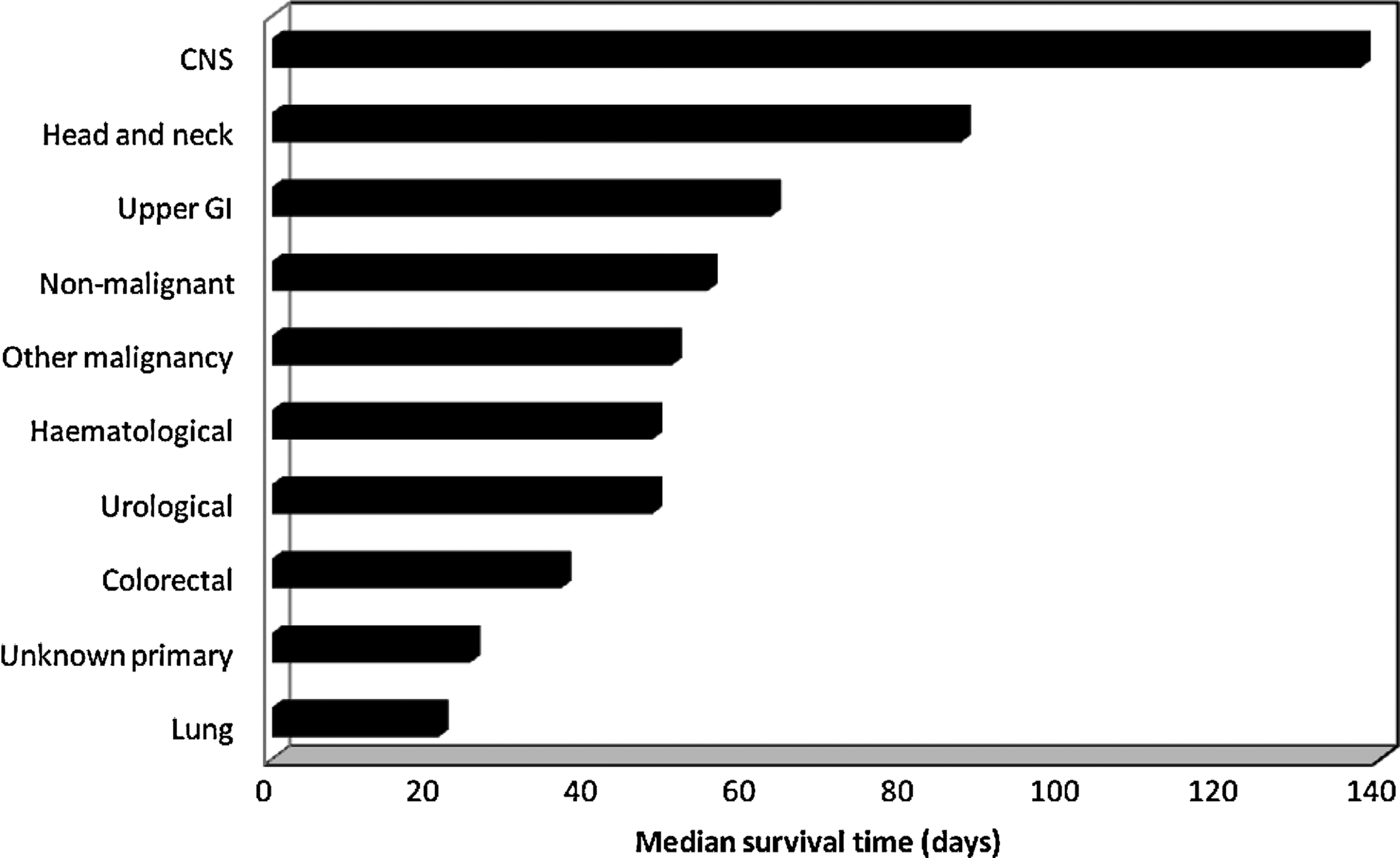
Graph comparing median survival times between primary pathologies.
Factors impacting survival times from univariate analyses are shown in Table 2. Shorter survival was associated with increasing age (p=0.021), briefer PCU length of stay (p=0.007), higher admission RUG-ADL score (p=0.005), dependent mobility (p=0.052), a diagnosis of lung cancer or malignancy of unknown origin (p=0.029), and either living alone or residing in an RACF prior to PCU admission (p=0.021).
PCU, palliative care unit; RACF, residential aged care facility; RUG-ADL, Resource Utilization Groups–Activities of Daily Living.
The results of the multivariate analysis are shown in Table 3. Increased age, shorter length of PCU stay, higher RUG-ADL score, and living alone or in a RACF prior to admission together were associated with reduced survival times after discharge from a PCU to an RACF.
PCU, palliative care unit; RACF, residential aged care facility; RUG-ADL, Resource Utilization Groups–Activities of Daily Living.
Discussion
Seven percent of total separations from the PCU were to an RACF and this is a greater proportion than previously reported.15,30 Several factors may have influenced this finding including the availability of nursing home beds in the region and the increasing demand for inpatient palliative care beds. 3 It is unlikely the difference was due to limitations in home-based community supports as the Barwon region is well served by such services.
The median survival time in this study was just over 6 weeks with 16% of subjects surviving ≥100 days. This does not support previous findings that patients often die shortly after transfer to an RACF.8,15 and may reflect both the larger sample size in the current study and expected differences across health care systems. The overall median survival of 42.5 days was comparable to that found by Lau and colleagues, 25 who reported a figure of 55 days in nine patients transferred from an Australian PCU to an RACF. Although there is no consensus as to an acceptable survival time in an RACF after discharge from a PCU, a minimum predicted period has been proposed as a requirement for consideration of RACF transfer. Reith and Lucas 15 suggested this should be 4 weeks, a time frame also advocated by a number of Australian PCUs. 31
The length of PCU stay for patients discharged to an RACF was considerably longer than the average for all separations. This is largely explained by the organizational processes required to facilitate RACF placement, which can take some time. For patients discharged to an RACF, longer PCU stays were significantly associated with prolonged survival. There are a number of potential explanations for this finding. It is likely that length of stay varied in part due to heterogeneous primary pathologies. Some patients with a better prognostic disease process may have experienced acute issues necessitating a longer stay. Once stabilized, their underlying primary pathology would continue to confer a better prognosis and therefore they would still be expected to have a prolonged comparative survival upon discharge. Some subjects may have required a lengthier stay due to complex medical, psychosocial, or emotional care needs. A prolonged stay would allow optimal management of these issues and in turn contribute to longer survival after transfer. The finding of association between longer PCU admission and improved postdischarge survival supports the use of an observation period after PCU admission prior to the establishment of discharge plans. This approach is used by numerous palliative care institutions, 31 including the one in the current study.
Poorer prognosis pathologies such as lung cancer and cancer of unknown primary had the shortest median survival times and were significantly associated with reduced survival in the univariate analyses. This is important as it suggests extra prudence is required when patients with these pathologies are being considered for discharge to an RACF. Conversely, a number of pathologies had median survival times of > 50 days and this information may allow increased confidence in the appropriateness of RACF-based discharge plans for these patient groups.
Increasing age was significantly associated with reduced survival after RACF transfer in the present study. This is in keeping with data investigating predictive survival factors for any patient admitted into residential care 17 but varies from that analysing prognosis in palliative patients. In the latter group age has generally been considered independent of survival time,18,21 although two recent studies14,21 in PCU settings have reported a significant relationship between younger age and worse prognosis. In a prospective analysis of patients in a Hong Kong PCU younger age was an independent prognosticator for reduced survival 21 and in a later North American study 14 was found to be significantly associated with inpatient APCU mortality. The patients in these studies were younger than those in the current one, and therefore comparison is difficult. It might be postulated that by demonstrating the clinical stability necessary for transfer from a PCU to an RACF, patients in the current study become more characteristic of the general population being considered for residential care and less like a clinically unstable PCU patient. In this way it would be anticipated that increasing age was predictive of shorter survival after discharge.
Impaired functional ability determined by a higher RUG-ADL score was significantly associated with reduced survival. This score represents a patient's ability to perform a range of ADL, with higher numbers indicating more impaired function. ADL scores have previously been shown to be predictors of poor prognosis in palliative patients 32 but have not been as extensively investigated as performance status measures such as the Karnofsky Performance Scale. 18 Dependent mobility represents a simple, practical indicator of reduced functional capacity and in the univariate analyses impacted upon survival time after discharge from a PCU to an RACF. This finding mirrors that of Twomey et al. 22 who found independent mobility to be a predictor of length of survival, with nonindependent patients at PCU admission being less than half as likely to survive as long as those able to mobilize on their own.
One potential influence on survival, which was not considered in the current study, is the availability of ongoing support once RACF transfer has occurred. It is conceivable that those discharged to facilities with less staff expertise in palliative management and/or less access to specialist palliative care services may be at risk of shortened survival. Although the majority of discharges in this study went to local RACFs routinely supported by the Barwon Health community palliative care service, the efficacy of this care transition was not specifically assessed. The possible impact of variations in palliative care support across RACFs should be considered in future research into this population.
There are other limitations associated with this research. The retrospective nature meant only data routinely collected upon PCU admission and/or available from Barwon Health sources could be analysed. Consequently, several potentially important factors including a prognostic or performance score, socioeconomic information, and pathology results could not be assessed. It had been planned to include symptom severity using ESAS scores in the analysis, but this was not possible due to inconsistent recording of patient scores. The sample in this study was drawn from a single PCU in regional Australia and thus the results may not be generalizable to a wider palliative population. It included only quantitative data on PCU to RACF transfers, and therefore important qualitative information emphasized by previous authors,2,5,6,8,15 such as patient and family satisfaction, was not able to be evaluated.
A number of areas for future research are suggested. The effect of primary diagnoses and factors such as age, function, and performance status upon survival after discharge from a PCU to an RACF warrants further clarification as this patient group will continue to grow. The physical, emotional, and psychosocial effects of the transfer upon patients and their families need also to be considered. A prospective, multicenter study incorporating a palliative prognostic scale and a qualitative assessment may provide the best method of achieving these aims.
This study of 62 discharges from a PCU to an RACF is one of the largest investigating this patient group and one of the first to address factors associated with shortened survival post-transfer. Summarized in Table 4, this information is important as it has the potential to advance PCU admission and discharge planning approaches, to improve bed allocation and assist staff, patients, and their families in the making of difficult decisions.
Unless patient's usual place of residence is an RACF and the plan is to transfer him or her back to facility for terminal care.
Footnotes
Acknowledgments
The authors would like to thank Ms. Kim Butler for assistance with data collection, Ms. Julie Garrard for information and advice, Dr. Linda Klein for statistical assistance, and Ms. Jo Sheedy for statistical advice and manuscript review.
Author Disclosure Statement
No competing financial interests exist.