
Abstract
Abstract
Background:
The literature has described the use of ketamine as an adjuvant treatment for opioid-refractory cancer pain. None of these studies have used the drug in a palliative care patient population.
Aims:
The primary objective of the study was to assess the efficacy of continuous intravenous infusion of ketamine in patients suffering from cancer pain refractory to opiates who had been admitted to palliative care units. Secondary objectives were to assess patients' satisfaction with and tolerance of ketamine.
Methods:
A randomized, double-blind, placebo-controlled study was designed, and the study setting included seven French adult palliative care units. Inclusion criteria were age ≥18 years, and cancer pain refractory to standard opiates. Evaluations were conducted at randomization (baseline), at ketamine or placebo introduction time (T0), and at 2 hours (T1), 24 hours (T2), and 48 hours (T3) after T0. The primary evaluation criterion was pain efficacy assessed using a patient self-rated Numeric Pain Intensity Scale (NPIS) at T1. The main secondary evaluation criteria were daily morphine dose, symptom evaluation (Edmonton Symptom Assessment Scale [ESAS]), and patient satisfaction (Pain Treatment Satisfaction Scale [PTSS]).
Results:
Twenty patients were analyzed (11 received ketamine and 9 received placebo). Self-reported pain did not differ between the two groups, as the symptoms continued to evolve during the study period. The tolerance for ketamine was satisfactory.
Conclusion:
The present study did not confirm the efficacy of the ketamine-morphine combination in refractory cancer pain. The results suggest that specific populations could be “good responders” for this therapeutic approach. Further studies should be performed that take into account the difficulties of conducting clinical research in the palliative care context.
Introduction
Since 1999, the French government has tried to widen the availability of palliative care using ambitious national programs. Palliative care, in accordance with the French Accompaniment and Palliative Care Society (SFAP), is now clearly defined as a global approach to the person affected by a serious illness that is becoming progressively worse or a patient at the end of life. 19 One of the aims of the various development plans has been to develop and strengthen palliative care research. This prompted us to set up a prospective, randomized, double-blind, placebo-controlled trial where the main objective was to assess the efficacy of continuous intravenous infusion of ketamine in patients in palliative care units suffering from cancer pain refractory to opiates. The secondary aim was to assess both tolerance and patients' satisfaction with this therapeutic approach.
Materials and Methods
Patient eligibility
Eligible patients included those suffering from cancer pain, receiving palliative care as defined by the World Health Organization (WHO): “Palliative care is provided to patients with an incurable disease and includes control of pain, control of other symptoms, and psychological aspects. The goal of palliative care is achievement of the best possible quality of life for patients and their families.” 20 The main inclusion criteria were age ≥18 years, cancer pain refractory to standard opiates regardless of the nature of the primary cancer (Numeric Pain Intensity Scale [NPIS] score ≥4/10 after 24 hours of continuous intravenous morphine administration), histological diagnosis of cancer with locally advanced or metastatic disease, with or without palliative anticancer treatment, and hospitalization in a specific palliative care unit. The exclusion criteria were contraindication to the use of ketamine, a sleepiness score higher than 16 on the Epworth Slumber Scale, 21 and WHO performance status >3. All patients provided written informed consent for participation. The study was approved by the local ethics committee (Comité de Protection des Personnes Sud-Méditerranée, France) and the French drug and device regulation agency, Agence française de sécurité sanitaire des produits de santé (AFSSAPS).
Study design
This randomized, double-blind, placebo-controlled study was performed in seven adult palliative care units localized in the South of France. The flow chart of the study is shown in Figure 1. A computer-generated randomized list was drawn up using a permuted block design. The experimental group was given a combination of ketamine and morphine, whereas the control group was given a combination of placebo and morphine. Inclusion and randomization were performed after a minimum duration of 24 hours of intravenous morphine.
Flow chart.
Control group
Morphine chlorhydrate was administered intravenously to standardize the therapeutic protocol and for quicker speed of action. For patients already taking oral opiates, the intravenous dose for 24 hours was equal to a third of the oral dose. For patients without initial oral opiate treatment, the loading dose was 1 mg/kg per day, except for in the setting of renal insufficiency or among the elderly, in which case the dose was 0.25 to 0.5 mg/kg per day. There was no maximum dose, as long as side effects could be controlled. Morphine treatment was carried out according to WHO recommendations. 20 Daily morphine dose could be increased daily by 50% if necessary. Morphine interdoses were planned with one-tenth of the daily dose. The interval between interdoses was fixed to one hour. A saline solution was administered intravenously and was continuous throughout the study period.
Experimental group
Morphine treatment was the same as that in the control group. Ketamine was administered intravenously and was continuous throughout the study period. Boluses were not administered to decrease the risk of neuropsychic effects. 15 The initial dosage was 0.5 mg/kg per day then 1 mg/kg per day after 24 hours if the NPIS score remained ≥1.
No other opioids were added during the study period. Evaluations were performed at five different time points: at randomization (baseline), at ketamine or placebo introduction time (T0), and at 2 hours (T1), 24 hours (T2), and 48 hours (T3) after treatment initiation.
Evaluation criteria
Primary evaluation criterion
The primary evaluation criterion was the change of pain level between baseline and T1 (2 hours after baseline evaluation). Pain levels were assessed using a patient self-administered NPIS. The instrument ranged from 0 (no pain) to 10 (worst pain possible).22,23 The numeric scale is largely used to assess pain level and has satisfactory properties. 24
Secondary evaluation criteria
The efficacy of pain management was conducted using the following scales: (1) change of pain level between baseline and T2, baseline and T3, and daily morphine dose during the 48-hour study period; (2) symptom evaluation as assessed using the Edmonton Symptom Assessment Scale (ESAS) at T2 and T3. The ESAS was developed for use in assessing the symptoms of patients receiving palliative care and has received much interest as a bedside clinical instrument, 25 as it allows for a multidimensional evaluation of pain using a nine-item patient-rated symptom scale. These symptoms include: pain, tiredness, nausea, depression, anxiety, drowsiness, lack of appetite, well-being, and shortness of breath on a 10-cm line (0 represents absence of the symptom and 10 represents the worst possible severity).
Tolerance to the treatments (morphine or morphine/ketamine) was assessed using the following: (1) the physician's evaluation: specific attention was made to psychodysleptic effects and signs of opioids overdose; and (2) the patient's point of view: the ESS is used to determine the level of daytime sleepiness and is based on eight-item scores, which represent different situational sleep propensities. 21 The total ESS score is the sum of the eight-item scores and ranges from 0 to 24 (the higher the score, the higher the sleep risk).
Patients' satisfaction was assessed using the Pain Treatment Satisfaction Scale (PTSS),26,27 which includes 39 items grouped into five dimensions: information (5 items), medical care (8 items), impact of current pain medication (8 items), satisfaction with pain medication (6 items), and side effects (12 items). A score is provided for each dimension, from 0 to 100. The higher the score on the instrument, the higher is the satisfaction level.
Statistical analysis
The sample size was determined to obtain 80% power to detect a 2-point difference (standard deviation: 1.5) in pain at 48 hours as evaluated by a numeric scale, as this difference was considered to be clinically pertinent. With statistical significance set at a p value of 0.05, these calculations showed that a total of 16 patients were needed. Assuming that a potential 10% of patients would be lost to follow-up, a total of 18 patients would need to be included. The final sample included 11 patients in the control group and 9 patients in the experimental group. Baseline characteristics between the control and experimental groups were compared using Fisher's exact tests for frequencies and Mann-Whitney tests for quantitative variables. NPIS scores at T1, at T2, at T3, and changes between NPIS baseline and NPIS at T1, T2, and T3 were compared between the two groups. Analysis of variance for repeated measurements was performed to compare changes in pain scores over the time between the two groups. The proportion of patients with a 30% reduction in pain level at T1, T2, and T3 are provided for each group. The ESAS dimension scores, the total ESS score, and the PTSS dimension scores were also compared between the two groups. Statistical significance was defined as p<0.05. Statistical analysis was performed using the SPSS version 15.0 software package (SPSS, Inc., Chicago, IL).
Results
Clinical characteristics
Twenty subjects were included during the study period. Patients' characteristics are shown in Table 1. The two groups were well-balanced for baseline characteristics. Pain level and ESS scores at baseline were not statistically different between the two groups. In the ketamine group, the initial dose of ketamine ranged from 23 to 43 mg per day.
BMI, body mass index.
NPIS, Numeric Pain Intensity Scale (0 lowest and 10 highest level of pain).
M±SD, mean±standard deviation; N(%) effective (percents); Med(IQR), median (interquartile range).
P value (Fisher's exact test for qualitative parameters, or Mann Whitney test for continuous parameters).
Efficacy: Pain and symptoms
As shown in Figure 2 and Table 2, self-reported pain did not differ significantly between the two groups during the three evaluation periods, regardless of the raw values and differentials (T2 change from T0, T3 change from T0) and global change over the time. Nevertheless, we noted that the decrease in pain at T2 was almost 2 points (1.95±2.82) in the ketamine group, whereas the decrease in pain in the placebo group was only 0.2 points. The proportion of patients with a 30% reduction in pain level at T1, T2, and T3 did not differ between the two groups. In the placebo group, 22.2%, 33.3%, and 25.0% of patients experienced this reduction in pain at T1, T2, and T3, respectively, whereas 36.4%, 30.0%, and 50.0% of patients in the ketamine group experienced this reduction at the respective time points. Whereas the 11 patients who received ketamine required a dose escalation according to the protocol, 4 of these 11 patients had a decrease in their NPIS score of at least 3 points in 48 hours (T3) without any significant increase in the amount of morphine consumed. Concerning changes in symptomatology (ESAS), no differences were found regardless of the symptom scale. Morphine consumption did not decrease during the study period. Patients in the ketamine group did not receive a significantly higher quantity of morphine, and the continuous, bolus, and cumulative doses were not different between the two groups.
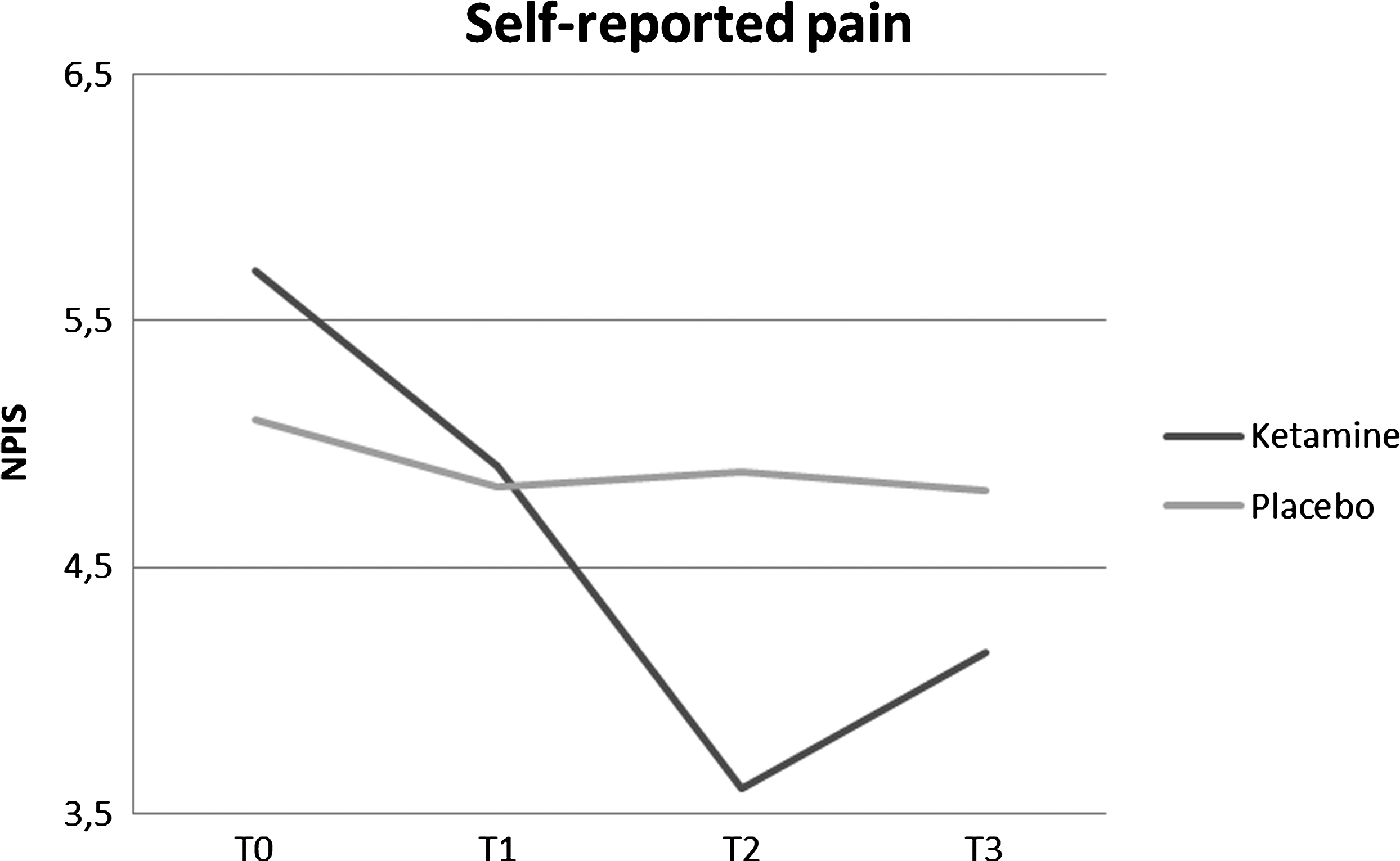
Changes in pain scores over the time between the two groups. T0, ketamine or placebo introduction time; T1, 2 hours; T2, 24 hours; T3, 48 hours after treatment initiation.
NPIS, Numeric Pain Intensity Scale; 0 lowest and 10 highest level of pain.
ESAS, Edmonton Symptom Assessment Scale; 0 absence to 10 worst possible severity.
ESS, Epworth Slumber Scale; the higher the score, the higher the somnolence.
P value for comparison ketamine versus Placebo.
T0, treatment initiation; T2, 24 hours after T0; T3, 48 hours after T0.
Tolerance: Adverse effects and sleepiness
Only one serious side effect was noted. One patient of the placebo group died during the study period. There were no adverse effects imputable to ketamine. With regard to the sedative effects, there was no significant difference between the ESS values in the two groups (Table 2).
Patient's satisfaction
PTSS scores are detailed in Table 3. No differences were found between the ketamine and placebo treatments. The ketamine group did not report greater satisfaction in regards to the medical care, the impact of the current pain medication, or the pain medication at T3. Furthermore, the satisfaction in regards to the side effects did not differ between the ketamine and placebo groups.
PTSS, Pain Treatment Satisfaction Scale (the higher the score, the higher the satisfaction level).
T0, treatment initiation; T3, 48 hours after T0.
P value Mann-Whitney test.
Discussion
Our study is the first to assess the efficacy of ketamine on cancer pain refractory to opiates among patients managed in palliative care units.
Four similar studies have been performed previously on different cancer populations. Two studies have focused on patients with cancer pain.15,16 In a cross-over study that was performed in 10 patients, Mercadante and colleagues found that an intravenous bolus dose of ketamine significantly reduced the pain intensity of the patients compared with treatment with saline solution, but higher doses were shown to entail central nervous system effects. 15 Lower doses of oral ketamine have been shown to be effective coadjuvant analgesics for cancer pain management without increasing somnolence. 16 The two additional studies17,18 were performed on patients with pain due to terminal cancer This first trial included 20 patients and was a cross-over study. Intrathecal ketamine was found to enhance the analgesic effect of intrathecal morphine. 18 The second study was performed on 48 terminal cancer pain patients and found that lower doses of epidural ketamine increased the duration of analgesia without increasing the incidence of adverse events. 17 These last two studies analyzed patients after using invasive routes of administration (intrathecal and epidural). None of these studies specifically studied the needs of the palliative care unit population.
Although we used a rigorous study schedule and employed a randomized, double-blind, placebo-controlled design, we did not find statistically significant differences between the ketamine-morphine combination and placebo with morphine in terms of its analgesic effects, its tolerability, or patient satisfaction. The reasons for this may be several fold.
We could hypothesize that the lack of efficacy was due to the use of too low doses of ketamine 15 ; this hypothesis is reinforced by the minimal number of adverse effects noted. In palliative care units, patients suffer from advanced cancers and often need co-analgesic treatments with multiple pain medications. In this study, patients suffered from refractory pain and had a long previous history of analgesic treatment. Such patients may have altered metabolism of ketamine,28,29 making it difficult to highlight ketamine's effects. It may be that the patients required higher doses of ketamine than we used. However, the results allowed us to confirm that low doses of ketamine do not involve any serious adverse effects in this population.
Although some authors have reported that patients treated with ketamine had a lower daily consumption of morphine, the morphine consumption did not decrease during the study period when the patients received ketamine. 16 Our patients suffer from pain unresponsive to morphine and are already advanced in the course of their pain syndrome. This may explain why morphine consumption did not change during the 2-day course of the study. In such a context, a longer data collection period should be used to highlight this phenomenon.
One limitation of this study was that the sample size is too small, prohibiting further conclusions. This limitation is a consistent problem in this specific area of research. Whereas it looks as though nearly 50% of the patients seemed to have had major analgesic responses, moderate efficacy may have been missed due to low statistical power. The sample size did not allow us to use a multivariate approach. This might have been useful, as potential confounding factors could have been identified.
Furthermore, pain decreased more than 3 points for four patients in the ketamine group, which might be reflective of the possible efficacy of ketamine in select patients. Future research is needed to identify factors that characterize “good responders” or “poor responders” to ketamine.
No details were provided regarding the type of pain that was experienced by the patients, which prohibited the evaluation of how the efficacy of ketamine may differ according to the type of pain. However, it can be assumed that the majority of the individuals experienced a mixed pain that consisted of both neuropathic and nociceptive components. In an effort to homogenize the therapeutic approach, morphine was the only opioid used for treatment in the control group. Although this choice allows for the comparison of our results with those of previous and similar studies, we acknowledge that patients in a clinical setting may be given multiple opioids. The initial dose of the ketamine infusion was arbitrarily designated by the investigators because no consensus was available from the literature.
Patients were included from only 7 centers of the 22 initially planned. This experience has allowed us to highlight multiple obstacles to managing a prospective study in the singular context of palliative care. 30 First, the inclusion mode should be adapted. The availability of the teams and their ability to agree to do research on people who they judge to be vulnerable is an obstacle. This vulnerability requires a particular attention and often times, the help of a third party supporting the patient. Some authors suggested involving a third person in the doctor-patient relationship. 31
Data collection can also be an obstacle. In palliative care, more than in other settings, interviewing a patient requires time and rapid or adequate adjustment to his or her reactions. At the same time, investigators need specific skills concerning the relational aspects of end-of-life care and about the technical aspects of clinical research. This vulnerability in the palliative care patient population also raises difficulties concerning the availability of patients as well as their moral and physical capacity to take part in the study. Richards and coworkers also specify that patients' health can frequently degrade during the course of the study period. 32 The adapted study design seems desirable for a study with a short study period, few secondary objectives, and simple questionnaires.
To conclude, we are unable to confirm that the ketamine-morphine combination has a superior analgesic effect to morphine alone. However, despite the fragile state of our patients, we did not observe any major side effects. Intravenous and continuous administration seems adaptive to patients in palliative care units. We also highlight the necessity of a global approach to pain management during this highly symptomatic and terminal phase. This context was a difficult one in which to perform this preliminary study of ketamine use in palliative care. The results of this work must be confirmed by a more powerful study that takes these difficulties into account.
Footnotes
Acknowledgments
We are grateful to all of the patients who participated in this study. Drs. Sébastien Salas and Matthieu Frasca contributed equally to the study.
Author Disclosure Statement
This study was financed with the gracious help of the Foundation of France. The sponsor was represented by Assistance Publique, Hôpitaux de Marseille. No competing financial interests exist.