
Abstract
Abstract
Objective:
To examine the characteristics of United States hospitalizations that result in hospice transfers including the clinical and demographic features, and to determine distinctive factors associated with discharges to hospice(DTH).
Methods:
The National Inpatient Sample(NIS) databases for 2000-2009 were queried for hospitalizations which resulted in transfers to hospice and expiration in the hospital. Yearly totals, as well as demographic and clinical features were tabulated for DTH hospitalizations. These characteristics were also compared with hospitalizations that ended with expiration using multivariate regression.
Results:
The number of DTH per year increased 15 fold from 27,912 in 2000 to 420,882 in 2009. The median hospital stay decreased, while the median age, proportion of sepsis disease related groups(DRGs), and proportion of Medicare hospitalizations increased. Lung, gastrointestinal, hepato-biliary, and brain cancer were consistently the most prevalent malignancy DRGs. However, the initial preponderance of hospitalizations with any diagnosis of cancer was diminished by the end of the study. The adjusted odds ratio(95%CI) for the prediction of DTH(compared to hospital death) by any diagnosis of cancer decreased from 3.61(3.52-3.71) to 2.02(2.00-2.04) from the years 2000-2009. Female gender, age, and chronic obstructive pulmonary disease were predictors of discharge to hospice, while congestive heart failure was inversely associated.
Conclusions:
Hospital discharges to hospice have increased over the past ten years, with a concomitant shift in clinical and demographic characteristics. A growing trend toward offering and adopting hospice care upon discharge from US hospitals will likely impact health care finance and quality of care measures.
Introduction
Over the past decade the number of hospice subscribers in the United States (US) has increased from 700,000 in 2000 to 1.56 million in 20095,6. However, the referral sources of this increase and the clinical course leading to enrollment in hospice has not been detailed on a national level. The characteristics of a hospital stay (e.g. total charges, length of stay, associated diagnoses) leading to discharge to hospice could add to our understanding of the growth in hospice enrollment. and can provide insight into patterns and sources of end of life expenses. We hypothesized that patients whose hospitalization ended in inpatient death or resulted in discharge to hospice(DTH) would share many characteristics and that defining differences in co-morbidity and demographics between these categories could provide a view of how this end-of-life option is currently being offered to US hospital in-patients. We analyzed a database sample of US hospitalizations, to examine characteristics of hospitalizations which resulted in DTH as compared to hospitalizations ending in death and to estimate the prevalence of DTH between 2000 and 2009.
Methods
Data sources
The National Inpatient Sample(NIS) of the Healthcare Cost and Utilization Project(HCUP), is funded by the US government's Agency for Healthcare Research and Quality (AHRQ) and contains annual hospital discharge data from a stratified, random sample of hospitals across the US 7 . The NIS includes public and private hospitals, teaching and non teaching hospitals, urban and rural hospitals and small/medium/large bed sized hospitals. Each NIS patient record includes data fields consisting of demographic, clinical and financial information. These fields include primary and secondary diagnostic fields, procedure codes, age, sex, race, total charges, length of stay and disposition status. Weights are provided for calculation of national estimates. The database for each year contains hospital discharges which account for 36,417,575 (2000) to 39,434,956 discharges per year (2009). The study was approved by the New York Downtown Hospital Institutional Review Board.
Case selection and classification
The NIS Core Databases for the years 2000-2009 were queried for patients who expired in the hospital, or were discharged to home or medical facility hospice. The later two dispositions were regrouped into one hospice outcome. The estimated yearly number of hospice subscribers was obtained from National Hospice and Palliative Care Organization's report (NHPCO).
Within this cohort, the frequencies of Diagnosis Related Groups (DRGs) were analyzed. DRG version 18 was used for years 2000 through 2005 and DRG version 24 was used for years 2006 through 2009, based on the presence of these variables in the NIS Database. The most common DRG categories(twenty) of patients discharged to hospice were tabulated to analyze patient demographics by year. DRGs describing the same diagnoses were combined into one category.
Statistical analysis
Summary data generation and all data analysis except for negative binomial regression were performed using SPSS for Windows Version 13 (SPSS Inc, Chicago, IL, USA). The national prevalences of DTH and expiration associated discharges were estimated by applying the proportions in hospitals without missing disposition to hospitalizations that had missing disposition(14.3% over the study period). Yearly charges based on estimated total DTH and expiration associated discharges were also calculated, taking into account charges relating to missing dispositions. Charges were reported in 2009 dollars using the consumer price index to adjust yearly amounts prior to 2009. Group differences in total charge between expired patients and hospice patients over time were examined using ANCOVA (GLM).
Negative binomial regression was performed using SAS for Windows version 9.1 (SAS Institute, Cary, NC,USA) to analyze trends in hospice discharges and expired patients using the GENMOD procedure 8 . Group effects were analyzed for DTH versus expired patients, and for DTH versus estimated non-hospital referrals to hospice(calculated by substracting yearly DTH from total yearly hospice enrollment), taking into account the total US population as the offset variable.
Co-morbidities of particular interest in distinguishing hospice from expiration in the hospital were identified by ICD-9 codes and included cancer (140.0-239.9), cerebrovascular disease (430*-438), congestive heart failure(CHF) (428*), chronic obstructive pulmonary disease(COPD)(491*-492*), dementia (290*), renal failure (403.01, 403.11, 403.91, 404.02, 404,03, 404.12, 404.13, 404.93), malnutrition (262*,263*), and dehydration/electrolyte imbalance (276.*). These co-morbidities were selected based on their association with hospice care, and their high prevalence in selected cohort. The presence of gastrostomy status (V44.1), abnormality of gait (781.2), or weakness interfering with activity (780.79) were each considered as an index of frailty(frailty indicator). Mechanical ventilation (96.71,96.72) or endotracheal intubation (96.04), were examined as a clinical characteristic of interest.
Logistic regression was performed to examine significant associations with the outcome of discharge to hospice compared to expiration in the hospital. Predictor effects were examined for demographic variables (age and sex), mechanical/intubation and relevant co-morbidities. Stepwise forward selection was employed. Because race was missing in a significant proportion of earlier year databases(between 25 and 30%) and because, when entered, race had a marginal effect in multivariate modeling, it was not used in logistic regression models.
Results
General characteristics of hospice discharges
Between 2000 and 2009, there were 2,279,541 discharges to hospice, with 1,010,082 discharges to a medical facility and 1,269,459 discharges to home hospice(Figure 1). In the study period DTH accounted for 0.59% of hospital discharges, and increased from 0.08% of discharges in 2000 to 1.07% in 2009 (Table 1). Cancer was the most prevalent co-morbidity in this population, present in 57.7% of discharges in 2000 and 43.6% in 2009 (Table 1). DTH were more frequently female, from 2000-2009 the percentage of female DTH rose from 54.4% to 55.3%. The median age, total charges, percent paying with Medicare, percent African American(not shown), and percent non-White patients increased throughout the study years, while the median length of stay decreased (Table 1). The total charges for DTH rose from 0.11% of total hospital charges in 2000 to 1.61% of total hospital charges in 2009.
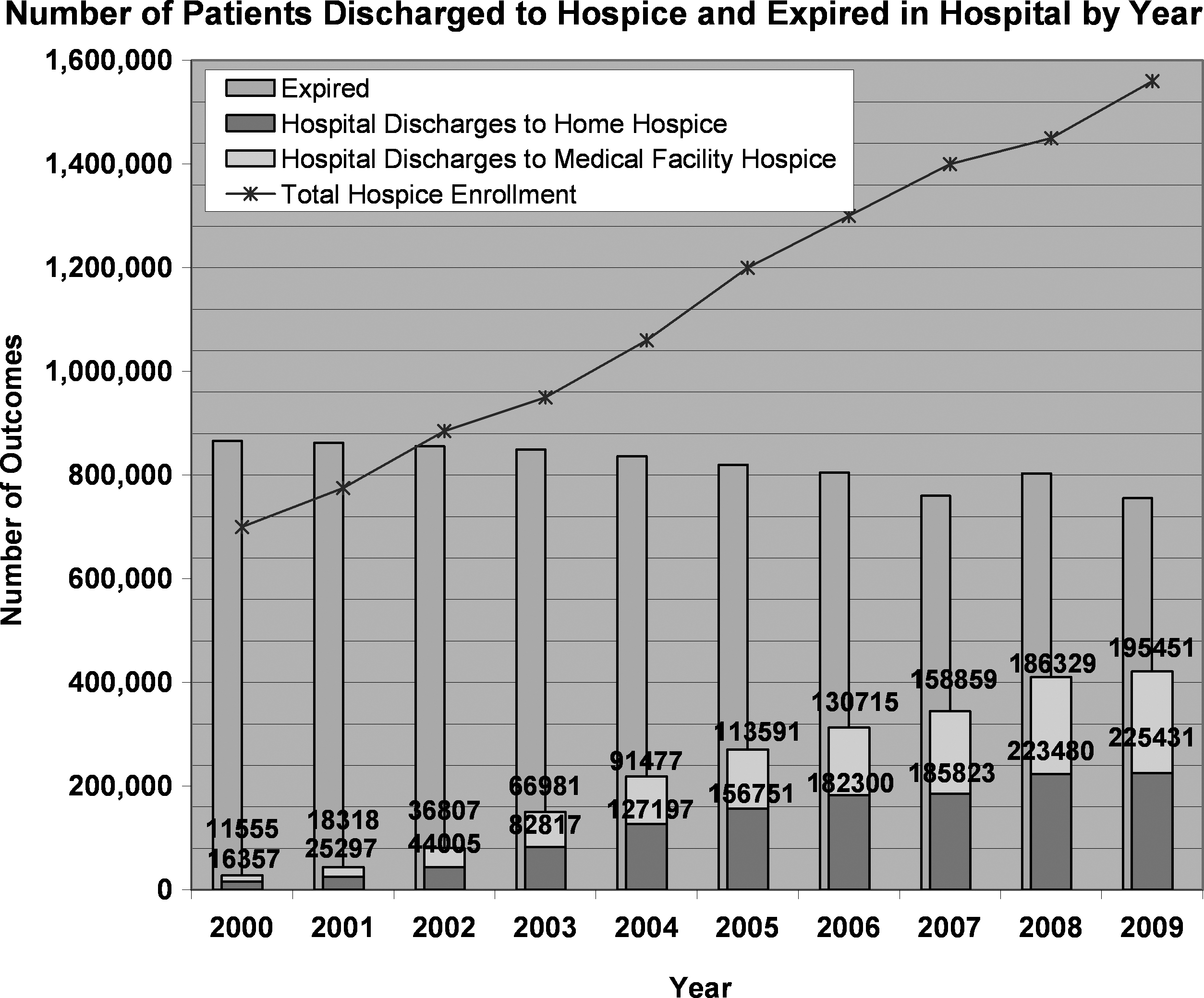
Yearly hospital discharges to hospice, hospital expirations, and hospice enrollees.
The top 20 DRG groupings in hospice patients are shown in Table 2. The DRG grouping respiratory infection (DRGs 79, 80, 81, 89, 90, 91) constituted the largest clinical group in all years (n=164,433; 7.9%). The DRG septicemia increased in DTH from 948 (3.43%) in the year 2000 to 30,801 (7.9%) in the year 2009, with combined septicemia and pneumonia DRG increasing from 12.14% to 15.27% of DTH. The septicemia DRG also increased in hospitalizations ending in expiration, from 5.9% in 2000 to 15.1% in 2009, and combined septicemia and pneumonia increased from 14.90% to 21.20% in this group. The percentage of DRGs related to cancer groupings decreased in this population from 2000 to 2009, specifically in respiratory neoplasms (n=2171; 7.8% to n=17473; 4.5%), hepato-biliary neoplasms (n=1235; 4.5% to n=11420; 2.9%) digestive malignancy (n=1077; 3.9% to n=9147; 2.4%), and lymphoma/leukemia (n=717, 2.7% to n=4671; 1.2%).
Cancer was the most common comorbidity and was prevalent in the most common non-cancer DRGs (Tables 3 and 4). CHF increased in prevalence as a comorbidity between 2000 and 2009 from 18.6% of hospice patients to 26% of hospice patients(Tables 3 and 4). Dehydration was also highly prevalent among hospice, and increased from 2000 to 2009(Tables 3 and 4). Other co-morbidities that showed increases from 2000 to 2009 were malnutrition, frailty indicator, diabetes, dehydration, and COPD (Tables 3 and 4). Mechanical ventilation/endotracheal intubation also increased in patients discharged to hospice from 2000 to 2009 (Tables 3 and 4).
Time trend analysis related to hospice discharges
There was a significant positive year trend for hospital discharges to hospice, as well as estimated non-hospital referrals to hospice(p<.0001). Hospital discharges to hospice increased from 27,912 in 2000 to 420,882 in 2009 (Figure 1). The increase in DTH, and hospice enrollment from other sources(non-hospital referrals to hospice as previously defined), showed a significant group by year interaction (p<.0001), indicating a more rapid growth in DTH. In contrast, expiration in the hospital showed a diminution with time(p<.0001), decreasing from 866,049 in 2000 to 755,710 in 2009. Hospital charge also showed a significant positive year effect for both hospice and expired patients (p<.0001)(Figure 2). The rate of rise of per discharge charges was significantly higher for expired patients than patients discharged to hospice (ANCOVA, p<.0001)(Figure 2).
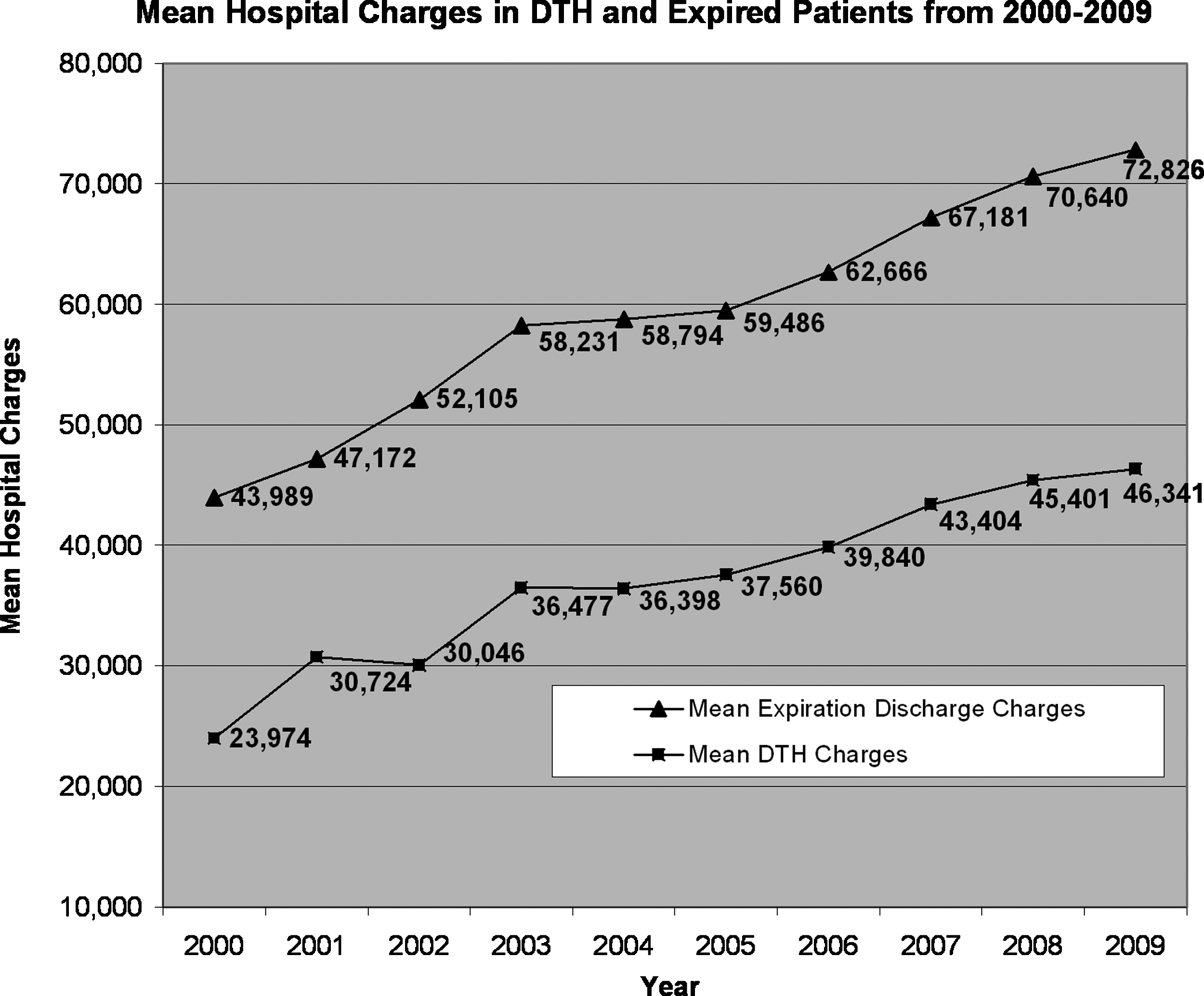
Mean yearly charges for hospitalizations resulting in DTH and for expiration hospitalizations.
Associations for hospitalizations discharged to hospice
Cancer was most strongly associated with a discharge to hospice relative to expiration in the hospital by univariate(not shown) and multivariate analysis, but it showed a decrease in magnitude of association(odds ratio) from 2000 to 2009 (Tables 5). Female gender, dementia, increasing decade of life, COPD, and frailty indicator also showed significant associations with a discharge to hospice by multivariate analysis throughout the study years (Table 5). Mechanical ventilation was the most negatively associated predictor for transfer to hospice compared to hospital expiration (Tables 5). Renal failure and CHF were also negatively associated with hospice discharges by univariate(not shown) and multivariate analysis(Table 5).
Discussion
Hospice care has been a growing area of public interest, as well as a growing health care expense in the United States 9 . Studies have shown that terminally ill patients prefer to die in the comfort of their home, and that home hospice increases the likelihood of this occurring 10 . Other reports have promoted implementation of palliative care programs, which have doubled in the past decade 11 as a means to reduce the cost of end of life care. 3 In this study, we examined characteristics of DTH hospitalizations, and defined distinctions between DTH and hospital expirations.
Our findings show that over the study period hospital deaths declined and there was an increase in DTH. These findings indicate a significant shift in end of life care in the United States. We also found a more rapid increase in DTH relative to non-hospital based hospice referrals, suggesting that end of life care is still focused in hospitalizations. The cost of these hospitalizations leading to DTH amounted to 19.5 billion dollars in total hospital charges in 2009(71.9% of which had Medicare as the payer). This compares to the 2009 total hospice charges to Medicare of 12 billion dollars 8 . Assuming a similar payer mix in total hospice enrollment 12 it can be calculated that in 2009 the Medicare hospitalizations resulting in DTH accounted for about 27% of that year's total Medicare hospice patients, and that these patients' hospitalizations alone cost more than the year's total Medicare costs for hospice care.
Financial incentive may be a societal consideration for discharge to hospice, and our findings suggest that hospice should be examined further as a cost saving measure. Chang and Steinberg reported that hospice enrollment is related to decreased inpatient mortality, with every 100 enrollments resulting in 28 fewer inpatient deaths 13 . Accordingly, with a reported increase of hospice patients by 860,000 between 2000 and 20095,6, one would expect a decrease of hospital expirations of 240,800. Although we did find a decrease in inpatient mortality over the study period, it only amounted to 110, 000 less hospital expirations(of which many obviously were not related to chronic terminal disease), which is less than half of the expected value. While the total hospital charges for these hospice discharges increased 29 fold, the total yearly charges for hospitalizations ending in expiration dwarfed those of DTH's. These findings underscore the financial impact of these hospitalizations and the need for measures to reduce both the number and the cost of these admissions.
Cancer DRG categories continued to be in the top DRGs throughout the study period, with lung cancer, hepato-biliary cancer, gastrointestinal cancer and brain cancer consistently being the most common. However, the steady decrease in any cancer patient proportion in discharges to hospice as well as the decreasing odds ratio for cancer as a predictor of discharges to hospice compared to hospital expiration, points toward an increasing diversity in patient selection for DTH over time. This is consistent with growing awareness in the medical community about the appropriate use of palliative care in non-cancer diseases such as heart failure and chronic obstructive lung disease14,15. The increase in the proportion of sepsis DRG in DTH in later years illustrates how serious infections such as sepsis and the most common DRG category of pneumonia, also an infectious process, represent a growing common final pathway in the DTH population. Indeed this trend was also seen in hospitalizations ending in expiration. Also of interest is the small but real increase in the age of DTH over time. This is may reflect both an aging American population, as well as an improved ability to treat patients with potentially fatal disease longer and more effectively.
Another demographic change found relates to race. In past studies, African Americans were found to be more likely to receive aggressive end of life treatment, and less likely to receive palliative care 16 . Our findings showed a modest increase in non-white patients discharged to hospice between the years of 2000 and 2009, particularly in African American discharges(not shown), suggesting that this disparity may be decreasing. The fact that race had such a negligible impact as a multivariate predictor for discharge to hospice(compared to hospital expiration), suggest that racial differences were subsumed by other clinical and demographic factors.
While there have been other studies looking at characteristics of total hospice enrollment, to our knowledge this is the first study to look specifically at the population of hospital discharges to hospice on such a large scale. There are some limitations to this study. Based on the structure of the database, we were unable to identify patients who were readmitted, which may have led to overestimation of hospice discharges. Additionally, prevalence may have been underestimated for co-morbidities, due to under-reporting and under-coding of diseases outside of the primary diagnosis17,18. DRG coding changed over the study period(as described in the methods section) and may have led to some changes in the proportion of DRGs.
The past decade has been a dynamic period for hospice and palliative care. Palliative care has grown as a field, and palliative care services at hospitals have been shown to increase the likelihood of referral to hospice earlier in the course of disease 19 . Additionally, the number of nursing home hospice programs has increased, enabling their enrollment to more than double 20 . Finally, there has been a change in clinical characterization of hospice patients, with an increasing number of hospice patients with non-cancer diagnoses 6 . It is likely that these transformations to the field have contributed to the observed changes in hospital discharges to hospice.
Footnotes
Acknowledgments
The authors acknowledge New York Medical College in supporting Ms. Levine's summer research.
Author Disclosure Statement
No competing financial interests exist.