
Abstract
Abstract
Background:
Patients with advanced lung cancer constitute a special focus in palliative care not only for epidemiological or prognostic reasons, but also because their symptom burden is felt to be widespread and difficult to treat. This study describes disease-specific characteristics and the symptom burden of patients with advanced incurable lung cancer, comparing them with patients suffering from other diseaseentities.
Methods:
A secondary analysis of the nationwide Hospice and Palliative Care Evaluation (HOPE) was performed, by focussing on inpatient hospice and palliative care unit patients and by using descriptive methods.
Results:
From 2006 to 2008, 5487 inpatients were registered, 874 of which were diagnosed with lung cancer and 1884 with pulmonary metastases. Symptoms such as weakness, tiredness, or pain were most prevalent in all subgroups. Dyspnea was significantly more prevalent in all patients with different kinds of pulmonary tumor manifestations; confusion was significantly more prevalent in patients with lung cancer. Dyspnea could not be treated as effectively as pain or nausea. Confusion and nursing problems worsened during the observation period. Dyspnea and confusion were associated with increased risk of death during the observational period.
Conclusion:
The symptom pattern of patients with lung cancer is characterized by dyspnea and confusion—symptoms that are difficult to treat until discharge and that imply a worse prognosis. Therefore, increased research on the pathophysiology and treatment of dyspnea and confusion is required, and efforts in advance care planning and anticipation of dyspnea and confusion as a critical symptom in patients with lung cancer should be reinforced.
Introduction
Besides these aspects, patients with advanced lung cancer constitute a special focus in palliative care: Temel and colleagues 3 found that patients with stage IIIb/IV non-small cell lung cancer not only had better quality of life and less aggressive treatment when receiving early structured palliative care interventions, but also had a significantly increased overall survival. In day-to-day clinical practice, though, the symptom burden of patients with advanced lung cancer and also with pulmonary metastases is felt to be widespread and difficult to treat. This correlates with findings from our institutional emergency medical service (EMS), where patients with lung cancer contributed most to the patients with advanced cancer that required prehospital emergency medical help (delivered by the EMS team including an emergency physician; 25.4%). 4
Further literature on patients with incurable lung cancer describes, for example, patterns of symptom intensity, 5 quality-of-life aspects, 6 gender aspects, 7 and the patients' experience of pain, 8 but data comparing specific palliative care needs of patients with advanced lung cancer as compared with patients suffering from other disease entities are scarce. Therefore, it is widely unknown why patients suffering from lung cancer are particularly vulnerable to emergencies, and whether the outstanding benefit of palliative care interventions, as found by Temel, 3 is to be retraced to specific medical or psychosocial conditions attributed to this disease entity.
The following study was therefore conducted to assess the specific needs and problems of patients with advanced lung cancer and pulmonary metastases, compared with patients in specialized palliative care who suffer from other disease entities.
Methods
A secondary analysis of the Hospice and Palliative Care Evaluation (HOPE) 9 was performed.
Hospice and Palliative Care Evaluation (HOPE)
HOPE is a prospective, annual, nationwide multicenter survey that collects epidemiological and clinical data from institutions that treat in- and outpatients from a palliative care perspective (i.e., palliative care units, inpatient hospices, oncology wards, general practitioners, oncology specialists, and palliative home care teams). Each participating institution was supposed to survey and assess 30 consecutive patients in a 3-month period per year. 10 Besides information on demography and underlying disease (age, gender, diagnosis, metastases, concurrent diseases), data on prevalence and intensity of symptoms, as well as psychological, nursing, and social problems were assessed by staff via an integrated symptom checklist using a 4-point grading scale. Detailed information on the development of the documentation tool has been published previously.11,12
Data management
Data from patients who suffered from lung cancer, pulmonary metastases, or both were gathered, and compared with patients without pulmonary tumor manifestations. In addition, the data were compared with the German cancer registry data. 1 Due to the heterogeneity of the participating institutions (including palliative care liaison services, hospital support teams, oncology wards, etc.) the focus was placed on hospice and palliative care inpatients. Data were merged from 3 consecutive years (2006–2008) and cleared from incomplete data subsets.
Definition of groups
1. All hospice and palliative care inpatients;
2. Patients with (primary and secondary) pulmonary tumor manifestations;
3. Patients with (primary) lung cancer (ICD 10 C34.-);
4. Patients with (secondary) pulmonary metastases;
5. Patients with pulmonary metastases from lung cancer (intersection of 3 and 4);
6. Patients without lung cancer (total cohort (1) minus subgroup 3);
7. Patients without malignant pulmonary disease.
Data analysis
Statistical analysis comprised Wilcoxon-Mann-Whitney testing, χ2 testing, as well as log rank testing for time to event data; results were deemed significant for p<0.05. Where appropriate, p values have been adjusted for multiple comparisons by Bonferroni's method. SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL) and Microsoft Excel version 2003 (Microsoft, Redmond, WA) software were used.
The study was approved by the local ethics authorities (registration number 17/3/09).
Results
From 2006 to 2008, a total of 8173 patients were surveyed in HOPE. Too provide comparable data, focus was placed on 5731 hospice and palliative care inpatients, and a further 244 patients had to be excluded due to missing, not evaluable, or incomplete data subsets.
The detailed secondary analysis therefore comprises 5487 inpatients from palliative care units and inpatient hospices (Fig. 1). On overage (mean % of 3 years), 30.5% of all palliative care units and 11.7% of all inpatients hospices contributed to the survey. 13
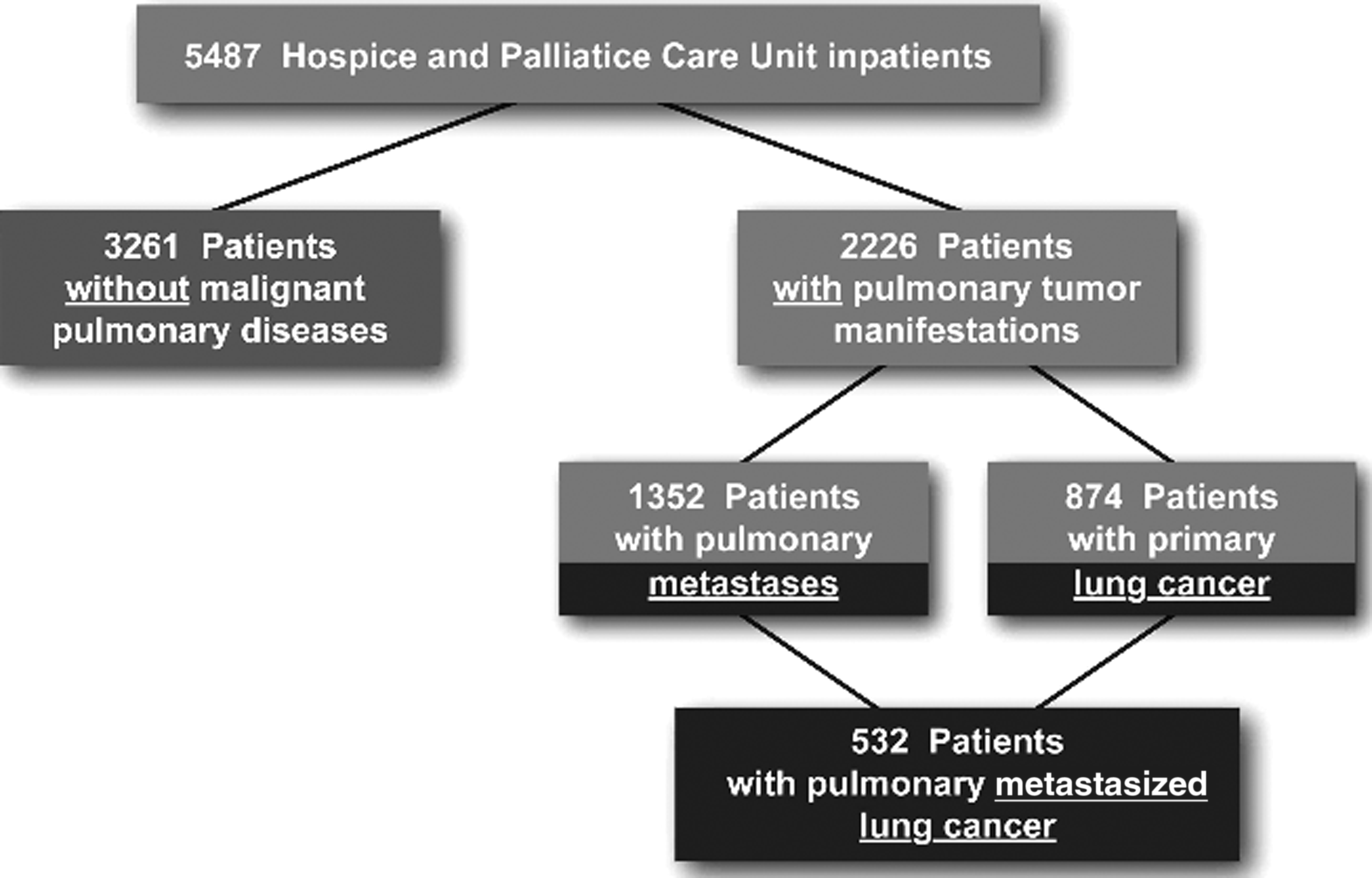
The Hospice and Palliative Care Evaluation 2006–2008 and study population.
Table 1 shows the epidemiological characteristics of this general inpatient hospice and palliative care population. This general cohort suffered from a variety of (predominantly) cancer entities: cancer of the gastrointestinal (GI) tract was the most often registered main diagnosis (26.1%), and only 5.7% suffered from incurable noncancer disease. Of the total cohort, 2226 patients (40.6%) had malignant pulmonary disease: of those, 874 patients suffered from lung cancer (15.9%), 1884 patients had pulmonary metastases (34.3%), and 532 patients (9.7%) had lung cancer with pulmonary metastases (an intersection subgroup of the two previous subgroups). The subgroup of lung cancer patients did not differ from the total cohort with respect to place of registration, whereas patients with lung cancer tended to be somewhat younger than the general cohort (p<0.0001).
ECOG, Eastern Cooperative Oncology Group; SD, standard deviation.
Table 1 also demonstrates a study population of patients with compromised functional status.
Significantly more women than men were registered in HOPE (53.9% versus 46.1%, p<0.0001), whereas nationwide cancer statistics show that more men than women die from cancer in Germany (Table 2). For patients with lung cancer, by far more men were registered in HOPE than women (62.1% versus 37.9%), but not as many as gender-specific differences in lung cancer-related mortality (70.9% versus 29.1%) 1 might have suggested. These differences of gender distribution in lung cancer patients (male to female ratio, Table 2) were also shown to be significant (p<0.0001).
HOPE, Hospice and Palliative Care Evaluation; PCU, palliative care unit; RKI, Robert Koch Institute. 1
Some of the registered symptoms such as weakness, pain, loss of appetite, constipation, family problems, or organizational problems were found to be similar between patients with or without pulmonary tumor manifestations.
On the other hand, patients with pulmonary tumor manifestations (66.3%), especially those with lung cancer (72.2%) or pulmonary metastases from lung cancer (75.8%), were found to have significantly (p<0.0001) more dyspnea than patients without malignant pulmonary disease (42.2%). Interestingly, dyspnea was less more prevalent in patients with pulmonary metastases (62.3%), but still more prevalent than in patients without malignant pulmonary disease.
Similarly, a higher percentage of patients with lung cancer suffered from confusion, as compared with patients with pulmonary metastases or patients without any pulmonary tumor manifestations.
Results on anxiety were less distinct: in patients with lung metastases, anxiety was more prevalent (73.5%) as compared with patients with lung cancer (71.5%) or without malignant pulmonary disease (69.4%), without reaching significance level (p<0.007).Vomiting was significantly less often reported (p=0.004) in patients with lung cancer (23.0%) than in patients with pulmonary metastases (29.1%) or (p<0.0001) without any malignant pulmonary disease (31.2%).
Also, problems in day-to-day nursing care were less often reported in patients with lung cancer as compared with patients with pulmonary metastases or without any malignant pulmonary disease, and fewer patients with lung cancer and pulmonary metastases were formally approved for nursing support as compared with patients without pulmonary tumor manifestations (28.5%/27.3% versus 31.1%). Functional state as scored by ECOG (Eastern Cooperative Oncology Group) 13 was not different through all subgroups (see Table 1 and Table 3).
Symptoms significantly more prevalent in patients with lung cancer (see text).
PCU, palliative care unit.
At the end of inpatient treatment, the prevalence of most of the named symptoms decreased (i.e., could be effectively relieved) in all subgroups, especially symptoms such as pain (e.g., 76.7% on admission versus 52.2% at the end of treatment in lung cancer patients) or nausea (42.6% versus 22.3% in lung cancer patients). Dyspnea was significantly relieved on discharge (72.2% versus 64.5% in lung cancer patients, p<0.0001), but the improvement was much smaller than the one in pain or nausea (Fig. 2). Weakness or nursing problems could not significantly be solved. Confusion was the only symptom that was even significantly more prevalent on discharge than on admission in nearly all subgroups (formal significance level was not reached for patients with lung cancer; here, the prevalence of confusion rose from 40.7% to 43.5%).
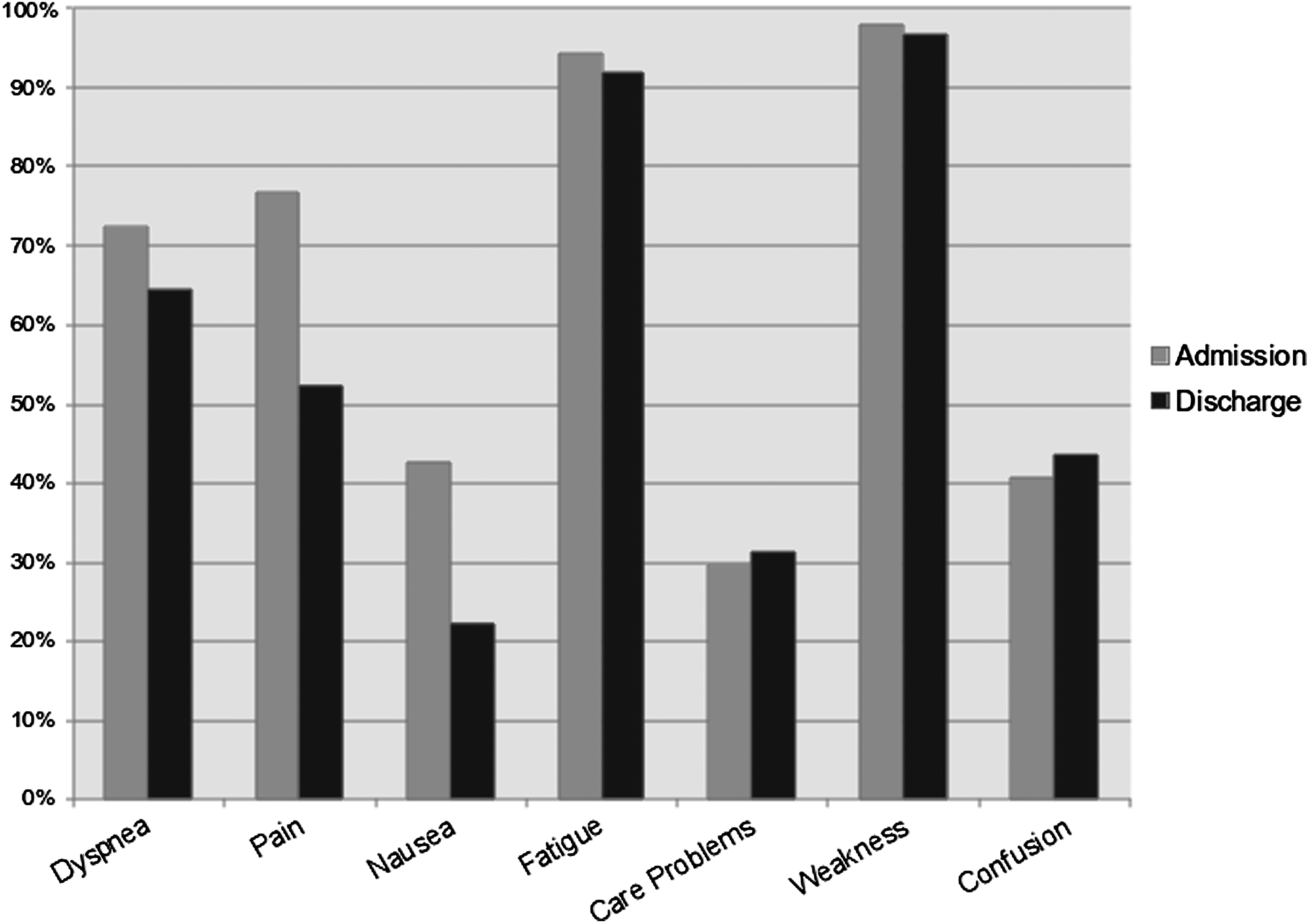
Prevalence of selected symptoms on admission and on discharge in the subgroup of patients with lung cancer.
About half of the study population died during the observation period while receiving inpatient care. The clinical course of patients with lung cancer showed that death during the observational period occurred significantly more often than in patients without malignant pulmonary disease, and median survival from the beginning of the documentation period was 17 days in lung cancer patients as compared with 18 days in palliative care patients without lung cancer (log rank, p=0.035). In patients with lung cancer who suffered from dyspnea, the probability to die during the observational period was significantly higher (p<0.0001) than in patients without dyspnea.
Discussion
In palliative care, a “common pathway toward death” 15 for underlying malignant or nonmalignant disease entities has been traditionally advocated. This analysis of a large nationwide survey in hospice and palliative care instead showed distinguishing features of patients with advanced incurable lung cancer as compared with patients without lung cancer or other pulmonary tumor manifestations that deserve clinical attention.
This finding is in line with recent research on patients with noncancer disease or brain tumors in palliative care who were found to have disease-specific demands and problems in the German Hospice and Palliative Care Evaluation.16,17
Two relevant characteristics of patients with lung cancer were the significantly elevated prevalence of dyspnea and confusion. From a clinical perspective, this finding may be even more relevant as these symptoms could hardly be satisfactorily relieved or reemerged until discharge or death, similar to weakness or nursing problems, but as opposed to other prevalent and well-treatable symptoms in palliative care such as pain or nausea. Also, dyspnea proved to be an predictive sign for death during the observational period.
The prevalence of dyspnea and confusion in lung cancer patients was considerably higher than in patients with pulmonary metastases; from a clinical standpoint, this might be attributed to specific biologic features and growth pattern of lung cancer as opposed to pulmonary metastases or other disease entities. For instance, patients with lung cancer might be particularly vulnerable to centrally compressing intrathoracic tumor growth pattern, to metabolic crises such as hypercalcemia, or to concurrent brain metastases. Similarly, the low incidence of nausea and vomiting in patients with lung cancer as compared with patients with pulmonary metastases might be traced to the high proportion of patients suffering from GI cancer (or other disease entities with a high probability for pulmonary metastases) in the total HOPE cohort with a relatively high baseline prevalence of nausea and vomiting.
Considering the vulnerability and clinical susceptibility to critical situations, as described by Wiese and coworkers, 4 it is remarkable that nursing problems were not more prevalent in patients with lung cancer than in other palliative care patients, and ECOG functional state was comparable.
A distinct but clear dominance of women in the HOPE registry (and therefore probably in palliative care in general) was identified, although men contribute to cancer-related mortality in Germany (53.3%). 1 Besides other possible reasons, this finding may be attributed to traditional care models, wherein women might be able to care for their ill spouses rather than the other way round. When a woman becomes severely affected, the likelihood might be higher that she requires external support. 18 This relative dominance of women as patients in palliative care may be of special importance for a predominantly male disease entity such as lung cancer and may therefore contribute to this postulated vulnerability in clinical or home care.
To find out whether there is a disease-specific problem in underestimating subjective symptoms, our study group compared self-assessment of symptoms with assessment by staff and showed that there was no general bias toward underestimation of symptoms. 19 Instead, staff tended to overestimate symptoms (except from pain) as compared wih the patients' self-assessment.
A limitation of this study is that only a minority of all German palliative care wards and inpatient hospices contributed to HOPE, despite large patient numbers and a symptom spectrum that was comparable to previous findings on palliative care patients.11,20,21 Another limitation of the study is that it relies on data from inpatients, whereas transferability to an outpatient scenario is unclear. Relevant literature, though, shows a similar disease-specific symptom burden for outpatients with lung cancer.23 Also, rare thoracic tumor entities such as mesothelioma were not identified and described separately (but were merged with other nonlung cancer entities). Precise data on total tumor load could not be provided by the HOPE registry, and data on symptom intensity (as compared with symptom prevalence) were not subject to analysis for methodological reasons. The survey did not provide information on adequate drug treatment or dosages. Furthermore, only limited conclusions could be drawn on the course of the disease, as the questionnaire registry provided cross-sectional data and limited longitudinal data.
In conclusion, the symptom burden of patients with lung cancer is characterized by a distinctly high prevalence of dyspnea and confusion–two symptoms that cannot be as effectively treated as pain or nausea. The relative dominance of women in palliative care might be related to the vulnerability of lung cancer patients to critical situations, but general nursing support or ECOG functional state could not be verified as a distinguishing feature of this particular group of patients. Therefore, research on the pathophysiology and treatment of dyspnea and confusion and other tools to prevent emergency situations in palliative care, such as advance care planning, have to be reinforced.
Footnotes
Acknowledgments
We would very much like to thank all the participating institutions and staff members who contributed to the data documentation, and the Hospice and Palliative Care Evaluation Working Group for their support.
Preliminary results of this study have been published in abstract form for the European Association of Palliative Care (EAPC) Research Forum, Glasgow, 2010.
B. Alt-Epping and A. Stäritz contributed equally to the manuscript.
The Hospice and Palliative Care Evaluation (HOPE) is supported by the German Society of Palliative Medicine, the German Hospice and Palliative Association, and the German Cancer Society. Part of the preparatory work and the data evaluation, as well as the development of a web-based database for HOPE, was supported by a grant from Mundipharma Company, Limburg. The departments of Palliative Medicine in Cologne and Gottingen are supported by the German Cancer Aid.
Author Disclosure Statement
No conflicting financial interests exist.