
Abstract
Abstract
Introduction:
Cancer-related lymphedema management in palliative care remains a challenge for health care professionals. We conducted a systematic review of the published literature related to the effectiveness of cancer-related lymphedema management in the palliative care setting.
Methods:
Eleven major medical databases were searched. Manuscripts were selected for articles published from January 2004 to October 30, 2011, using search terms for lymphedema and palliative care. Eleven articles were selected based on defined eligibility criteria for final review and were categorized as lymphedema management in palliative care by topic experts. Articles were also rated for quality according to the Oncology Nursing Society Putting Evidence into Practice® classification.
Results:
Five case studies were identified addressing closed-controlled subcutaneous drainage; one retrospective study on manual lymphatic drainage (MLD); two case studies on compression therapy; and three case studies on complete decongestive therapy (CDT). All studies were rated in the category of “effectiveness not established” due to study limitations in design and sample size. Few studies included objective measures of outcomes, and there were no randomized controlled trials. There is a need for larger, well-designed research studies to test the effectiveness of management of cancer-related lymphedema in palliative care.
Introduction
According to the World Health Organization (WHO), 13 palliative care is an essential part of cancer care, with the optimal goal of improving quality of life for both patients and their families by providing relief from pain and other symptoms, and integrating physical, psychological, and spiritual aspects into patient care.
LE cannot be cured, but requires complex and individualized management. Consequently, LE may cause patients to feel distress and discomfort and can reduce patients' mobility and function. 14 A qualitative study by Frid et al. 15 reported that for cancer patients in the late palliative stage, the impact of LE was worsened due to the feelings of hopelessness, disgust, and social isolation. The authors did not report the definition of late palliative stage, but they stated that the time between the day of interview and the day of the patient's death ranged from 12–168 days. The International Lymphoedema Framework 16 suggested that a palliative approach is required for advanced cancer patients, since they frequently cannot tolerate a full assessment and treatment program. This highlights the importance of developing the appropriate palliative care services to properly manage LE for these patients.17,18
Towers et al. 19 suggested key concepts of palliative care that can be applied in LE care, including: (1) understanding, respecting, and not abandoning the patients; (2) including family members and community in providing LE resources and care; (3) working as an interdisciplinary team; (4) communicating with patients, family, and other palliative care providers; (5) controlling pain, other symptoms, and therapeutic problems; (6) maintaining independence and function; and (7) attending to both patient's and therapist's emotions.
In general, the goal of LE management is to reduce swelling and other symptoms and to restore function. However, for patients with advanced stages of cancer and LE, the primary goal is often to improve patient quality of life, rather than to resolve the swelling completely. Therefore, any treatment modality that may be burdensome with minimal benefit should be considered carefully.20–23
Currently, complete decongestive therapy (CDT) is the gold standard for managing LE. With some adaptations, the four components of CDT, including skin care, exercise, manual lymphatic drainage (MLD), and compression therapy, can be used to manage LE in advanced cancer patients.14,24 However, specialized LE management in palliative care has been neglected and remains a challenge for health care professionals.19,25,26
Aim
The current review is part of a larger project aimed to provide updated evidence for the Second Edition of the Best Practices Document, a joint project of the American Lymphedema Framework Project (ALFP) and the International Lymphoedema Framework (ILF), to provide evidence-based clinical practice guidelines for all aspects of LE diagnosis and management. The specific aim of this report is to review the contemporary literature related to LE management in the palliative care setting in order to identify and provide best practice recommendations for LE management in palliative care, which in turn will enhance quality of life for patients with advanced cancer and secondary LE.
Methods
A systematic review of 2004–2010 literature on LE management in palliative care was performed in two phases (Fig. 1). The initial phase was performed by a reference librarian who searched 11 medical indices (PubMed, Medline, CINAHL, Cochrane Library databases [Systematic Reviews and Controlled Trials Register], PapersFirst, Proceedings First, Worldcat, PEDro, National Guidelines Clearing House, ACP Journal Club, and Dare) for articles using the following search terms: lymphedema, lymphoedema, lymphodema, elephantiasis, swelling, edema, and oedema, to capture all literature related to LE. Additional articles from 2011 were subsequently identified and included. A total of 5927 articles were retrieved and 4624 articles not relevant to LE research were excluded by research associates (screen 1). The remaining 1303 articles were reviewed by three author team members according to pre-defined inclusion (LE-related) and exclusion criteria (non-refereed articles) criteria, and a total of 644 articles were excluded, resulting in 659 articles for consideration in review for palliative care and other topics (screen 2). Articles with no available English translation were also excluded.
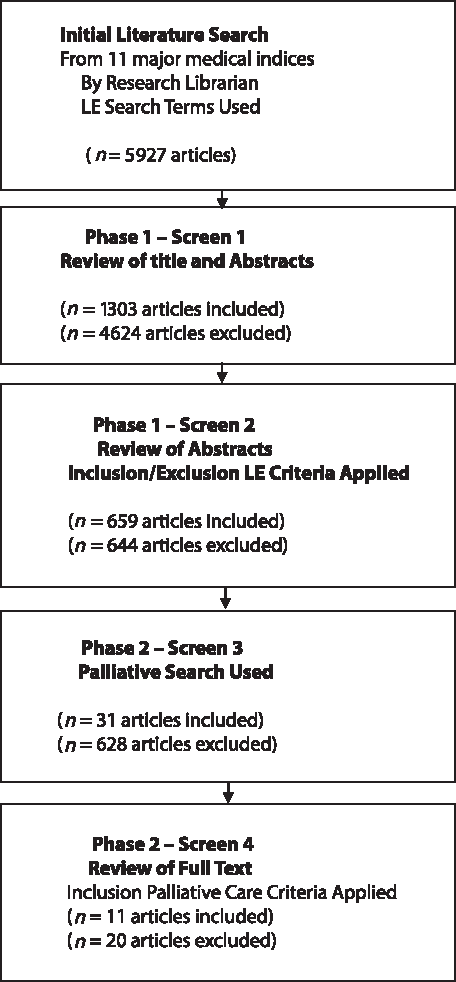
Literature review process for palliative care and cancer-related lymphedema systematic review (LE, lymphedema).
For the second phase, keywords for LE management in palliative care were applied (e.g., palliative care, advanced disease, and metastatic cancer). A total of 31 articles were selected and reviewed by the author team (screen 3). Inclusion criteria for the final review included randomized clinical trials, cohort studies, case-control studies, meta-analyses, and systematic reviews, pertaining to LE management in the setting of palliative care. Included studies had to have lymphedema as the outcome of interest. A total of 20 articles were excluded for the following reasons: abstract only (n=2); letter to editor (n=2); cross-sectional study (n=2); qualitative study (n=1); and general LE overview, not LE in palliative care period, and no intervention evaluated (n=13). The remaining 11 studies met the inclusion criteria (screen 4). Each article was summarized by one author and reviewed by other authors to ensure appropriate and accurate representations of the material. Each eligible study was rated in six categories according to the Putting Evidence into Practice® (PEP) classification of the Oncology Nursing Society (ONS) 27 : (1) recommended for practice, (2) likely to be effective, (3) benefits balanced with harms, (4) effectiveness not established, (5) effectiveness unlikely, and (6) not recommended for practice. The PEP classification system was chosen due to its high reliability and accessibility for evidence-based practice guidelines compared with other published rating methods. 28
Results
Based on the 11 articles meeting criteria for inclusion in this review (Table 1), all reviewed publications met the “effectiveness not established” category, as assessed by the ONS PEP classification. In addition, the authors identified four categories of LE management in the palliative care setting: (1) closed-controlled subcutaneous drainage studies, (2) MLD, (3) compression therapy, and (4) CDT.
Closed-controlled subcutaneous drainage
The use of closed-controlled subcutaneous drainage to manage lower limb edema in patients with advanced cancer was first reported by Clein and Pugachev 29 in 2004. In their study, a total of 8 patients with swelling of the lower limbs associated with various types of cancer (i.e., prostate, kidney, bladder, and melanoma) were treated with drainage by placing subcutaneous needles in the swollen legs, which drained into an enclosed bag, for a period of 12 hours to 1 week, depending on the volume of drainage. The results of the study showed that in seven of eight patients, there was objective improvement, as measured by the amount of fluid drained and the observed reduction in limb swelling. There were no adverse effects associated with the procedure such as infections, because sterile techniques were fully employed. In addition, the investigators reported that with this cost-effective procedure, all patients died in comfort. However, one of the limitations of this study is that objective limb volume assessment tools were not used.
In 2007, Faily et al. 30 applied this technique in a woman with ovarian cancer that had metastasized to the liver, anterior abdominal wall muscles, and lymph nodes. They inserted four subcutaneous needles in both swollen calves and thighs, which drained to a urine collection bag, for 2 and 4 weeks, respectively. The patient benefited from this procedure both physically and psychologically as a result of clinical improvement of limb swelling. The authors reported that the patient was very satisfied with the results achieved, as measured with the Edmonton Symptom Assessment Scale.
In 2009, two studies reported the use of closed-controlled subcutaneous drainage to manage lower limb edema in patients with metastatic colorectal cancer.31,32 Lam et al. 32 modified this technique by inserting two subcutaneous angiocatheters into the lateral aspects of the lower thigh and ankle in order to reduce the risk of infection, bleeding, and pain, in two patients with chronic lower limb edema. Over the course of 1 week, there was a notable reduction in thigh and calf girth. The protein level of the fluid drained was low and there were no subsequent skin infections. The authors claimed that this was the first report of the use of closed-controlled subcutaneous drainage in Hong Kong. However, it is difficult to generalize these results given that this is a small case study.
In the same year, Bar-Sela et al. 31 examined the use of this technique in eight patients with lower limb edema associated with various types of advanced cancer (prostate, lung, colon, stomach, and pancreas). In this report, subcutaneous needles were inserted into the inner and outer aspects of the ankles by creating subcutaneous tracts and attached to an enclosed drainage bag. All eight patients in this report were noted to have lost weight, ranging from 2–5 kg, after 24 hours. Five patients reported significant improvement in mobilization; however, objective evaluation tools were not utilized in this study.
Recently, Jacobsen and Blinderman 33 published a case study (n=2) to examine the use of subcutaneous lymphatic drainage for the palliation of severe refractory LE in cancer patients. In this study, six intravenous catheters were inserted around the patient's thighs and allowed to passively drain into a bucket on the floor without the use of drainage tubing for about 1–1.5 hours and repeated several times upon patient request. The patient experienced relief from the initial procedure and from the subsequent periodic drainage procedures, and there was a visible decrease in the area of swelling. The authors claimed that this procedure was easy to perform and well tolerated by the patient, as this approach avoided the use of indwelling catheters or tubing. However, the authors suggested that subcutaneous lymphatic drainage should be performed in carefully-selected patients, as those with chronic LE may have less accumulated subcutaneous fluid and be more susceptible to infection and poorer wound healing.
Manual lymphatic drainage (MLD)
One retrospective study was conducted to evaluate the effectiveness of MLD in the palliative care setting for advanced cancer patients with LE. 34 Of 208 patients, 90 with symptoms due to LE were included. Primary outcomes of the study included the reduction of pain intensity and dyspnea, and the reduction of LE and resultant functional impairment. When MLD was performed daily, patients experienced a significant decrease in pain intensity. Specifically, 94% of patients with pain reported a clinically-relevant reduction of pain intensity, and 73.9% of patients with dyspnea reported significant relief. However, four patients with neuropathic pain discontinued MLD due to pain experienced with MLD. In addition, 18.9% of the patients reported LE reduction as “little;” 64.4% as “moderate,” and 16.7% as “good.” Study limitations were its small sample size, lack of a control group for comparison, and the possibility of the influence of drug therapy on the intensity of pain and dyspnea prior to MLD. Two small case studies were conducted to evaluate the use of compression therapy in reducing LE for advanced cancer patients.25,26
Compression therapy: Multi-layer bandaging
In 2007, Pyszora et al. 25 conducted a case study (n=1) to evaluate the effectiveness of multi-layer bandaging and limb elevation in a patient with advanced cervical cancer and LE. The primary outcome was a reduction in swelling, as measured by circumferential measurements of the legs at four points: above the ankle, below the knee, above the knee, and below the buttock fold. The therapy consisted of multi-layer compression bandaging, limb elevation, and skin care. The results showed that edema was reduced by about 35% in both limbs. The patient was very satisfied with the results.
Compression therapy: Kinesio taping
A second case study was conducted by Pyszora et al. 26 in 2010 with the goal to examine the effectiveness of Kinesio® taping in reducing LE for a patient with advanced pancreatic cancer. The investigators applied the Kinesio tape to the lower leg of the patient with 15–25% tension for 3 days. Following treatment, the patient reported that swelling, pain, and the feeling of heaviness decreased. However, the small sample size and a lack of objective tools to measure the outcomes were limitations of the study.
Complete decongestive therapy (CDT)
Three case studies were conducted to test the effectiveness of CDT in managing LE in the palliative care setting.17,19,35 In the report by Hewitt et al., 17 two patients with advanced cancer (breast and lung cancer) and LE were treated with modified therapy, including multi-layer compression bandaging, exercise, MLD, and skin care as tolerated. Primary outcomes for the study included reduction of limb size and improvement of limb function. Both patients reported the reduction of limb size and the improvement of limb function.
Similarly, Towers et al. 19 treated three patients with advanced cancer (breast and prostate cancer) and LE with CDT and evaluated comfort, edema reduction, and improved function as rated by the patients as primary outcomes. The results showed that two patients received comfort and symptom relief until the end of life, and the last patient reported satisfaction with this treatment. Both studies have limitations in terms of small sample size and a lack of objective assessment tools.
Recently, Fenton 35 published a case study (n=1) to show the power of touch (MLD) or CDT in managing LE and fungating wounds for a patient with advanced breast cancer. Primary outcomes of the study included edema reduction, improved range of movement, and function. The results showed that CDT helped to increase range of movement and function. Patients perceived limb weight reduction, and the sense that LE was being controlled. In addition, the author also reported that with touch therapy, the patient reported feeling comfort and feeling intact and sensual up to the end of life. Study limitations were again the small sample size and lack of objective tools to measure the outcomes.
Discussion
Despite the limitations of the contemporary literature, closed-controlled subcutaneous drainage appears to be a potentially effective procedure for managing LE in patients with advanced cancer. However, these findings are based on small case studies and subjective outcomes. Using the ONS PEP classifications for assessing the weight of the level of evidence, the studies could only be classified as “effectiveness not established.” None of the studies reported any adverse effects such as infection; however, we recommend that this technique be carefully performed using sterile techniques. In addition, all of the procedures were conducted in the lower extremities and there is no reported protocol. Therefore it is difficult to generalize these results to the care of patients with upper extremity LE. However, these reports are promising and should encourage additional research to examine the effectiveness of this procedure using a standard protocol for the management of upper- or lower-limb LE.
In terms of MLD alone, there is only one report that used this strategy, which is also limited by a small sample size. Therefore, the current weight of the evidence for MLD in the palliative care setting was also rated as “effectiveness not established.” However, with respect to the human aspect, adapting MLD for patients with cancer-related LE in palliative care is important, because it not only assists to reduce swelling, but it also provides holistic care for these patients. 19 Therefore, more work with rigorous study designs and larger sample sizes to evaluate the effectiveness of MLD in cancer-related LE in palliative care is needed. In clinical practice, a consulting MLD specialist may provide recommendations for adapting MLD for individual patients with cancer-related LE in palliative care. 19
Compression therapy alone was also evaluated in two case studies with small sample sizes and a lack of objective tools to measure outcomes. These reports were also rated as “effectiveness not established.” With palliative bandaging, it is important to recognize that patients in palliative care may be unable to tolerate high compression pressure, and that bandaging may lead to undesirable adverse effects, such as pain, skin damage, or altered arterial circulation. Therefore it is suggested that fewer bandage layers and lighter compression pressure be encouraged for these patients. Guidelines for adapting compression therapy are outlined in the International Lymphoedema Framework and Canadian Lymphoedema Framework palliative care document. 23
Lastly, only three previous studies reported the benefits of CDT for palliative cancer patients with LE in terms of comfort, edema reduction, and function. However, the interpretation of these studies with small sample sizes must be considered carefully, because these results were measured using subjective self-reported data. Ideally, larger, well-designed, randomized-controlled trials are recommended to confirm whether or not CDT is effective to manage LE for palliative cancer care. Ethically, it may be difficult to obtain informed consent for clinical research being conducted in advanced cancer patients with LE, and professionals may need to consider the primary goals of palliative care for advanced cancer patients with LE. Previous clinicians have asserted that, “For patients with advanced disease and LE, the optimal goal is to improve patient's quality of life, rather than to resolve the swelling completely.”20–23 Accordingly, the outcome measures of LE treatment in the palliative care setting should focus on improving patients' quality of life, rather than the absolute reduction of swelling. Towers et al. 19 pointed out that although objective outcome measures, such as circumferential measurement, may be generally useful as an assessment tool, it is less beneficial for cancer-related LE patients in palliative care. It has been suggested that a log of activities of daily living and symptom measures are more likely to be useful.
In conclusion, there is a paucity of rigorously conducted comparative clinical research studies pertaining to the treatment of lymphedema in patients with advanced cancer. In order to provide evidence-based practice guidelines for this population of patients, it is critical to design and test these strategies using relevant patient-reported outcomes. In general, the case studies reported that all of the procedures, including closed-controlled subcutaneous drainage, MLD, compression, and CDT, are relatively safe and may be considered in individual patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.