
Abstract

Dear Editor:
Palliative care grew out of, and is often only associated with, end-of-life care. With the demonstrated power of the clinical interventions, there has been a shift toward initiating earlier in the course of illness, when disease-directed therapies are still effective. We think this development challenges the common tag line of “transition from cure to comfort” to a tag line, “the cure and comort model.”
Palliative care is one of the most significant and fastest growing fields in Medicine in the United States. Compared to 2000, there has been a 96% increase in palliative care programs in hospitals with more than 250 beds. 1 Hospice and palliative medicine was recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME) in 2006.
Along with the growth of the field, there has been a gradual shift in the philosophy of care as well. The field has been characterized by some as an expansion of hospice care into the hospital with a focus on care for patients at the end-of-life while in the hospital and their transition out to home hospice care. In 1990, the World Health Organization (WHO) published the diagram shown below (Fig. 1) depicting the increasing role of palliative care in cancer patients with disease progression. It must be noted that most medical conditions like dementia, heart failure, chronic obstructive pulmonary disease (COPD), incurable cancer, etc., fit the description of the WHO figure. Historically, cancer is the diagnosis that is most often associated with palliative care. This is reflected by the fact that most of the patients admitted to hospices have a diagnosis of cancer. 2
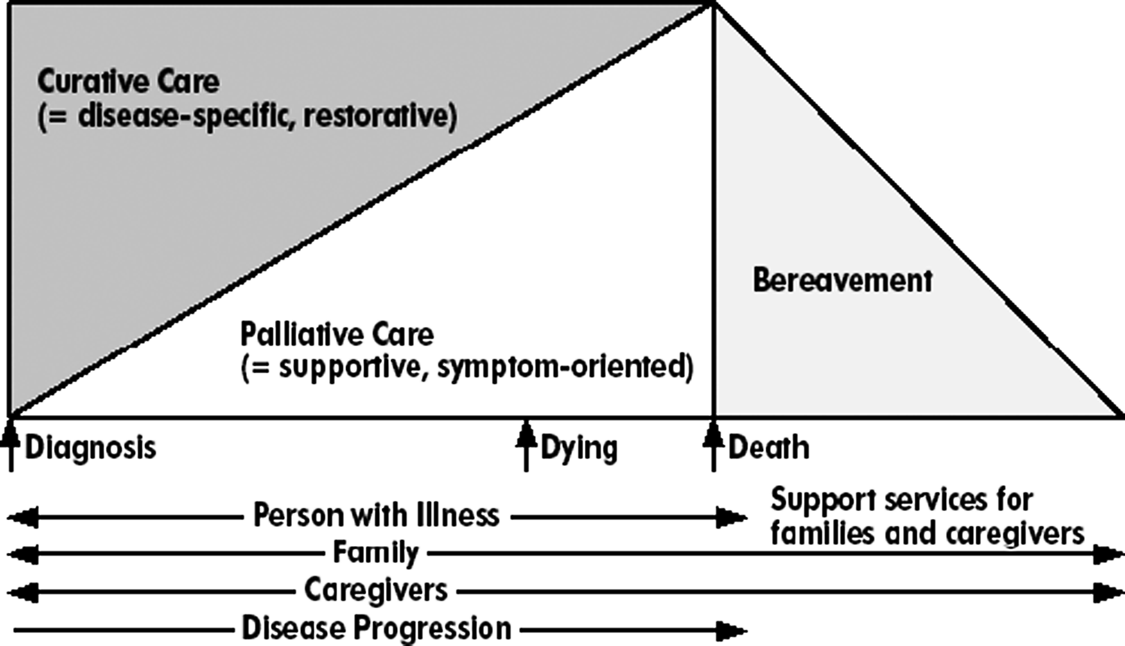
World Health Organization (WHO) model of palliative care.
A frequently used modification of this diagram is depicted in Figure 2. The rectangle at the far right represents the last 6 months of a terminally ill patient's life and is ideally under the care of hospice. The vertical line depicting transition onto hospice is traditionally describes as “the wall.” The patient often has to give up certain treatments to make the jump. Quite often the choices are presented as comfort or cure.
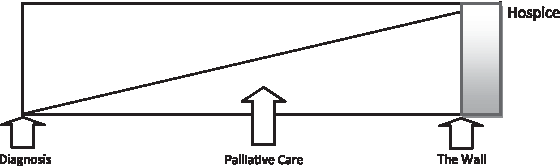
Comfort or cure model.
In 2002, WHO modified its definition of palliative care to add “is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.” 3 The Center to Advance Palliative Care (CAPC) has on its public website a description of palliative care that clearly states the following: “It is appropriate at any point in a serious illness and can be provided at the same time as treatment that is meant to cure.” 4 Thus seen is an evolution in the concept of palliative care.
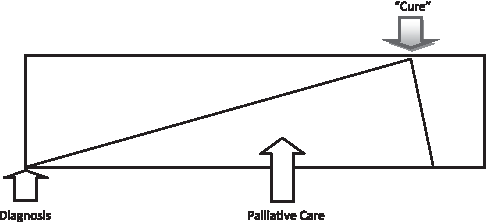
At Cedars-Sinai Medical Center, we have had experience with early involvement of palliative care. Palliative care has been involved with care of patients with stage D heart failure. The involvement is not limited to patients who have exhausted all treatments and are then waiting to succumb to their disease process. Some of the patients seen by the service have received heart transplants with the palliative care service being involved before and after the surgery. Others have received a ventricular assist device (VAD) as a bridge to transplant or destination therapy. Few of these patients receive end-of-life care and hospice care. Thus palliative care covers the whole spectrum of outcomes from a successful transplant to end-of-life care. We depict our experience in a modification of the WHO diagram to the one shown below (Fig. 3). The diagram depicts the involvement of palliative care in our patients who have received heart transplants. We call the change in the direction of disease progression from worse to better after the transplant “the bend.” It is noteworthy that the line depicting level of palliative care involvement for symptoms/support does not return to baseline after transplant as there is morbidity involved post transplant and the patient's life is never back to baseline.

Comfort and cure model in transplant patients (e.g., heart and kidney).
The Palliative Care Service has experienced significant growth in both depth and breadth of scope within the Cedars-Sinai Medical Center. In addition to involvement in patients needing end-of life care, and heart failure patients, a palliative care consultation will be part of the standardized admission orders for patients who are admitted to the hospital for a bone marrow transplant (BMT). Similar to the heart failure service, patients who have received successful bone marrow transplants have been followed by the team prior to the transplant being initiated. The involvement of the palliative care service augments the integrative team care received by these patients. Furthermore, the palliative care team has been invited to be part of the multi-disciplinary screening process for BMT eligibility. A subset of this patient population undergoes an autologous stem cell transplant and thus achieves a true “cure” with the expectation of little or no associated morbidity after the transplant if successful. In this patient population we have modified the WHO diagram as below (Fig. 4).
Comfort and cure model in autologous bone marrow transplant patients.
There is an increasing body of evidence that indicates that involvement of palliative care not only improves quality of life but also prolongs life as well.5,6 With the experiences at our institution, we have successfully shown the shift from the “comfort or cure” model to the “comfort and cure model.” We strongly make the case for palliative care being involved in the care of patients irrespective of the treatment paths they select. We make the case that involvement of palliative care in the treatment of patients not be an option, but instead a standard of care irrespective of the treatment paths chosen.