
Abstract

Dear Editor:
The Republic of Georgia, formerly one of the members of the Union of Soviet Socialist Republics (USSR), has a population of about 4.5 million citizens. About 1.2 million live in the capital city. The rest live in small towns and mostly rural areas in 11 regions of the country. The situation in Georgia is representative of the challenges to development of palliative care in many countries around the world. First, economically speaking, it is a developing country with an economy in transition. Consequently, there are serious limits to the amount of money that can be spent on health care. Second, it has a national health system that must provide care to citizens throughout the country. Third, it is facing a changing demographic where its population is living longer because of improvements in public health and sanitation. For all the reasons that palliative care makes sense in developed countries, it makes even more sense to incorporate it into the health systems of developing countries. The purpose of this letter is to summarize a simple educational approach that proved pivotal in the Republic of Georgia.
Background
In 2003–2004, we found that 83% of representatives from national governmental structures, decision makers and stakeholders failed to understand the role of palliative care in a national health care system. Consequently, any meaningful decisions for political approval of strategy, finance, needed human resources, drug availability, and the practical implementation of palliative care were not possible. The results were also consistent with prevalent cultural norms in the country. First, talking about the diagnosis of cancer is taboo. Second, laws and standards inherited from the Soviet period for the prescription and dispensing of opioids are consistent with opiophobia. Third, the health system has been free of charge to all citizens, but is of low quality. Consequently, there wasn't a belief that it is possible to develop a service with real benefit that is also cost-effective. Even the “customers” of palliative care, the patients and their family members, did not comprehend what palliative care can do for them. Our conclusion from this period of assessment was that in any country/society, including Georgia, successful implementation of palliative care can never be successful without the support of potential consumers on the one hand, and health care system managers, on the other. We had to develop a strategy that would simply and convincingly make the case for palliative care in a country like Georgia.
Overcoming Barriers through Education
We condensed and simplified information about palliative care and its significance for the public in Georgia and presented it to key representatives of the constituencies identified during our initial assessment. The information answers two questions:
What does palliative care mean for our country?
The population of every country generally can be divided into three main groups: “Healthy People,” “Potentially Treatable Patients,” and “Advanced Chronic Patients.”(See Fig. 1.) Consequently, a centrally planned health care system will want to develop three principal directions:
Prevention (aimed at healthy people), intending the maintenance of healthy status and decreasing morbidity and mortality;
Curative (for potentially treatable patients), aimed at the patient convalescence and rehabilitation for return to a normal productive life;
Palliative (for Advanced Chronic Patients), intending the maintenance of maximally available life quality.
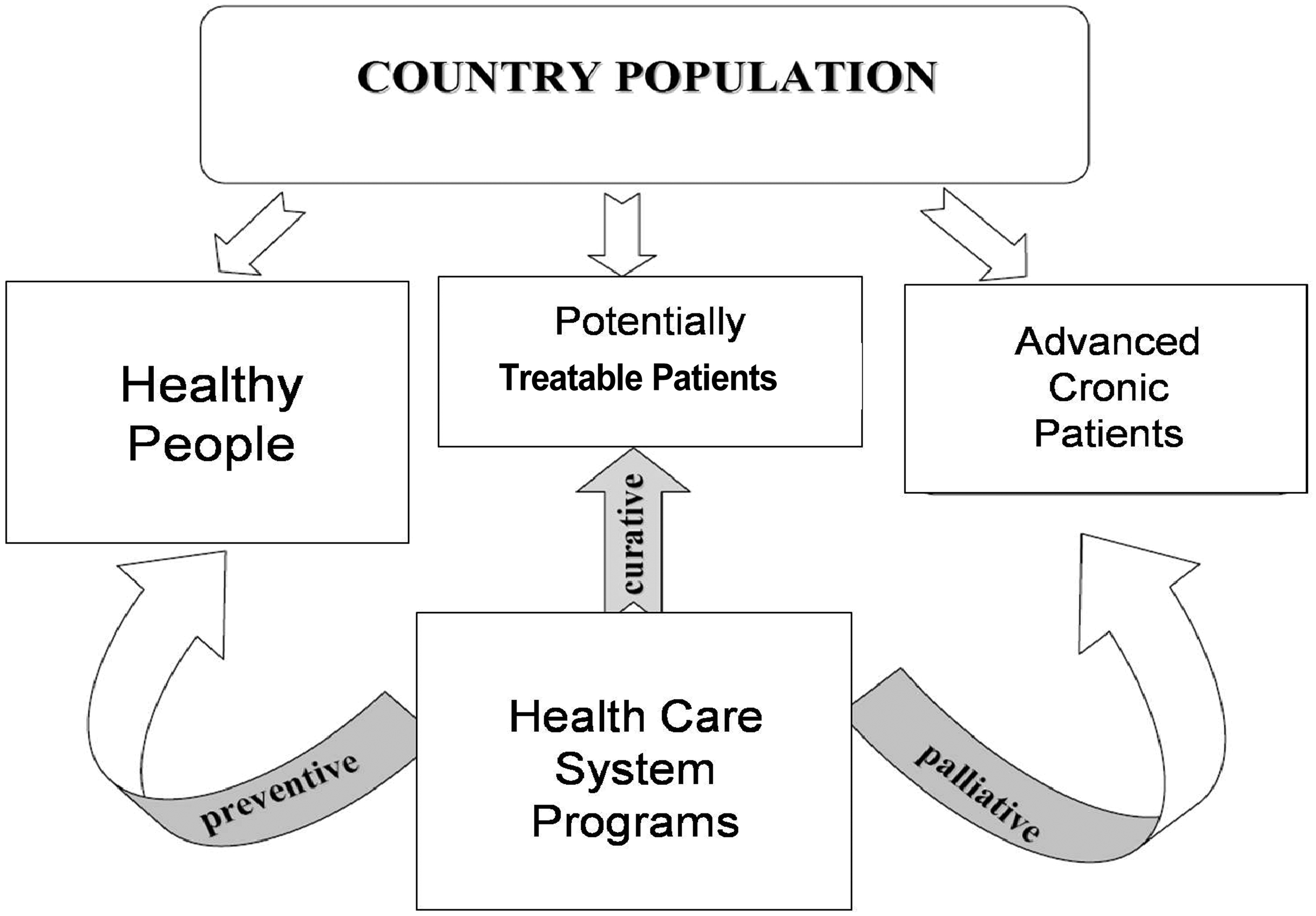
Three groups of population according to health state.
If any of the listed directions is omitted, the health care system cannot be considered complete because a significant part of the society becomes deprived of the health care service. Similarly, if inappropriate strategies and methods are used (e.g., incorrectly planned and performed preventive programs fail to avoid and/or effectively prevent the development of certain diseases), there is a fundamental failure of the health care system. It follows that incorrect, incomplete, or inadequate palliative care will lead to a similar failure of a fundamental role for a national health care system.
What does palliative care mean for a patient with advanced illness?
Each of us has countless wishes and possibilities we want to realize through our lifetime. These possibilities are shown in the largest circle in Fig. 2 (“Overall Life Possibilities”).
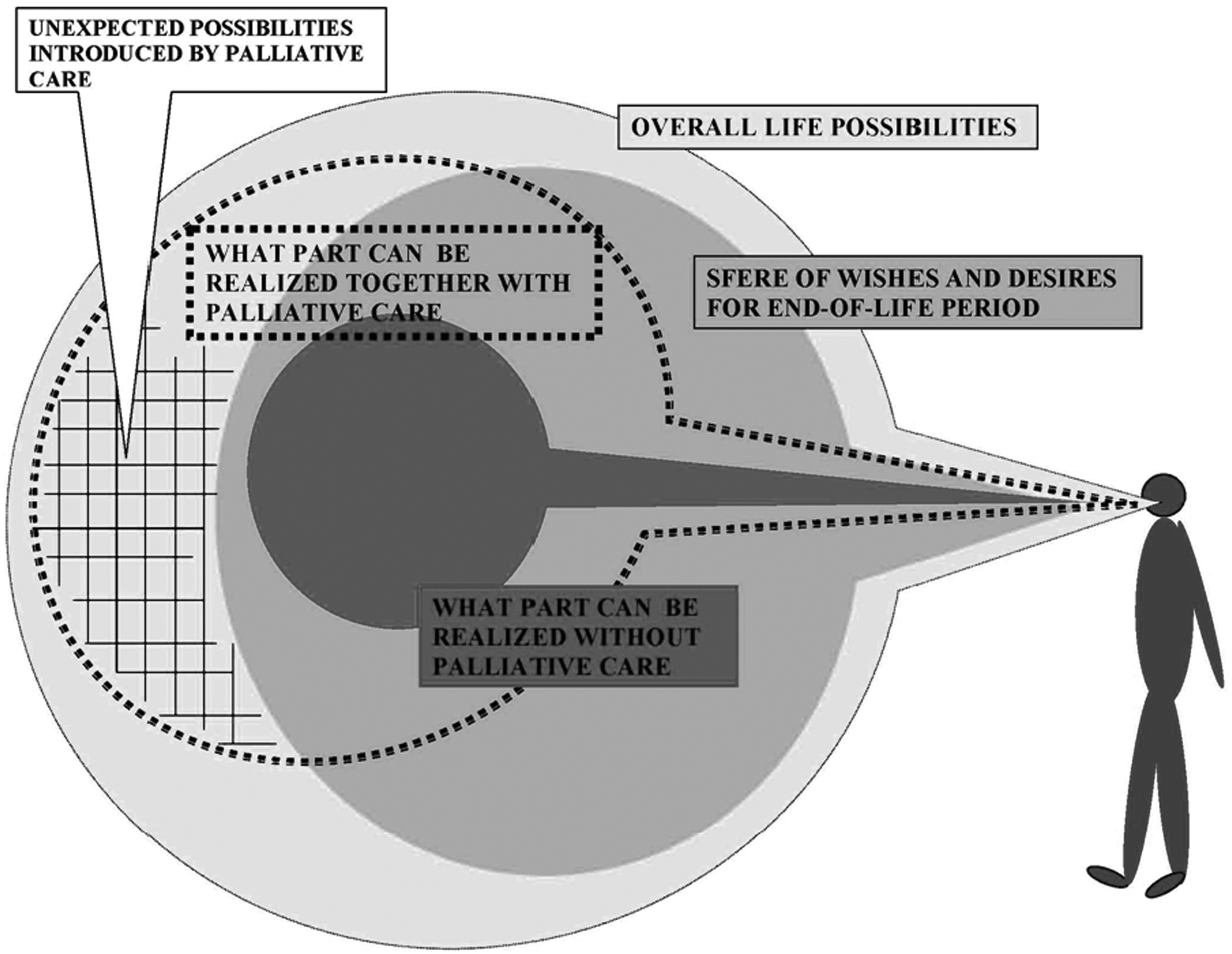
Life wishes and possibilities.
This circle involves wishes and possibilities such as love, marriage, health, friendship, journeys, sport, art and creativity, safety, comfort, wealth gaining, rest, etc.…
In the setting of chronic incurable illness, the circle of wishes and possibilities gets smaller for advanced chronic patients. A person and his or her family changes plans and concentrates on desires such as peaceful family life, rest, safety, comfort, and freedom from pain and other complaints. This condition is depicted in the mid-sized circle, “Sphere of Wishes and Desires for End-of-Life Period.” Unfortunately, uncontrolled pain and numerous annoying and distressing symptoms prevent the realization of even those limited wishes, which had been planned for the end of life. These severely limited possibilities are depicted in the third, smallest circle: “What Part Can Be Realized without Palliative Care.”
Comprehensive palliative care is the tool for relieving pain and different distressing symptoms (nausea, vomiting, cachexia, bedsores and pressure ulcers, constipation or diarrhea, etc.) and for achieving maximal comfort. It enables the patient with advanced disease to make the rest of his or her life biologically and socially active, surrounding the patient by the atmosphere of not only medical but also social and spiritual support. In other words, palliative care is a proven approach to the widening of the realm of the patient's possibilities. This reality is shown in Fig. 2 by the circle drawn with the dashed line. There should be nothing surprising in the fact that the limitation of possibilities for patients with advanced chronic illness near the end of their lives is wider with palliative care compared with a life without palliative care, if not given the following circumstance: a dotted area on the diagram with the title, “Unexpected Possibilities Introduced by Palliative Care.” It should be apparent that the comfort provided by comprehensive palliative care can be so significant, that possibilities for advanced chronic patients become a fascinating surprise they could never have been imagined to be possible.
A verse by the famous Georgian producer, poet, and translator Revaz Tabukashvili—“To my grandsons, Rezo and Bombo”—was written by the author, who was suffering from incurable illness, the day before his death. The poem became his last will not only to his grandsons, but to the entire Country of Georgia. The comfort provided by pain relief and symptom control brought him back the endurance and inspiration of creator once more, and enabled him to light the final days with this masterpiece. This easily understood case example helps the country to understand the benefits of palliative care.
The question, “What does palliative care give a person?” can be answered simply with the following two words: unexpected possibilities. We should not permit anyone to miss a chance to share these unexpected possibilities, even by the end of life. We must heed the old Greek byword: “I feel unexpectedness—that means I live.”
Outcomes from Education
The items in the following list of achievements are measures of the effectiveness of the educational campaign based on these two simple diagrams:
Adoption of amendments to existing federal laws of Georgia establishing the necessity of palliative care as an integral part of the national health care system;
Approval of basic clinical guidelines for palliative care and liberalized opioid prescription regulations by order of the Minister of Labor, Health, and Social Affairs of Georgia;
Importation of oral morphine;
Establishment of the Office of Coordinator of National Program of Palliative Care at the Committee of Healthcare and Social Issues of the Parliament of Georgia;
Implementation of palliative care curricula in the universities and several colleges of medical education;
Two physicians sent for palliative medicine training abroad in a program specifically designed to help them lead new demonstration clinical programs in palliative care that will, in turn, train others for service in the country;
Launching of the Home-based Palliative Care mobile teams and Inpatient Units for Advanced Patients in several towns and regions of Georgia (financed by governmental budget and Global Fund (for HIV/AIDS patients);
Compilation of Georgian handbooks for doctors, nurses, and medical students;
Launching the educational/training courses for health care professionals (in cooperation with international faculty);
Launching a program of research in palliative care (funded by OSGF and GNSF grants);
Setting up an international cooperative network (OSI, IPMatSDH, CEH and Hungarian Hospice Foundation, HtH, ESMO, etc.).
In summary, two simple diagrams proved to be the basis for an effective education campaign with the key decision makers for a national health care program that provided the basis for implementation of initial clinical programs. We think that other countries could use these same diagrams for the basis of a similar outcome.