
Abstract
Abstract
Background:
In this single-site study, we evaluated the feasibility of a parent-clinician communication intervention designed to: identify parents' rationale for the phase I, do-not-resuscitate (DNR), or terminal care decision made on behalf of their child with incurable cancer; identify their definition of being a good parent to their ill child; and provide this information to the child's clinicians in time to be of use in the family's care.
Methods:
Sixty-two parents of 58 children and 126 clinicians participated. Within 72 hours after the treatment decision, parents responded to 6 open-ended interview questions and completed a 10-item questionnaire about the end-of-life communication with their child's clinicians. They completed the questionnaire again two to three weeks later and responded to three open-ended questions to assess the benefit:risk ratio of their study participation three months after the intervention. Clinicians received the interview data within hours of the parent interview and evaluated the usefulness of the information three weeks later.
Results:
All preestablished intervention feasibility criteria were met; 77.3% of families consented; and in 100% of interventions, information was successfully provided individually to 3 to 11 clinicians per child before the child died. No harm was reported by parents as a result of participating; satisfaction and other benefits were reported. Clinicians reported moderate to strong satisfaction with the intervention.
Conclusion:
The communication intervention was feasible within hours of decision making, was acceptable and beneficial without harm to participating parents, and was acceptable and useful to clinicians in their care of families.
Introduction
The study proposed to assess the feasibility of a parent-clinician end-of-life communication intervention. Interventions were to provide clinicians with parents' statements of understanding about the end-of-life decision made, the options they considered, their rationale for the option chosen, and their definition of being a good parent to their seriously ill child. The study sought to determine the clinician behaviors that could help parents to achieve their definition of being a good parent. Assessment was made of parents' perceptions of the acceptability and clinicians' of the usefulness of the intervention. The study was guided by the Pediatric Quality of Life at End-of-Life model. 15 This model includes factors that influence parental understanding of their child's transition to end of life, including information from trusted clinicians, the parents' definition of being a good parent to their ill child, the child's apparent symptoms and altered physical appearance, and information indicating that no scientific advances remain to help their child survive the illness.16–18
Methods
Inclusion criteria for parents were the following: the parent of a child with incurable cancer receiving care at the study site who had participated in making a decision within the previous 72 hours about either (1) enrolling the child on a phase I experimental agent study, (2) initiating a do-not-resuscitate (DNR) order, or (3) ceasing disease-directed treatment and initiating terminal care; at least 19 years of age; English-speaking; and willing to give written consent. Parents were ineligible if their child's physician, nurse, or psychosocial team expert (social worker, childlife worker, psychologist) identified them as being emotionally or mentally unable to participate in an informed consent process or likely to find the study to be too burdensome because of their emotional or mental state.
Inclusion criteria for clinicians (i.e., attending, fellow, registered nurse, advanced practice nurse, pharmacist, social worker, child life worker, nursing care assistant) included the following: directly involved in the care of the child for whom an end-of-life treatment decision had been made in the previous 72 hours, English-speaking, and willing to give written consent. Parents were enrolled only once, but clinicians could be enrolled multiple times during the study period if parents of their other patients became eligible for the study.
The study had a single-site, feasibility, pre-post communication intervention design. The design had five data-collection time points (see Fig. 1):
T1: Parent eligibility was confirmed, and parents were informed of the study's purpose. T2: Study forms were completed during face-to-face interviews with parents. T3: Clinicians completed a baseline questionnaire about the decision. With parental permission, the parents' interview responses were then disseminated to available clinicians orally by the study team member, and the written interview was then placed in the child's medical record to provide access to all involved clinicians. T4: Clinicians' perceptions of acceptability and usefulness of the communication intervention were solicited approximately three weeks after they received the parent interview information. T5: Parents' perceptions of the communication intervention and study participation were solicited approximately 12 weeks after their participation in the study.
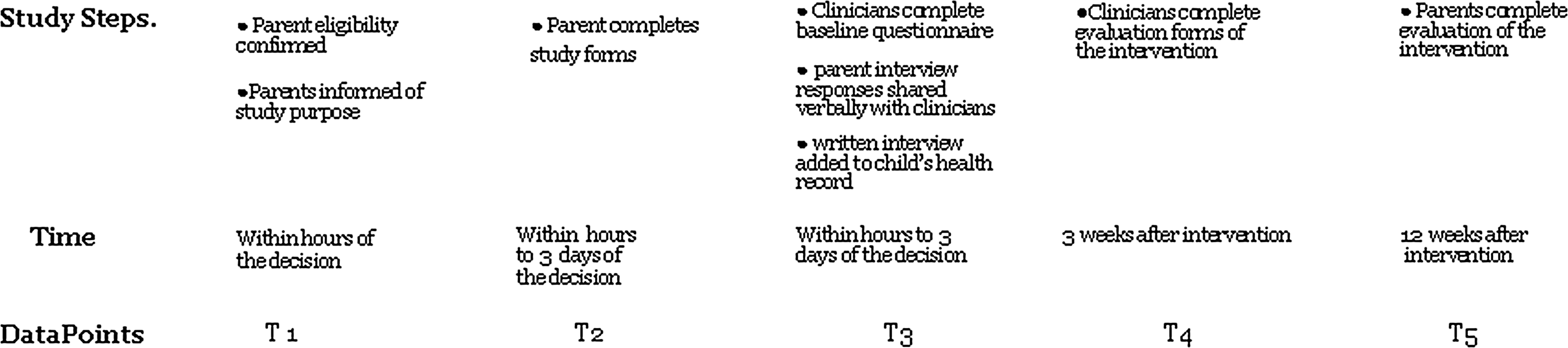
Study Design Schema (T1 – T5).
End-of-life decisions were identified during daily clinical rounds by a study team member from each clinical team, review of daily physician documentation and orders in high acuity clinical areas (intensive care unit, bone marrow transplant unit), and by electronic notification from the central protocol and data management office when patients were enrolled in a phase I study. Parent eligibility was then confirmed individually by the attending physician, a psychosocial expert, and a nurse. If the three sources disagreed, then the study team asked them to discuss their opinions and render a final decision about parent eligibility. Five disagreements occurred and were resolved after discussion with the involved clinicians.
The intervention (T2) included the study team member administering the Parent Perceptions of End-of-Life Communication with Staff Form to each participating parent. This form, developed for this study, is composed of 10 items from the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT) Study
19
and the Satisfaction with Decision Instrument
20
and 2 additional items related to parents' perceptions of achieving their definition of being a good parent to their seriously ill child. The second form administered to each parent was the Parent-Clinician Communication Form at the Time of Difficult Decision Making, a 6-item interview guide composed of 4 previously tested questions in end-of-life decision-making studies and 2 additional questions about being a good parent at the end of life.1,21,22 The basis of the questions was explained to each participating parent. The interview questions were:
1. Please tell me in your own words what the treatment decision was that you helped to make for your child. 2. Please tell me the options that you considered when you helped to make this decision. 3. Please list who was in the room with you when the decision was made. 4. Please tell me about your reason/s for choosing this option. 5. Please share with me your definition of being a good parent for your child at this point in your child's life. 6. Please describe for me the actions from staff that would help you in your efforts to be a good parent to your child now.
Clinicians completed a 6-item questionnaire, Staff Perceptions of End-of-Life Communications, at T3 and T4. Four items had response options of “rarely,” “almost half the time,” and “almost always;” 2 items had “agree/disagree” response formats. At T4, clinicians responded to 6 additional items about their recall of the information shared during the communication intervention and their perception of the usefulness of that information; they also answered the open-ended question, “How did the information influence your practice or your interactions with this family?”
At T5, parents were asked three questions during a telephone follow-up contact initiated by a study team member who was not a part of the intervention:
1. What was good about being in the study? 2. What was bad about being in the study? 3. What else would you like us to know?
Statistical considerations
The study definition of feasibility was at least 60% of eligible parents would consent to participate and at least 60% of participating parents and their child's clinicians would be able to complete the communication intervention before the child died. Parent and clinician responses to the questionnaire items were analyzed using descriptive statistics. Change in the parent scores was not assessed because of the high (ceiling) scores of satisfaction at both measurement points. Change in clinician scores on the Staff Perceptions of End-of-Life Communications Questionnaire was assessed at the individual item level using percent change and the Kappa statistic of agreement. Two members of the study team independently rated the clinician responses for recall accuracy of the parent interview data, and percent agreement was subsequently calculated. Two team members independently rated the clinician responses to the open-ended question to achieve a minimum of 80% agreement with coding of the clinician responses.
Results
During the 22-month study enrollment period, 232 eligible end-of-life decisions were identified at the study setting. Of these, 91 (39.2%) decisions were identified after the family had exited the study site to return to their homes and had no return appointment planned (see Fig. 2). Sixty-six decisions were ineligible with the two most common reasons being clinician perception of the parent being too vulnerable to participate (n=27) and the parent being non–English speaking (n=24).
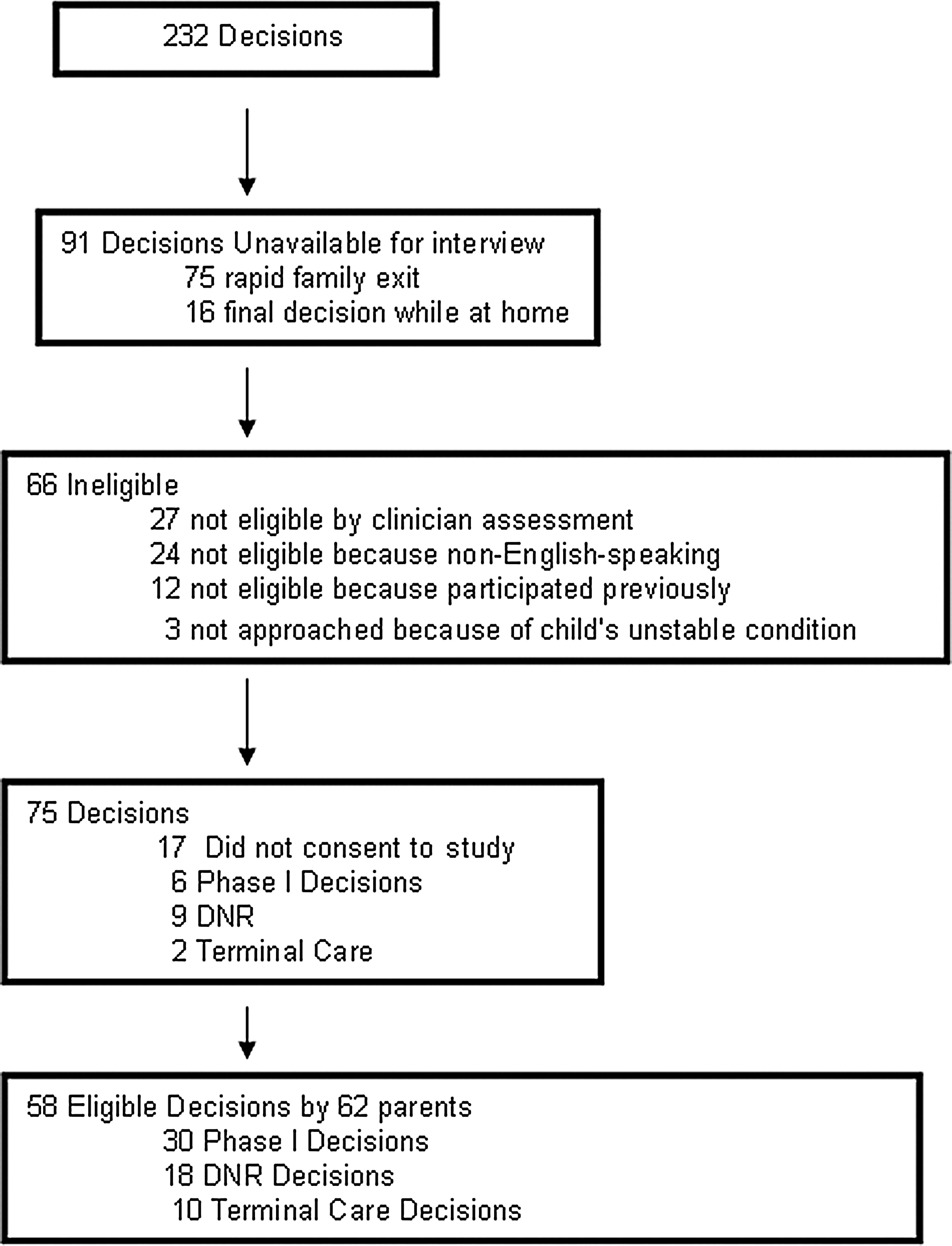
Study Enrollment.
Parent participation rates
Of the 75 eligible families, 62 (77.3%) parents of 58 seriously ill children enrolled in the study (see Table 1), and 17 parents (21.5%) declined. Of the 17 parents who declined, 9 (52.9%) had made a DNR decision; 6 (35.3%), a phase I decision; and 2 (11.8%), a terminal care decision. The primary reasons for refusal were “no time now to participate” (n=8), with 3 families asking to participate after they had returned to their homes, and “too hard to do this now” (n=5).
DNR, do not resuscitate; sd, standard deviation
Clinician participation rates
Of the 139 clinicians involved in the care of eligible families, 126 (90.6%) enrolled in the study; the rest declined to participate. The primary reason for clinician refusal was “not sure what to do with the information that would be made available to me” (n=7). Clinicians participated 1 to 10 times in the study, with the majority of clinicians (88.9%) participating 1 to 3 times. Altogether, the 126 clinicians provided 253 reports at T3 and 215 reports at T4. Only the clinician reports available at both T3 and T4 (n=215) were included in the analysis. The clinicians providing those reports were nurses (n=106, 49.3%); psychosocial experts (n=38, 17.7%); physicians (n=22, 10.2%); nurse practitioners (n=18, 8.4%); nursing care assistants and unit coordinators (n=13, 6.1%); fellows (n=11, 5.1%); and others (pharmacists/physician assistants/volunteers) (n=7, 3.2%). No family withdrew from the study. Additionally, the communication intervention was fully delivered to each participating parent and clinician before the child's death. These findings support the feasibility of the communication intervention being delivered within 72 hours of an end-of-life treatment decision.
Parent and clinician satisfaction with the end-of-life communication intervention 2 to 3 weeks after the intervention
Parent-matched reports at T2 and T4 (n=46) were included in the analysis of satisfaction with end-of-life decision making. Of the 10 items reported, 6 were at 97.8% to 100% agreement at T2; all 10 items reported at T4 were at 95.7% to 100% agreement, indicating that overall parent satisfaction with end-of-life decision making and with clinician support for decision making remained high three months after the intervention. Five parents at T2 indicated agreement with the item, “If the staff had told me more about my child's condition, I would have made a different decision about my child's care.” Of these parents, three had enrolled their child in a phase I trial, and two had made a DNR decision. Only two of these parents gave the same response at T4.
Clinician-matched reports at T3 and T4 (n=215) were included in the analysis of satisfaction with the communication intervention. All item ratings improved slightly from T3 to T4 (improvements ranging from 1.9% to 11.6%). When the clinician responses to the items are considered by type of decision, the improvements are larger for the phase I and DNR decisions than for the decision for terminal care (data not shown). The item across all decisions that received the lowest clinician ratings and smallest Kappa coefficient was, “Documentation about end-of-life decisions is adequate.” The item with the highest percent of “almost always” responses and the largest Kappa coefficient (0.6014) was, “It is easy for me to talk openly with nurses on my team about end-of-life decisions for our patients” (see Table 2). Nursing assistants and unit coordinators (n=13) reported having the least access to information about end-of-life decision making and the least involvement in the decision-making process; physicians reported having the most access and involvement. In terms of change between T3 and T4 by discipline, the more positive scores were reported by nurses and psychosocial experts (data not shown).
T3, third data point; T4, fourth data point
Of the 215 clinician reports at T4, 72.6% were a complete or a partial match as determined by the two independent raters of the parents' rationale for the end-of-life decision made; and 66.1% of the reports were a complete or a partial match with the parents' definition of being a good parent (see Table 3). Ninety-three clinician reports (43.3%) indicated that knowing the parents' perceptions of the end-of-life decision improved their interactions with the parent. Additionally, clinician responses to the query about how the interview information influenced their practice or interactions with the family were categorized into five categories, with the largest category being “my professional interactions with the parent/s improved” (n=75) (see Table 4). Finally, 29.3% of the clinician reports indicated that having the information in the communication intervention helped to reduce tension among clinicians about end-of-life decision making. Field notes of spontaneous comments made by clinicians indicated that 43 reported that no tension around the decision existed and, therefore, no reduction of tension was possible.
T4, fourth data point
The majority of parental responses (87.5%) to the follow-up question at T5 about what was good about being in the study were related to “helping others.” The most frequent parent response to the question about what was bad about being in the study was “nothing” (89.2%). Two parents (4.3%) reported negative aspects: inappropriate timing of being informed about the study (n=1) and participating triggered a reliving of the end-of-life decision making (n=1). The most frequent parent response to the interview question about what else parents wanted clinicians to know was “nothing else” (65.3%) (see Table 5).
T5, fifth data point
Discussion
Although the number of refusals was small, the refusals occurred more often in the resuscitation decision category than in the phase I decision category. This trend may reflect the number of families in the resuscitation category who wanted to exit the study setting quickly to take their child home.
Having a mechanism by which to provide information about end-of-life decision making could be a helpful clinical tool for clinicians caring for the family members making such decisions. However, the extent to which these discussions are documented in the medical record varies and can be limited by the type of decision made. 23 End-of-life documentation has typically been studied by reviews of medical records. In two such studies, 35% to 40% of eligible medical records had incomplete or missing documentation about end-of-life decisions, making these records inevaluable.24,25 In another study, documentation was described as fragmented and inconsistent. 26 Furthermore, many clinicians in our study commented that they would not have had access to such information without our intervention.
Clearly, standard documentation in the medical record does not sufficiently help clinicians understand end-of-life decisions. In other studies, specific order forms designed to communicate a treatment-limitation decision to clinicians have been described by clinicians as significantly improving the clarity of written orders and the communication between clinicians, family members, and other clinicians. 27,28 The parent interview tool we used served as a similarly simple communication tool and provided the parents' own words about the decision, their rationale, and their definition of being a good parent at the end of their child's life—as well as suggesting actions clinicians could take to help parents fulfill that definition.
Clinician-reported usefulness of the communication intervention included four categories that reflected an increase in clinician understanding of the family's reasons for the end-of-life decision making. These clinician-reported categories directly address previously published concerns from clinicians about discussing end-of-life decision making and care for a child with incurable cancer, indicating that the parent-clinician intervention improves parent-clinician interactions and communication.29–31 The second largest category, “nothing changed,” contained responses indicating that clinicians either did not allow the information to affect their interactions with the parents or had no opportunities to use the information. The study team noted in some clinicians' verbal responses a seeming sensitivity to the interview question, as if they interpreted the question as implying that their practice or interactions with parents needed to improve. For future studies, we will revise this question, using more neutral wording.
Three families who participated in the study contacted the study team when a second end-of-life decision was made and asked to participate again because of the benefit of participating the first time. This unexpected experience suggests that some parents would consider being part of a longitudinal prospective study, allowing the study of parents' perspectives over time and decisions. Our findings also indicate that only a minority of parents are perceived by clinicians as being too vulnerable to participate in a communication intervention study after an end-of-life treatment decision has been made; thus, clinician protection of parents is not a central barrier to this kind of intervention. Limitations of our study include having only a small number of fathers in the sample and inflexibility of the method, as only parents available for face-to-face interviews and who were English speaking were eligible.
A parent-clinician communication intervention within 72 hours of end-of-life decision making on behalf of a child with incurable cancer is feasible, acceptable, and beneficial without harm to participating parents. Such intervention is also acceptable and useful to clinicians directly involved in the care of the seriously ill child and family. The focus on the good parent concept proved to be a positive aspect of the communication intervention for the participating parents and was used by some participating clinicians in their clinical care interactions with the parents.
Footnotes
Acknowledgments
The findings reported here have not been previously presented; however, previously published in the Journal of Clinical Oncology was a related aspect of the conceptual definition of being a good parent to a seriously ill child. 2 This research was supported in part by Grant No. R21 NR008634 from the National Institute of Nursing Research, Cancer Center Support Grant No. P30 CA21765 from the National Cancer Institute, and by the American Lebanese Syrian Associated Charities.
Author Disclosure Statement
No competing financial interests exist. None of the authors have any actual or potential conflict of interest to disclose.