
Abstract
Abstract
Background:
Agitated delirium is often observed in terminal patients with cancer. To clarify the risk factors for agitated delirium in terminal patients with cancer, we conducted a retrospective chart review of 126 patients with cancer who died at a university hospital in 2008.
Method:
As a working definition, we define agitated delirium as a score of 2 or more in item 9 of the Memorial Delirium Assessment Scale with diurnal variation.
Results:
The results were as follows: agitated delirium was observed in 49 (42%) of the 115 patients, and it occurred within the last week before death in 49% of the patients. Univariate analysis revealed older age, male gender, smoking history, lung cancer, diabetes, and high C-reactive protein (CRP) value as major risk factors, while dendritic analysis revealed lung cancer, high CRP value, diabetes, older age, and smoking history as key factors for predicting agitation.
Conclusion:
It is necessary to consider risk factors in order to categorize terminal patients with cancer into high- and low-risk groups and undertake possible counter-measures.
Introduction
Methods
We conducted a retrospective chart review of patients with cancer who were aged 16 years or older and who died at Osaka University Hospital between January 1, 2008 and December 31, 2008.
We assessed the demographics, the presence of agitated delirium, the laboratory results, the administration of therapeutic drugs, and their effects in these patients.
Identification of patients with agitated delirium from medical records
Psychomotor activities of delirium symptoms were assessed with item 9 on MDAS and classified into 4 grades (0, normal psychomotor activity; 1, mild psychomotor activity; 2, moderate psychomotor activity; and 3, severe hyperactivity). We identified agitated delirium in patients when the score on item 9 of the MDAS was 2 or more and it showed diurnal variation. Patients were divided into the agitated delirium and nonagitated delirium groups.
Investigational items for the identification of risk factors
We compared age, gender, body mass index (BMI), smoking history, drinking habits, primary site of cancer, site of metastasis, complications other than metastasis, and laboratory test values (glomerular filtration rate [GFR], white blood cell counts, C-reactive protein [CRP] levels, albumin levels, platelet counts, aspartate amino transferase levels, and alanine transaminase levels) between the agitated and nonagitated delirium groups. On the basis of patients' statements regarding their smoking and drinking habits, we determined their smoking history and daily consumption of alcohol (excluding occasional consumption). With regard to the laboratory test values, we investigated the values from the onset of agitated delirium in the agitated delirium group and from 1 week before death in the nonagitated delirium group. For both groups, data from a day close to the day selected for evaluation was used when no data was available on the evaluation day.
Statistical analysis
We used Student's t tests to compare age, BMI, and laboratory test values. To compare the two groups, we used a Fisher's exact test for independent verification of other items and performed univariate analyses using Microsoft Excel Statistics package (Microsoft, Redmond, WA). We also performed a dendritic analysis of the agitated and nonagitated delirium groups for all investigational items.
Drug therapy
With regard to pharmacotherapy for agitated delirium, we selected to investigate drugs that were administered for 5 days or more. This was because the type and dosage of drugs that were used for the suppression of the recurrence of agitated delirium varied over a period of 4 days in certain patients. If patients had no recurrence of agitated delirium for a period of more than 5 days within 14 days of administering the drugs, they were considered as having no recurrence. When injectable drugs were used, we considered them to be periodically administered drugs after the dosage stabilized. Thus, cases in which no agitated delirium was observed through the entire period of drug injection were regarded as “no recurrence” cases.
Results
Subjects
One hundred twenty-six patients who were 16 years of age or older died of cancer in our institution in 2008. One hundred fifteen of these patients were enrolled as subjects in this study. Ten patients were excluded because of serious illnesses such as dementia, meningitis carcinomatosa, hepatic encephalopathy, postresuscitation encephalopathy, brain metastasis, or personality disorders; one patient was confined to ICU. Hence, these patients were excluded because we believed that an accurate evaluation of the agitated delirium in these patients would be difficult. The final group of included patients consisted of 64 males and 51 females; the average age was 58.8±15.3 years. The most common primary sites of cancer were as follows: the blood for 28 patients, the lungs for 14, the breasts for 14, and the pancreas for 10. The most common primary sites of metastasis were as follows: the lungs for 53 patients, the bones for 43, the liver for 41, and the brain for 17.
Patients with agitated delirium spent an average of 38 days in hospital. Agitated delirium occurred most frequently 6 days before death (mode, in 6 cases) on an average, it occurred 20 days before death, with the median value being 11 days before death (Fig. 1).

Period of time before death onset of agitation.
Investigation results
Agitated delirium was observed in 49 subjects (42%). With regard to patient characteristics, the mean age of the patients in the agitated delirium group was significantly higher than that of the patients in the nonagitated delirium group. The agitated delirium group also had a higher proportion of male patients and patients with positive smoking history compared with nonagitated delirium group (Table 1). With regard to the primary cancer site and existence of complications, lung cancer and diabetes occurred significantly more in the agitated delirium group than in the nonagitated delirium group (Figs. 2 and 3). When the laboratory test values of the agitated delirium and nonagitated delirium groups were compared, GFR values were significantly lower and CRP levels were significantly higher in the agitated delirium group (Table 2).
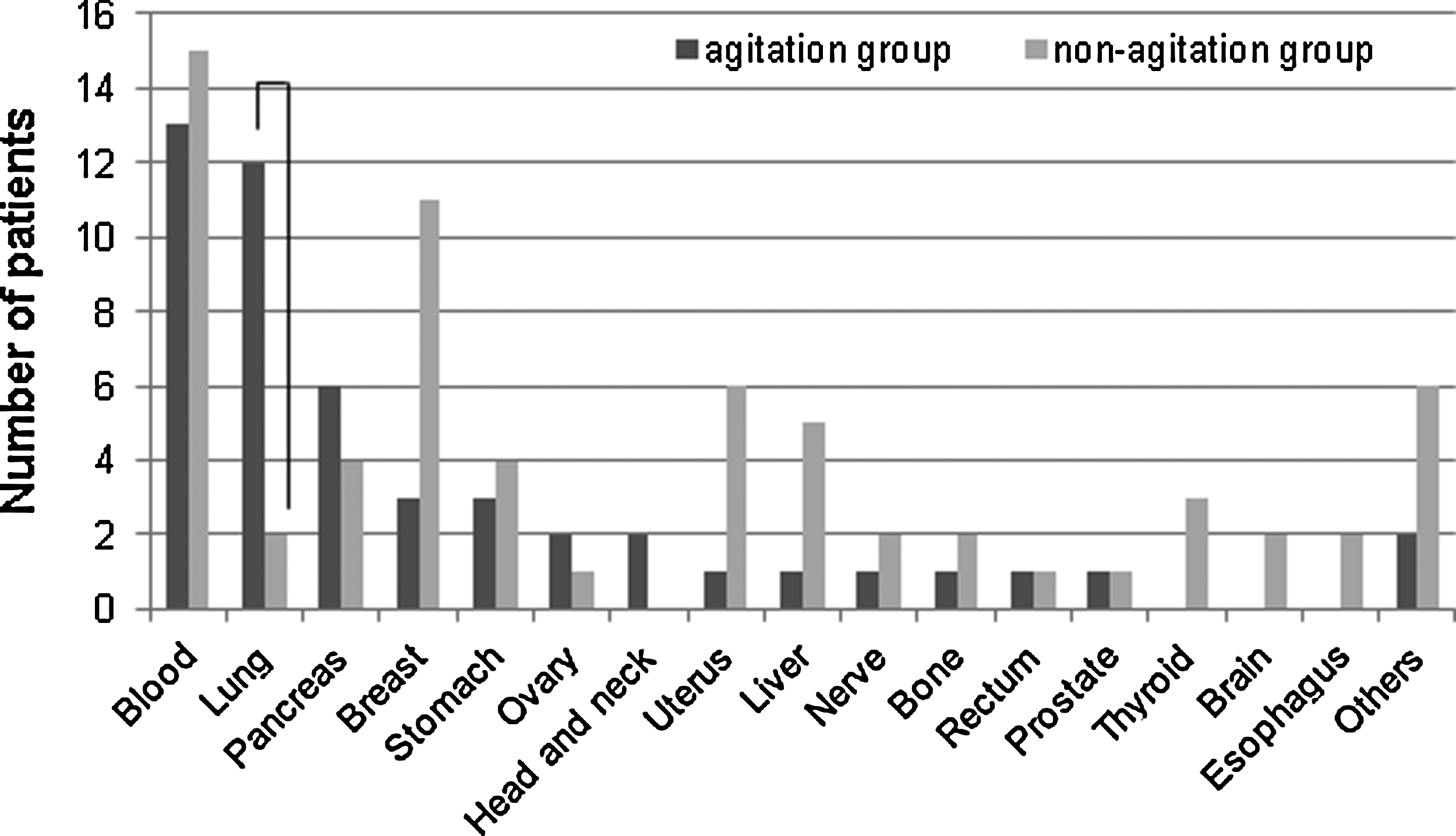
Primary site of cancer.

Comorbidity.
p<0.05, bp<0.01.
age: average±SD, BMI: average.
age, BMI: t-test, others: Fisher's exact test.
BMI, body mass index.
t-test *p<0.05.
SD, standard deviation; WBC, white blood cell count; Plt, platelet; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GFR, glomerular filtration rate; CRP, C-reactive protein; Alb, albumin.
Analysis results
We performed a dendritic analysis with all risk factors. Figure 4 shows the composition of the decision tree that was obtained from our analysis and used as a predictive model. When creating this model, we excluded any patient for whom we could not investigate even 1 factor. There were a total of 99 patients, with 45 patients in the agitated delirium group and 54 patients in the nonagitated delirium group. According to the decision tree, key risk factors for predicting the occurrence of agitated delirium were lung cancer, high CRP levels (≥22.32 mg/dL), diabetes, old age (≥72.5 years), and a positive smoking history. With regard to risk factors in the decision tree, 98.2% of patients did not exhibit agitated delirium, whereas 73.3% exhibited agitated delirium; we obtained a specific rate of 86.9%.

Among each item, 0 is a group that is not applicable to the factor and 1 is a group that is applicable to the factor. C-reactive protein (CRP) and age are divided into two groups in the range of number. The size is ratio (%) of the total number of people of the items (99 people). Purity is the ratio (%) of the number of people of the agitation group in the item (or the nonagitation group).
Type and effects of therapeutic drugs
Table 3 shows the drug therapies used to treat agitated delirium and their effects. Drugs for preventing recurrence were only used in 17 cases.
Discussion
We targeted patients with agitated delirium with this method. This investigation elucidated the risk factors for agitated delirium in terminal patients with cancer. However, as mentioned above, delirium during the last days of life may indicate terminal phase agitation. 2 For patients with cancer, delirium occurred in 8%–40% of inpatients and increased from 27% to 83% in the terminal phase and immediately before death (weeks to days before death). 2 According to Bruera et al., 4 the incidence of delirium in terminal patients with cancer in the palliative care unit was 34% when they were admitted and 83% immediately before death (16±6 days). Of the 115 terminal patients with cancer enrolled in this study, agitated delirium was observed in 49 (42%), which was similar to the rate observed in the palliative care unit.
When the agitated and nonagitated delirium groups were compared according to the results of the univariate analysis, background factors such as older age, male gender, and positive smoking history were significantly higher in the agitated delirium group. Delirium occurs often in elderly patients.5,6 There have also been reports of it being more common in males. 6 Lungs as the primary site of cancer and a diabetic state as a complication were significantly more common in the agitated delirium group than in the nonagitated delirium group. No difference was observed with regard to the site of metastasis. Pulmonary disease was also cited as a cause of delirium, and respiratory failure has been reported to be a risk factor related to the time of diagnosis of delirium. 12 We believe that lung cancer was significantly more common in the agitated delirium group because it is related to respiratory failure. Furthermore, we believe that diabetes is a risk factor because endocrine disorders are also considered to cause delirium. 12
After comparing the laboratory test values, we used the test values from the first day of agitated delirium onset for the agitated delirium group and the values from 6 days before death for the nonagitated delirium group. This is because the first occurrence of agitated delirium occurred most often 6 days before death in the agitated delirium group. Because the period from the day when the agitated delirium first occurred until the patient's death in certain cases in the agitated delirium group was long, many investigational items showed a better trend than those in the nonagitated delirium group. However, GFR values were significantly lower in the agitated delirium group than in the nonagitated delirium group. This suggested that agitated delirium often occurs in patients with decreased kidney function. In addition, CRP values were significantly higher in the agitated delirium group than in the nonagitated delirium group. Although infection or cachexia was believed to have caused this, these factors could not be evaluated in our study.
Dendritic analysis is a method of data mining where multifactorial analysis is used for a group with a high number of objective variables, and one concentrated featured variable is obtained. The analysis allows a tree diagram to be constructed by stratification and the flow of the evaluation to be visually comprehended. Therefore, we decided to apply a dendritic analysis in this study in order to determine the characteristic factors for predicting the occurrence of agitated delirium. The factors shown in Figure 4 had a significance of 5%, and they were shown to be related to the predicting agitated delirium. However, even among these factors, for a few cases, such as the 16 cases with a drinking habit or cases in which factors were distributed in extreme ratios (e.g., with the head and neck area [primary site] of the 38 cases, only 1 case had a drinking habit), the importance of the factor is decreased. Furthermore, even if a factor is commonly present among all cases just as much as a higher factor, it is not as important as the higher factor—the more important the factor, the higher is its purity (e.g., although agitated delirium did not occur in cases with positive smoking history with a purity of 57.9%, it did not occur in cases with no smoking history with a purity of 84.2% as well; therefore, a difference in purity is evident). From the above findings, we can deduce that the accuracy of predicting agitated delirium with factors such as infections (except pneumonia), drinking habits, cancer of the head and neck, and gender are low, and the factors that are important in the prediction of agitated delirium occurrence are lung cancer, high CRP levels (≥22.32 mg/dL), diabetes, old age (≥72.5 years), and positive smoking history. If these are present, agitated delirium is more likely to occur. In addition, on the basis of this decision tree flow chart, we were able to obtain a specific rate of 86.9% as a whole, and 98.2% of the patients did not exhibit agitated delirium, while 73.3% patients exhibited agitated delirium. The specific rate was less than 100% because of the frequent occurrence of agitated delirium in patients without meningeal dissemination despite their having lung cancer and because of the presence of factors with low precision such as infection (except pneumonia), drinking habits, and gender.
Investigative research conducted on delirium in patients with cancer has so far been related to the distribution and prevalence of the delirium amongst other psychiatric diagnoses, 12 rather than on an investigation of risk factors. Because of this, the number of patients with cancer who exhibited agitated delirium in previous studies was not sufficient to obtain a relationship between risk factors. 12 In contrast to this, our study clarified the risk factors for agitated delirium in the terminal phase.
With regard to the drugs administered to prevent recurrence of agitated delirium, no recurrence was observed in 15 (88.2%) of the 17 patients who received therapeutic drugs. Of the 2 patients with recurrences, the dosage was possibly not sufficient for 1 patient who was administered midazolam. We beleve that cirrhosis caused by liver metastasis may have been involved in the case of the other patient who was administered haloperidol. In recent years, haloperidol injections or oral administration of antipsychotic drugs (when possible) such as haloperidol, risperidone, quetiapine, and olanzapine have been used to treat delirium, particularly in cases of hyperactive delirium. In the patients included in the study, only haloperidol, risperidone, and midazolam were administered. Injections were used for 14 of the 17 patients because they were in an agitated state and oral administration was not possible.
Because delirium is an important factor in the palliative prognostic index, 16 which is widely used as a prognostic indicator for delirium including agitated delirium, we believe that further validation is necessary in the patient groups in which delirium does not occur because there is a possibility of evaluating the vital prognosis as being longer.
In future, it is necessary to separate terminal patients with cancer into high- and low-risk groups according to their risk factors, perform adequate countermeasures, and investigate therapeutic drugs for the treatment of terminal phase agitated delirium in which the cause is difficult to eliminate. Our research was conducted at an isolated facility. Thus, we believe that conducting a large-scale investigation at multiple facilities in future would improve the accuracy of these results.
Footnotes
Acknowledgments
No funding was received for this work, and the authors report no conflicts of interest.
Author Disclosure Statement
No competing financial interests exist.