
Abstract
Abstract
Context:
Unmet spiritual needs have been associated with decreased patient ratings of quality of care, satisfaction, and quality of life. Few instruments exist to measure spiritual needs particularly among non-English speaking patients in the U.S.
Objective:
To develop an internally consistent and reliable Chinese version of the Spiritual Needs Assessment for Patients (SNAP).
Methods:
The SNAP consists of 23 total items in 3 domains: psychosocial (n=5), spiritual (n=13), and religious (n=5). The Chinese SNAP was developed through a translation-back translation process followed by cognitive pre-testing. The instrument was then administered to a convenience sample of 30 ambulatory predominantly Mandarin speaking cancer patients in New York. We tested for internal consistency, test-retest reliability, and degree of association with the question “Have your spiritual needs been met?”
Results:
Mean participant age was 56 years, 70% had less than a high school education. Twenty three percent were Buddhist, 63% identified no religious affiliation, 83% described themselves as spiritual but not religious, 33% reported unmet spiritual needs, and 60% wanted help meeting their spiritual needs. The Cronbach's alpha for the total SNAP was 0.89. Test-retest correlation coefficient for the total SNAP=0.75. Unmet spiritual needs, as assessed through a single-item question, were not associated with higher SNAP scores in contrast to results of the English SNAP.
Conclusion:
The Chinese SNAP is an internally consistent and reliable instrument for measuring spiritual needs. The apparent lack of correlation between the SNAP score and the question on unmet spiritual needs may suggest that the SNAP captures patient needs considered by Westerners to be spiritual but that Chinese patients might not readily describe as spiritual.
Introduction
There are only a few validated instruments with which to measure spiritual needs. We recently reported on a newly devised English language instrument that distinguishes between psychosocial needs, spiritual needs, and religious needs. We validated this instrument in English-speaking patients in an urban outpatient cancer center. 6
After Spanish, the Chinese languages represent the most common non-English language spoken at home in the United States, with 2 million Chinese speakers in the 2000 census
There is little data about the spiritual needs of Chinese-speaking patients who are cared for in the United States. The Maimonides Cancer Center is situated in the midst of a neighborhood with a predominant Chinese-speaking population and is an ideal location in which to develop and validate a Chinese language spiritual needs survey instrument.
Methods
Participants
Participants were recruited at the Maimonides Cancer Center in Brooklyn, New York. Patients self-identified as being of Chinese ethnicity, spoke and read Mandarin or another dialect of spoken Chinese, and were over the age of 18 years. Potential subjects were identified by their treating physicians, two Mandarin-speaking medical oncologists, and signed a letter of participation. The study was approved by the Maimonides Institutional Review Board.
Instrument
The English Spiritual Needs Assessment for Patients (SNAP) measure (see Appendix 1) includes 23 total items: 5 in the domain of psychosocial needs, 13 in spiritual needs, and 5 in religious needs. Responses were categorized on a scale of 1–4: “Very much,” “Somewhat,” “Not very much,” and “Not at all.” The Chinese version of the SNAP (see Appendix 2) was developed through a translation–back translation process. First, the SNAP was translated from English to Chinese by a bilingual Chinese-American physician. Next, a focus group of eight Mandarin- and Cantonese-speaking staff revised the translated items. The Chinese version was then translated back into English by a separate bilingual person. Finally, we subjected the translated items to cognitive pretesting8,9 with a convenience sample of eight Chinese ambulatory oncology patients at Maimonides. We made iterative adjustments based on these interviews, refining the characters for the translated items. Since the written characters are the same, a single written instrument can be used for a multiplicity of Chinese languages.
Patient demographics and clinical information were obtained via a patient questionnaire that was administered in Chinese. Patients also completed information on their religion, whether they consider themselves spiritual but not religious, and how often they attend religious services. They answered a question on whether they felt their spiritual needs were being met (yes/no) and whether they wanted help in getting their spiritual needs met (yes/no).
Statistical analysis
We assessed internal reliability using the Cronbach's alpha. Test-retest reliability was assessed using intraclass correlation coefficients (ICC) for the total scale in all 30 patients, who were re-interviewed within two weeks. Using Mann-Whitney U testing, we measured the association between the total scale and subscale scores and the dichotomized response (yes/no) to the following spiritual needs question: “Do you feel your spiritual needs are being met?” Since we had shown significant associations in English, we hypothesized that patients who answered that their spiritual needs were not being met would have higher total scale scores and higher scores on the spiritual needs subscale compared to the religious and psychosocial needs subscales. All data analyses were conducted using Stata 11.0 (StataCorp, College Station, Texas).
Results
Study sample
Thirty-five outpatients were approached, of whom five declined participation because of lack of time, resulting in a study sample of 30 participants. Characteristics of the participants are described in Table 1. Twenty-eight of the 30 participants (93%) spoke Mandarin (some of this group also spoke Cantonese), and two (7%) spoke Fujianese only. Over half of the sample (73%) had less than a high school education (70%). Two-thirds of patients had Medicaid insurance.
Other includes prostate, adrenal, renal, and thyroid cancer.
While the majority of participants (63%) identified no religious affiliation, 23% described themselves as Buddhist, 10% as Protestant, and 3% Catholic. Sixty-three percent of participants never attended religious services, but almost all of them (83%) described themselves as spiritual but not religious. Thirty-three percent of participants reported that their spiritual needs had not been met and 60% wanted help meeting their spiritual needs.
Descriptive statistics and scale reliability
Figures 1, 2, and 3 show the score distribution for each of the three subscales, with higher scores indicating higher need. Table 2 shows the mean for each individual subscale item. The mean score for the psychosocial needs subscale was 13.7 (SD 3.5). The mean score for the spiritual needs subscale was 28.5 (SD 8.8). The mean score for the religious needs subscale was 8.3 (SD 4.4).
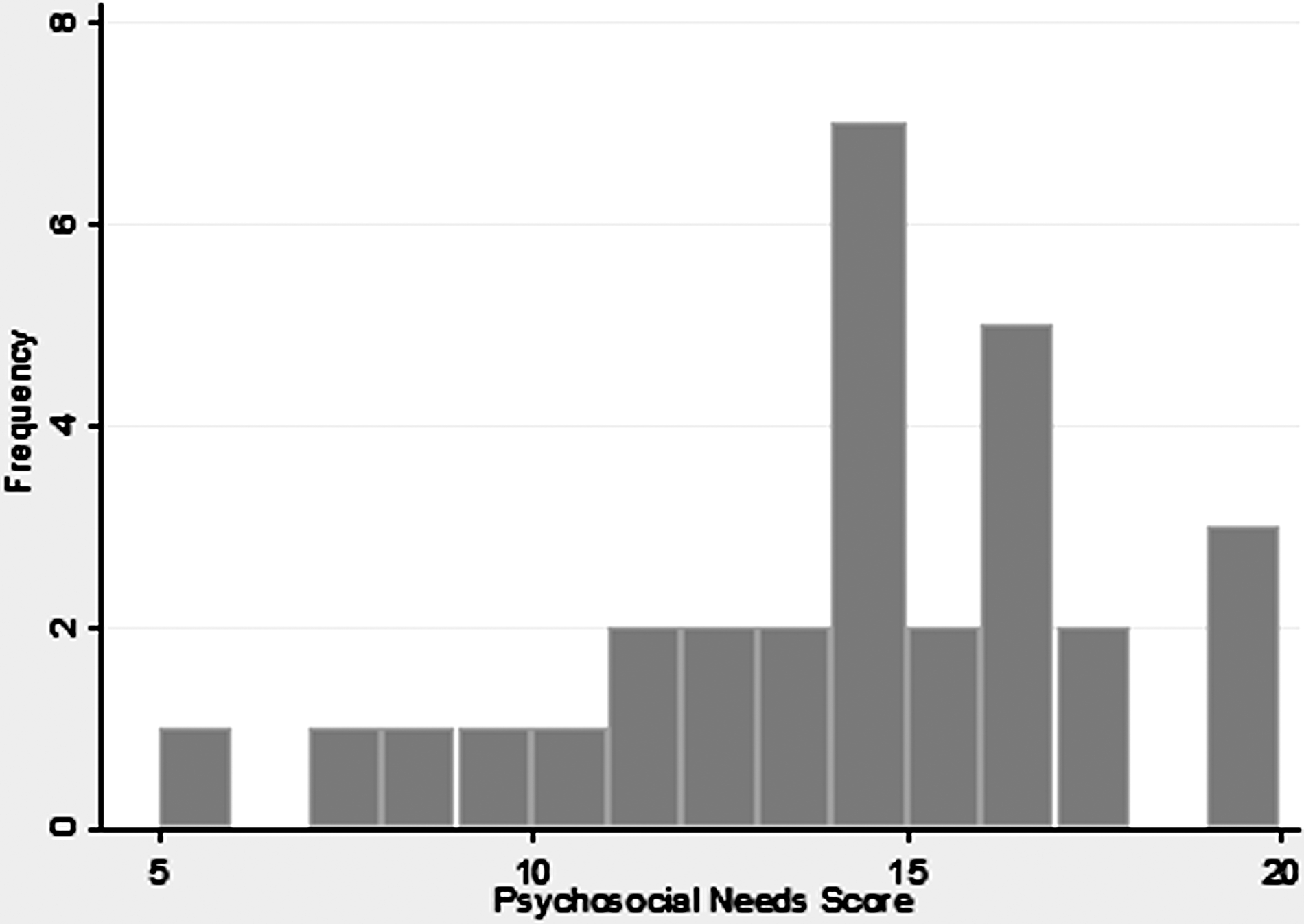
The psychosocial needs subscale distribution. (Note: Score of 5 indicates no psychosocial needs. Higher scores indicate higher psychosocial needs.)
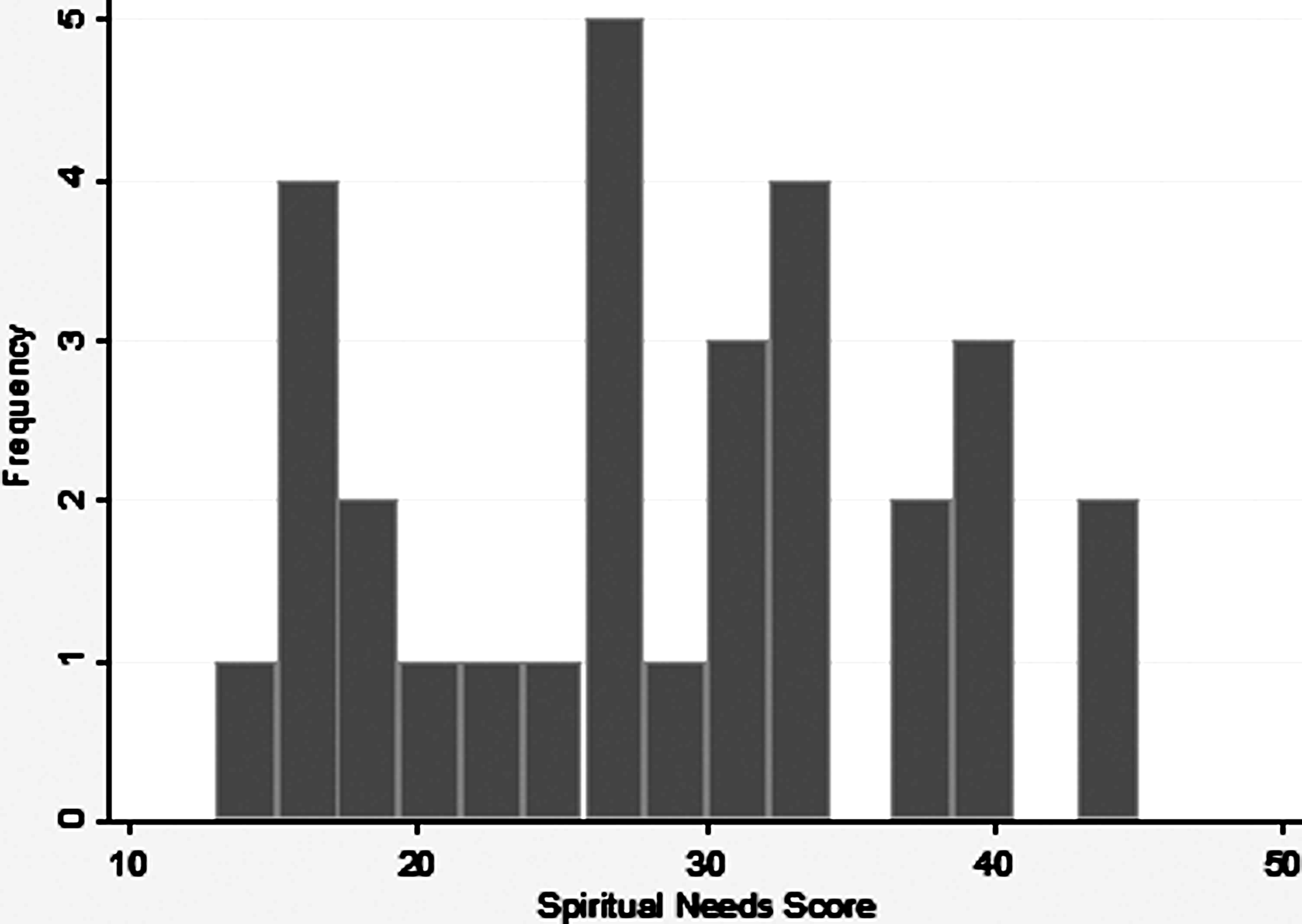
The spiritual needs subscale distribution. (Note: Score of 13 indicates no spiritual needs. Higher scores indicate higher spiritual needs.)
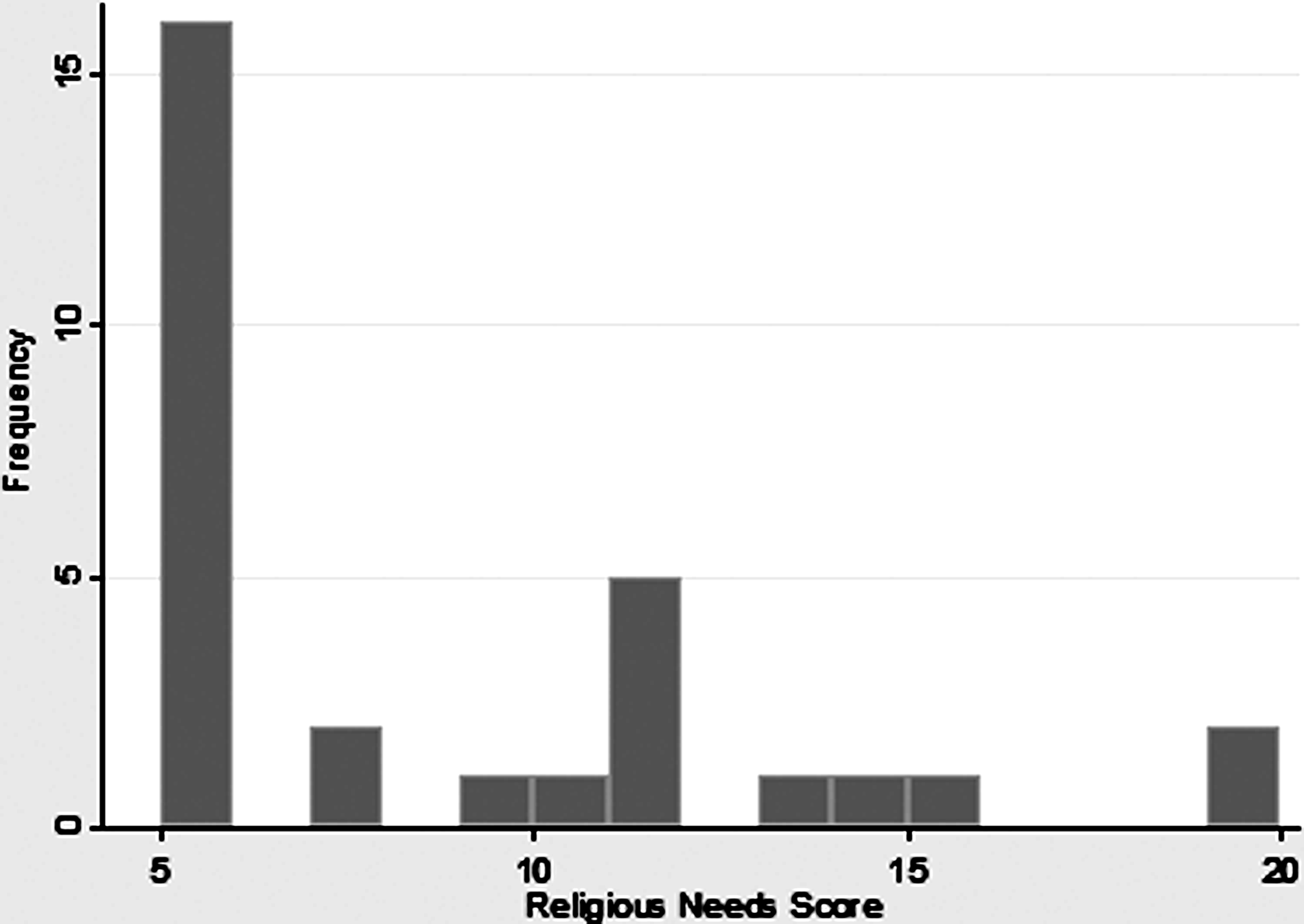
The religious needs subscale distribution. (Note: Score of 5 indicates no religious needs. Higher scores indicate higher religious needs.)
SD, standard deviation.
Note: The question stem was: “How much would you like help with the following?” Response options were “very much” (4 points), “somewhat” (3 points), “not very much” (2 points), and “not at all (1 point).
Test-retest reliability of the Chinese SNAP was 0.75 as determined by the intraclass correlation coefficient (ICC). The ICC for the three subscales was as follows: psychosocial needs 0.57, spiritual needs 0.70, and religious needs 0.77.
Internal consistency
The Cronbach's alpha coefficient for the total SNAP was 0.89, and for each of the subscales was as follows: psychosocial needs 0.58, spiritual needs 0.83, and religious needs 0.90. We tested the total SNAP score and each of the subscale scores for association with the following general spiritual needs assessment question: “Are your spiritual needs being met?” There was no significant association between responses to this question and subscale or total scale scores (p=0.37).
Discussion
Spirituality, religion, and personal beliefs have been shown to represent an important component of quality of life across cultures, especially in seriously ill patients. Patients may understand the meaning of illness differently depending upon cultural background, and English-language terms that describe deeply personal experiences require careful translation and validation if clinicians are to understand better the needs of patients from diverse cultures.
Increasing numbers of U.S. residents speak a Chinese dialect as their primary language. Little is known about the spiritual needs of this group of patients.10,11,12 One recent comprehensive review of Chinese spirituality notes that “there are few scientific studies on spirituality of the Chinese people.” 13
We used a number of well-accepted methods of translation and validation including an expert panel of native Chinese speakers to review the translation, cognitive pretesting using a focus group of predominantly Mandarin-speaking cancer patients, Cronbach's alpha to assess internal consistency, and readministration of the survey instrument to determine test/retest reliability. We found excellent internal consistency, with a Cronbach's alpha of 0.89. Test/retest reliability was also within an acceptable range.
Our patient population consisted of recent immigrants of low socioeconomic status and little formal education, with two-thirds reporting Medicaid as their primary health insurance and 70% with less than a high school education. This is a limitation of the study, as a study group with more formal education might have responded to our survey questions differently. Future studies will attempt to include a wider socioeconomic range of Chinese-speaking patients. The group was evenly balanced between men and women and had the range and percentages of malignancies that one would expect to see at a cancer center in a population of recent immigrants to the United States from China. Relatively few identified with formal religion, with 63% reporting no religious affiliation. Importantly, however, many patients reported a wide range of specific spiritual needs, a few reported specific religious needs, and 60% wanted help in addressing their spiritual needs.
In contrast to our English-language instrument, we found no association between increasing spiritual needs (as measured by our spiritual needs subscale) and response to the single question, “Are your spiritual needs being met?” Given our small sample size, we cannot exclude a type II error. In reviewing free text responses where our study population could write in their specific spiritual needs, however, patients specified needs such as support from family and friends, communication with doctors and nurses, and singing and dancing with a group. These sorts of needs might not be captured by the English word “spiritual,” which suggests that our Chinese-speaking patient population might not have understood our Chinese term “spiritual” as a Western population might, or may not have responded to an inquiry regarding adequacy of addressing spiritual needs in the same way that a predominantly Western patient population would understand the term. Our instrument does include examples of “psychosocial” needs as distinguished from “spiritual” ones in our psychosocial subscale, however, which suggests that it would not miss these concerns among a population of Chinese patients.
We have translated spirituality as  or jing shen. In our view this is the closest Chinese language equivalent. It connotes a person's deepest beliefs. A secondary alternative would be
or jing shen. In our view this is the closest Chinese language equivalent. It connotes a person's deepest beliefs. A secondary alternative would be  or xin ling. This corresponds approximately to the English word “soul.” As we continue to refine this instrument, we may include both terms. For instance, we have translated the question, “Do you consider yourself spiritual but not religious” as “
or xin ling. This corresponds approximately to the English word “soul.” As we continue to refine this instrument, we may include both terms. For instance, we have translated the question, “Do you consider yourself spiritual but not religious” as “ .” As an alternative we may substitute, “
.” As an alternative we may substitute, “ .”
.”
Overall, we found that our Chinese translation of the SNAP was internally consistent. The English word “spiritual,” however, may not translate readily into Chinese. While the instrument detects unmet needs of Chinese patients that correspond to needs that Western patients identify as spiritual, definitive linguistic validation will require further study.
Footnotes
Author Disclosure Statement
This work was supported by a donation from Ms. Dorothy Kryger. The authors have no relevant conflicts of interest to report.
Acknowledgments
The authors would like to thank Shulin Wang, M.D., for her assistance in translating and administering the survey instrument and in data collection and Jeremy Weedon, Ph.D., for statistical analysis.