
Abstract
Abstract
Background:
Pain is common during cancer treatment, and patient self-reporting of pain is an essential first step for ideal cancer pain management. However, many studies on cancer pain management report that, because pain may be underestimated, it is often inadequately managed.
Objective:
The aim of this study was to evaluate the effectiveness of bedside self-assessment of pain intensity for inpatients using a self-reporting pain board.
Methods:
Fifty consecutive inpatients admitted to the Oncology Department of Chungbuk National University Hospital were included in this observational prospective study from February 2011 to December 2011. The medical staff performed pain assessments by asking patients questions and using verbal rated scales (VRS) over 3 consecutive days. Then, for 3 additional days, patients used a self-reporting pain board attached to the bed, which had movable indicators representing 0–10 on a numeric rating scale (NRS) and the frequency of breakthrough pain.
Results:
Patient reliability over the medical staff's pain assessment increased from 74% to 96% after applying the self-reporting pain board (p=0.004). The gap (mean±standard deviation [SD]) between the NRS reported by patients and the NRS recorded on the medical records decreased from 3.16±2.08 to 1.00±1.02 (p<0.001), and the level of patient satisfaction with pain management increased from 54% to 82% (p=0.002).
Conclusion:
This study suggests that the self-reporting bedside pain assessment tool provides a reliable and effective means of assessing pain in oncology inpatients.
Introduction
It is relatively easy to use a self-reporting system, such as a pain diary, for outpatients whose performance status is relatively good and whose condition is stable. However, it is relatively difficult for inpatients with poor general health and acute problems (in addition to pain) to express their degree of pain. In fact, many studies on cancer pain management report that observer and patient assessments do not correlate well, and that there is a tendency for medical staff to underestimate pain levels.11–13 Therefore, the aim of this study was to evaluate the effectiveness of inpatient bedside self-assessment of pain intensity using a self-reporting pain board attached to the bed.
Methods
Patients
All consecutive eligible inpatients admitted to the Oncology Department of Chungbuk National University Hospital were considered for this study. The following inclusion criteria were applied: age>18 years, a histologically confirmed diagnosis of cancer, pain due to cancer or cancer treatment, ability to understand the Korean language, and normal cognitive function. Patients with terminal conditions or low performance status (Eastern Cooperative Oncology Group [ECOG] performance status≥4) were excluded. Opioid treatment varied from patient to patient, and short-acting analgesics were available to all patients. Written informed consent was obtained from all patients prior to participating in the study. This observational study was reviewed and approved by the Institutional Review Board of Chungbuk National University Hospital.
Pain measurement method
To estimate the effectiveness of a self-reporting pain assessment system alone, we educated patients regarding the general principles of cancer pain and pain management on the first day of study participation prior to the first assessment (Appendix A). Over the first 3 days of the study, pain assessments were performed by medical staff, who asked questions and recorded the patients' answers using a 0–10 VRS, in which 0 indicated no pain and 10 indicated the worst pain imaginable. Over the following 3 days, a self-reporting pain board was attached to each patient's bed, and the patients were instructed on how to use the board by the research nurse. Pain assessments were then carried out using these self-reporting bedside pain boards, which had movable indicators representing a 0–10 NRS and the frequency of breakthrough pain (Fig. 1). The pain score was recorded 3 times a day: at 10 AM for the morning assessment, 4 PM for the afternoon assessment, and 10 PM for the evening assessment. The average pain intensity in Days 3 and 6, as recorded by the patient in the patient questionnaire, was used to generate the NRS for the medical record.
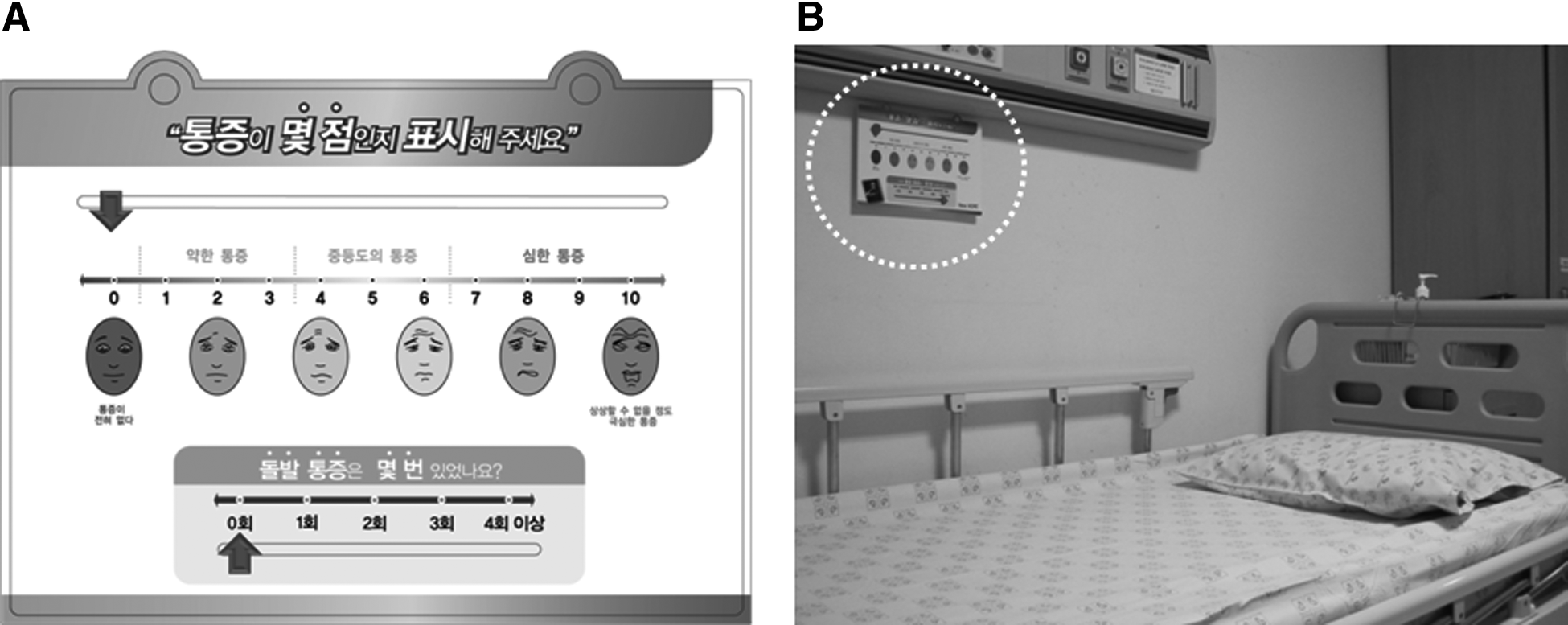
The self-reporting pain board. (
Data collection
Cancer pain knowledge questionnaire
All patients completed a seven-item cancer pain knowledge questionnaire (Appendix B). One item contained 10 questions that addressed the patient's knowledge of cancer pain, addiction, and analgesics. Two items addressed the average pain intensity and breakthrough pain experienced by the patient during the previous 24 hours, one item addressed sleep disturbance due to pain, one item (containing seven questions) addressed the patients' impressions of their current pain management, one item addressed the goals of pain control, and one item addressed levels of satisfaction with the current pain management. Questionnaires were also provided to three matched medical staff (two physicians and one nurse attending each patient) (Appendix C). A two-item cancer pain questionnaire contained questions regarding the reliability of matched patient pain and the workload required to assess patient pain. This survey was conducted twice for patients and medical staff, both before and after using the self-reporting pain board at the bedside.
Patient medical record review
Patient medical records were reviewed to obtain baseline demographic data (age and sex), performance status, stage of disease, current treatment(s), aim of treatment, reason(s) for admission, patient-recorded pain intensity, and analgesic doses. The Pain Management Index (PMI) was used to evaluate the adequacy of analgesic use.14–18 Analgesic strength was categorized as 0 (no analgesic), 1 (nonopioid), 2 (weak opioid), or 3 (strong opioid). In addition, patient pain levels, based on the modified Brief Pain Inventory, were classified as follows: 0 (no pain=0), 1 (mild pain=1–3), 2 (moderate pain=4–6), or 3 (severe pain=7–10). PMI values were calculated by subtracting the pain scores from the analgesic scores. Scores of 0 or above indicated adequate analgesia, whereas a negative score indicated inadequate analgesia.
Statistical analyses
χ2 tests were used to compare percentages, and independent sample t tests were used to compare mean values. Descriptive statistics were reported as proportions and medians. The means and standard deviations (SD) of the reliability of patient pain assessed by medical staff, workload required by medical staff to assess patient pain, NRS, dose of morphine, and frequency of breakthrough pain were also calculated. All significance levels refer to two-sided tests. A p value of<0.05 was considered significant. All statistical analyses were performed using SPSS for Windows software, version 15.0 (SPSS Inc., Chicago, IL). The study design is presented schematically in Figure 2.
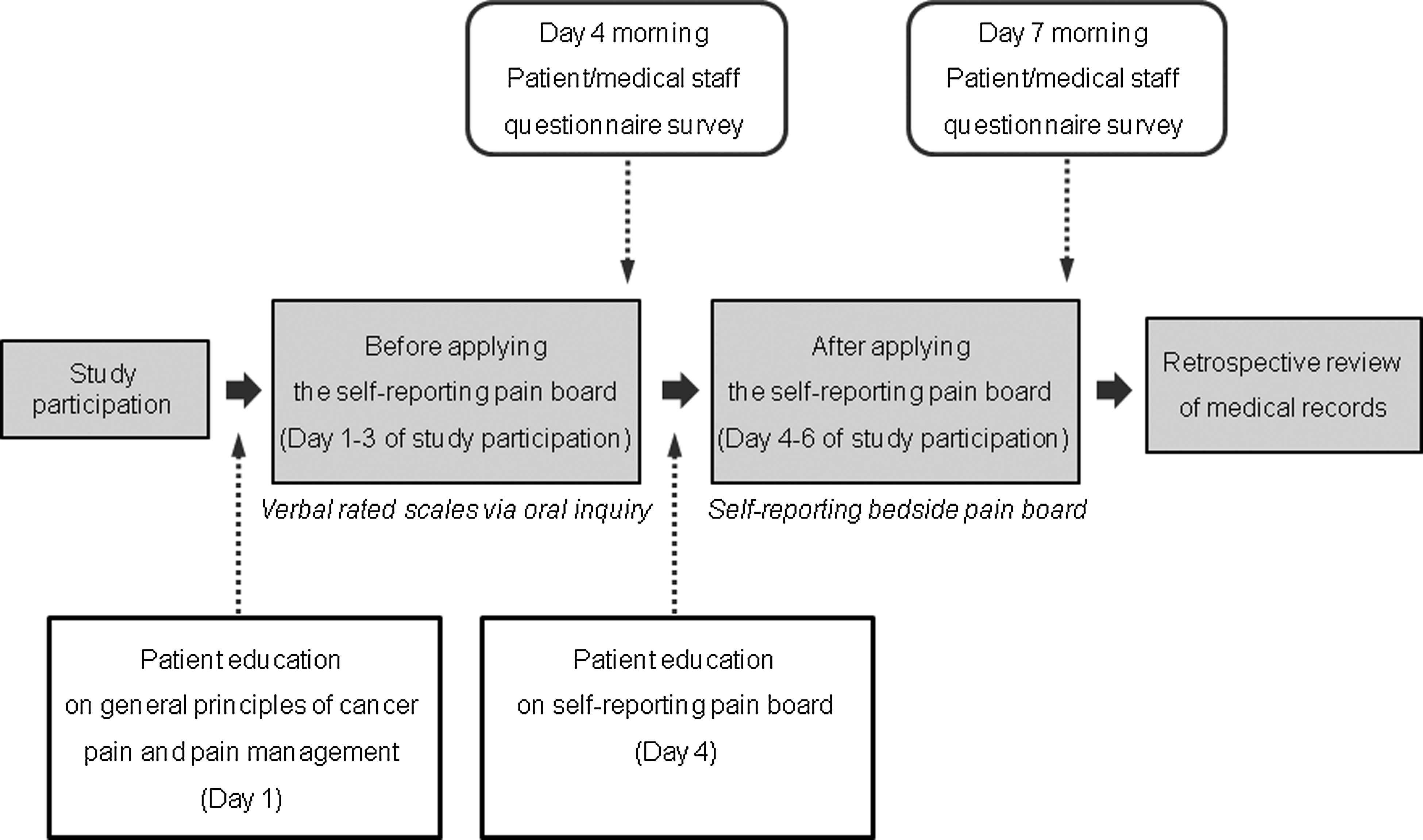
Study design.
Results
Of the 67 patients screened between February 2011 and December 2011, 54 were included in the study, and 13 patients were excluded because of cognitive impairment (n=5), refusal to participate (n=6), or inability to fill in the questionnaire (n=2). Of the 54 remaining patients, 50 had complete data that were evaluable, and 4 had incomplete data because of early discharge (n=2) or a rapid deterioration of disease status (n=2) and were excluded. The demographics, clinical characteristics, pain intensity, and analgesic drug consumption of the 50 patients who comprised the study cohort are shown in Table 1. The median age of the patients was 59.4 years (range, 28–80 years) and 33 (66%) were men. Eighteen patients (36%) had good ECOG performance status (0–1), the majority of patients (80%) had stage IV disease, and 18 patients (36%) were currently receiving only best supportive care. Fourteen patients (28%) reported moderate or severe pain based on the NRS scale, and 46 patients (92%) were receiving opioid treatment at Day 1 of the study. For the matched medical staff data, 150 questionnaires (from two physicians and one nurse per patient) were analyzed. The number of medical staff participating in the questionnaire was 46 (12 physicians and 34 nurses), and the median number of questionnaires from each medical staff was 2 (range, 1 to 5).
ECOG, Eastern Cooperative Oncology Group Performance Status; NSAID, nonsteroidal anti-inflammatory drug; NRS, numeric rating scale; SD, standard deviation.
Changes in perception of cancer pain and patient satisfaction with pain management
Changes in perception of cancer pain and pain management after using the self-reporting pain board are shown in Table 2. The percentage of patients who answered “most pain is relieved sufficiently by pain killers” increased from 76% to 90% after using the self-reporting pain board attached to the bed (Question 1.2 [Q1.2]; p=0.035). The percentage of patients who answered “absolutely yes” or “yes” to the item “medical staff tend to underestimate my pain” decreased from 32% to 12% (Q1.7; p=0.002). In addition, the percentage of patients who answered “pain caused by cancer can be controlled effectively by pain killers” increased from 48% to 88% (Q1.9; p<0.001). Patient reliability over the medical staff's pain assessment increased from 74% to 96% after using the self-reporting pain board (Q5.3; p=0.004). Moreover, the percentage of patients who answered “if I consider pain treatment unsatisfactory, the doctor changes the drug or the dose” increased from 68% to 96% (Q5.4; p=0.001). As a result, the level of patient satisfaction with pain management increased from 54% to 82% (Q7; p=0.002; Fig. 3).
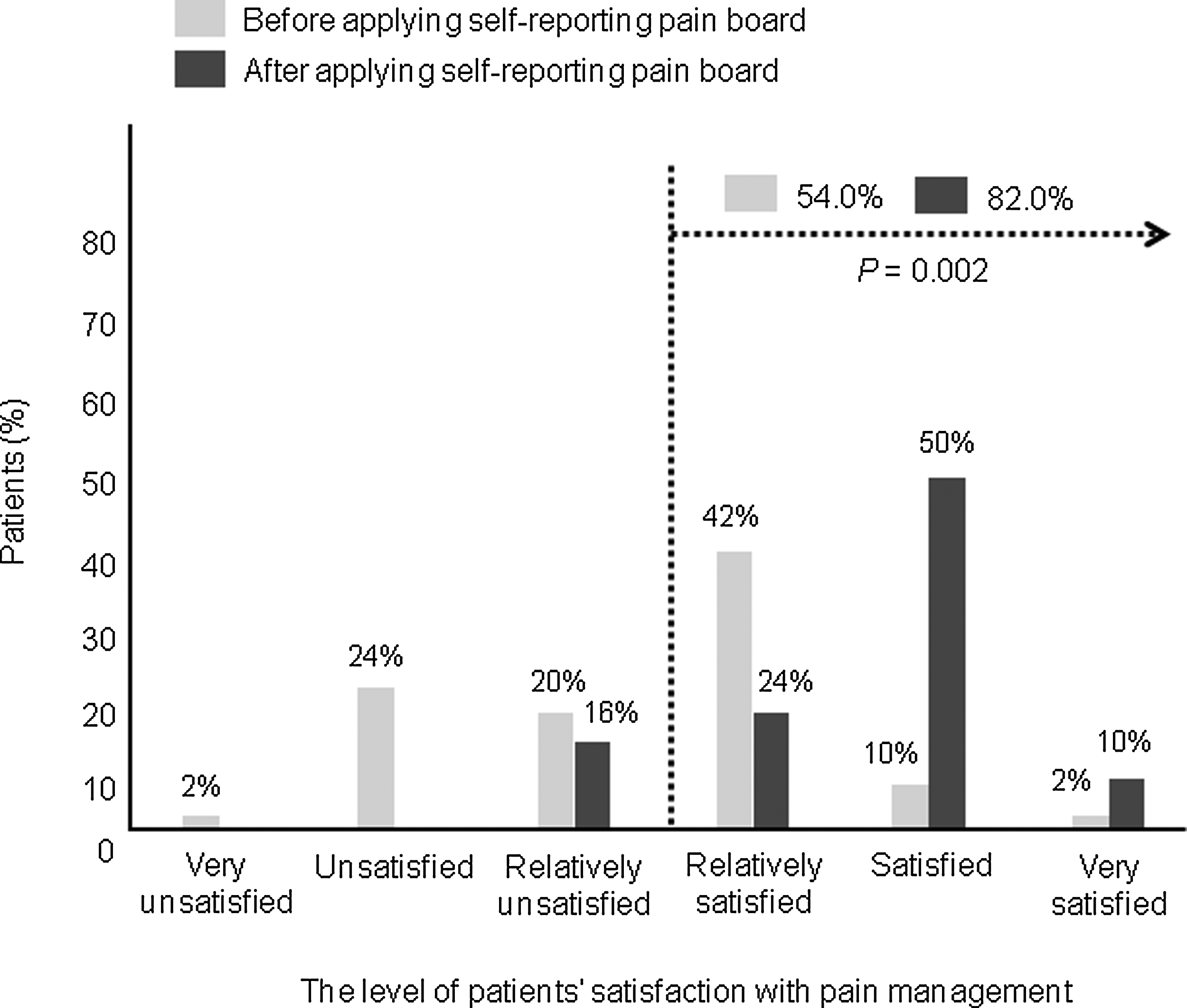
Changes in the levels of patient satisfaction with pain management after applying the self-reporting pain board.
Changes in the reliability of patient pain and workload incurred by pain assessment by medical staff
The reliability of patient pain recorded by medical staff was not significantly different after applying the self-reporting pain board (down from 3.06±1.34 to 2.98±1.54) (Q2; a score of 5 indicated very reliable; p=0.788). However, the percentage of medical staff that answered “yes” to the item “pain intensity expressed in the medical records of this patient is recorded exactly as stated by the patient” increased from 47.3% to 65.3% (Q3; p<0.001). The percentage of medical staff that answered “yes” to the item “I tend to underestimate the patient's pain” decreased from 38.0% to 16.0% (Q4; p=0.002). Changes in the medical staff's perception of pain assessment, as evaluated using the medical staff questionnaire, are shown in Table 3. Moreover, the workload required to assess patient pain decreased from 46.9±15.5 to 24.3±11.2 after using the self-reporting pain board (Q5; a score of 100 indicated highly burdensome; p<0.001).
Impact of the adequacy of pain assessment and management
The gap between the NRS reported by patients and that stated in the medical records decreased from 3.16±2.08 to 1.00±1.02 after using the self-reporting pain board (Fig. 4; p<0.001). Moreover, the gap between patient- and staff- (three matched medical staff) assessed NRS decreased from 1.82±1.61 to 0.92±0.74 (p=0.001). Although the patient NRS recorded on the medical records increased from 1.50±1.77 to 2.26±1.85, the patient-assessed NRS decreased from 4.28±2.04 to 2.52±1.59 after using the self-reporting pain board (Fig. 5).
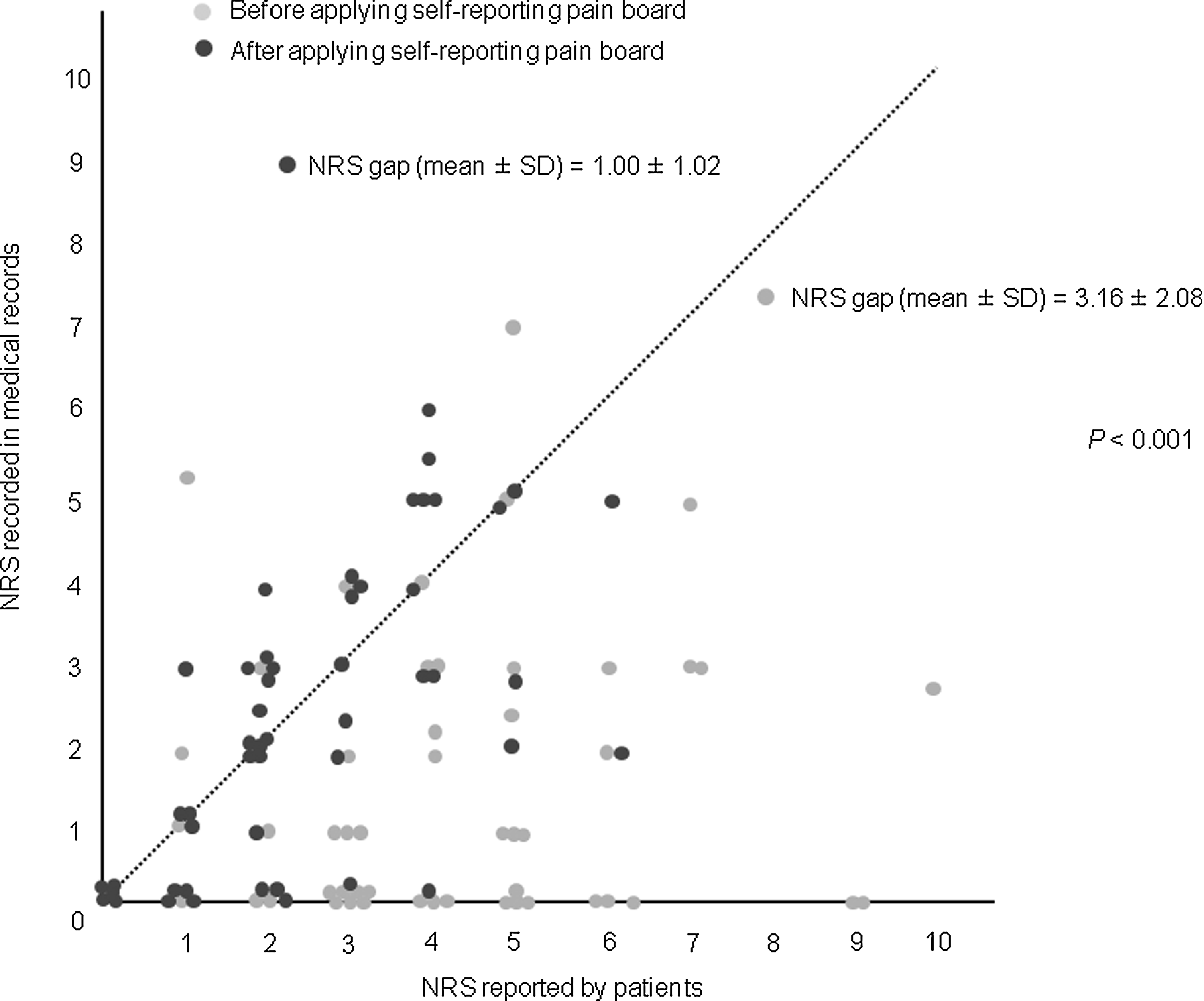
Numeric rating scales (NRS) gaps between pain scores reported by patients and pain scores from medical records.

Numeric rating scale (NRS) changes after using the self-reporting pain board.
The mean dose of morphine (mg/day/patient) used for continuous pain control increased from 79.5±167.1 to 99.4±199.3, although this difference was not statistically significant (p=0.580). The frequency of breakthrough pain stated in the medical records was also not significantly different (2.28±4.59 times before and 2.66±5.30 times after using the self-reporting pain board; p=0.702). However, the frequency of patient-assessed breakthrough pain recorded on the patient questionnaire decreased from 2.18±2.42 to 1.10±1.43 times (p=0.008). Four patients had a negative PMI before using the self-reporting pain board; however, PMI values were positive for all patients after using the self-reporting pain board.
Discussion
In this study, we found that a pain assessment system using a self-reporting pain board attached to the patient's bed provides a reliable and effective means of assessing pain. Of course, general pain education alone can play a role in changing patient perceptions and knowledge regarding cancer pain and painkillers, thereby improving cancer pain management. In a large-scale, prospective, cross-sectional cancer pain survey conducted in Korea between 2001 and 2006, the percentage of patients that reported a negative PMI was>40%. 18 In the present study, we educated patients regarding the general principles of cancer pain and pain management on the first day of study participation, and as a result, almost all patients had a positive PMI 3 days after admission.
However, suboptimal cancer pain management is common in the clinical setting and is believed to be related to a range of barriers that prevent good cancer pain management.19–21 One of the major barriers is the staff's failure to ask patients whether they are experiencing pain and to obtain a measurement of their pain intensity.19–25 A recent national survey of U.S. medical oncologists found that inadequate assessment of patient pain was the most significant barrier to pain management. 26 In clinical situations, the medical staff fail to spend sufficient time encouraging patients to accurately express the intensity of their pain and, occasionally, recorded pain intensities are estimated. For inpatients, the routine use of pain charts has considerably improved pain management; 27 however, according to several previous surveys of pain, a gap exists between the pain intensity recorded on medical records and the pain intensity perceived by patients.11–13 This situation arises because, unlike outpatient pain diaries, inpatient pain charts are recorded by nurses rather than by patients. Careceni and colleagues reported an improvement in pain assessment by having inpatients keep pain diaries 28 ; unfortunately, inpatients are often unable to keep pain diaries because they have poor performance status or acute problems in addition to pain. Therefore, an assessment tool is needed that allows inpatients to express pain intensity easily, actively, and frankly, thereby enabling the expressed pain levels to be transcribed accurately into the medical records.
The self-reporting pain board attached to the patient's bed used in this study allows patients to express pain intensity by moving an indicator. This significantly reduced the gap between the NRS recorded on pain charts and that actually perceived by patients (3.16 and 1.00, respectively). In addition to the direct expression of pain by patients, the self-reporting pain board offers other benefits. Because the board is always present at the bedside, it tends to increase patient interest in the scoring of pain. Accordingly, patients can communicate with the medical staff regarding their pain severity more frequently than they can when their pain is assessed by the medical staff intermittently at fixed times. Furthermore, as the self-reporting pain board is visible to medical staff, it stimulates their interest in patient pain and encourages active pain management. Furthermore, the self-reporting pain board can reduce staff workload with respect to pain assessment. The patients became familiar with the pain board very quickly and, as a result, they reported their pain scores voluntarily, with no encouragement from the medical staff. These benefits increase awareness and efficiency of patient-medical staff communication and ultimately increase patient satisfaction with pain management (from 54% to 82% in the present study).
The present study has several limitations. First, the control used in this study was the VRS (via oral inquiry). Recently, pain assessments are performed using self-reporting pain indicators in many medical institutions; however, these assessments are usually carried out by the medical staff and presented to the patient only when medical staff ask about pain. Therefore, comparing the self-reporting pain board attached to the patient's bed with the pain indicator carried by medical staff, which has become common practice for oncology inpatients, would have provided a more appropriate comparison. Second, patient education on cancer pain, the questionnaire given to both patients and staff, the self-reporting pain board itself, and the overall increased attention to pain management resulting from these practices could all have contributed to the improvement seen in this study. To minimize these effects and examine only the effect of the self-reporting pain assessment system itself, this study was designed to compare the same patient before and after the use of the pain board during the same period of hospital stay, with general education regarding the principles of cancer pain given only on Day 1 of study participation. Finally, the self-reporting pain board is not effective for cancer patients with very poor performance status or impaired cognitive function; particularly those under palliative care. Therefore, it may be necessary to devise a simpler and more reliable pain assessment tool for such patients.
Although the present findings were derived from a relatively small number of cases because of the limited number of available pain boards, we believe that the self-reporting bedside pain board is a reliable and effective instrument for assessing pain in cancer inpatients. The present study shows that this board improves cancer pain management considerably by reducing under-assessment of cancer pain by staff, narrowing the NRS gap between patient-perceived and medical staff-assessed pain severity, and encouraging both patients and medical staff to pay more attention to cancer pain and its management.
Footnotes
Acknowledgments
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MEST) (No. 2012-0000475).
Author Disclosure Statement
No competing financial interests exist.